
Abstract
Many individuals with mental illness want to return to work and stay in employment. Yet, there is little research that has examined the perspectives of employers on hiring and accommodating these workers and the kinds of supports employers need to facilitate their reintegration into the workforce. The aim of the current research was to explore the challenges employers face and the support they need to hire and accommodate workers with mental illness (WWMI). A qualitative research design guided by a grounded theory approach was used. In-depth interviews were conducted with 28 employers selected from a wide range of industries in and around Edmonton, Canada. The employers were a mix of frontline managers, disability consultants, and human resource managers who had direct experience with hiring and supervising WWMI. Data were analyzed using the principles of grounded theory. The findings highlight several challenges that employers face when dealing with mental health issues of workers in the workplace. These challenges can act as barriers to hiring and accommodating WWMI.
Research on the social determinants of health informs us that employment is a major determinant of mental health not only because it provides income but also because it affords people a sense of identity and purpose, social contacts and opportunities for personal growth (Harnois & Gabriel, 2000; Keon & Pepin, 2009; Raphael, Bryant, & Rioux, 2010). In the case of people with serious mental disorder, employment can provide a stepping-stone to recovery and there is increasing evidence that the ability to participate in employment enriches their quality of life and decreases disability (Ackerman & McReynolds, 2005; Becker, Drake, & Naughton, 2005; Morgan, 2005). Yet between 80% and 90% of individuals with serious mental disorder are unemployed, dependent on government pensions or on time limited allowances (Gilbride, Stensrud, Ehlers, Evans, & Peterson, 2000; Kirby & Keon, 2006; Krupa, Kirsh, Cockburn, & Gewurtz, 2009; McQuilken et al., 2003; Sanderson & Andrews, 2006; Secker & Membrey, 2003). This is unfortunate because most people with serious mental disorders desire to and can work (Bond, Drake, & Becker, 2008; Henry & Lucca, 2004; Liu, Hollis, Warren, & Williamson, 2007; Macias, DeCario, Wang, Frey, & Barreira, 2001; Morgan, 2005), but are excluded from the workforce because of attitudinal and structural barriers that prevent many from even gaining entry into the workforce. For those with mental illness who are in the workforce, there are issues related to sustaining their capacity for productive work. Currently, mental illness and addiction account for 60% to 65% of all disability insurance claims among Canadian employers (Dewa, Goering, & Lin, 2000; Goetzel et al., 2004; Kirby & Keon, 2006), while a more recent study estimated the overall economic costs of mental illness in Canada to be CAD$51 billion (Lim, Jacobs, Ohinmaa, Schopflocher, & Dewa, 2008). Whereas individuals with serious mental disorders need specialized vocational and employment services, those with mental illness who are already in the workforce need workplace interventions, accommodations, and counseling support to help them sustain employment. Currently, both groups face several barriers to gaining or sustaining employment. There is a critical need to improve employment outcomes for all individuals who experience mental health disorders and an increasing body of literature shows that employers can play a significant role in improving these outcomes.
Literature Review
Research to improve employment outcomes for people who experience mental disorders initially focused on understanding which people respond best to vocational interventions on the basis of individual, demographic, clinical, and social variables. However, few strong associations were found between these variables and employment outcomes defined variously in terms of job attainment, job retention, and number of hours worked (Anthony, 1994; Arns & Linney, 1993; Cook et al., 2005; McGurk, Mueser, Harvey, LaPuglia, & Marder, 2003). Contemporary conceptualizations have moved beyond individually focused models to understanding the employment of people with mental disorders as a dynamic process of interaction among several factors. These include the strengths, competencies, and needs of the worker, the nature of the job, and the demands of the work environment (Gilbride, Stensrud, Vandergoot, & Golden, 2003; Kirsh, Krupa, Cockburn, & Gewurtz, 2006). Other factors are inadequate vocational and clinical services, limitations of current disability support services, and legislation related to hiring and accommodating workers with mental illness (WWMI; Becker et al., 1998; Cockburn et al., 2006; Cook, 2006; Crisp, Gelder, Rix, Meltzer, & Rowlands, 2000; Goetzel et al., 2004; Granger, 2000; Liu et al., 2007; Murphy, Mullen, & Spagnolo, 2005). Increasing attention is now directed toward studying the demands arising from the work environment, particularly the role of employers in assisting people with mental illness to gain and/or sustain employment, maintain productivity, health, and well-being (Fabian, Waterworth, & Ripke, 1993; Gervey & Kowal, 1995).
Canada, unlike the United States, does not have a national disability policy. Human rights and discrimination against people with disabilities (and other social groups) in all areas including employment are governed by the number of Federal acts and programs. Prominent among these are the Canadian Human Rights Act (CHRA; 1977), the Charter of Rights and Freedoms (CRF; 1982), and the Employment Equity Act (EEA; 1986). The EEA, though limited in its jurisdiction to industries that are federally regulated, requires employers to engage in proactive measures to improve employment equity and opportunities for people with disabilities (Department of Justice Canada, 1995). In addition to Federal acts, each province has its own disability legislation and programs to improve employment equity and outcomes for people with disabilities. Although legislation may vary across provinces, employers have a legal duty to provide reasonable accommodations for workers with disabilities if and when they disclose their disability. Although human rights legislation prohibits employers from making direct inquiries into a prospective employee’s medical or mental health condition, they are allowed to ask objective questions that help determine whether a person can perform the essential duties of a job (Alberta Human Rights Commission, 2010). While an obvious physical disability is simple to detect and discuss accommodation for, mental health disabilities are hidden and workers are often uncomfortable confiding in their employer about these issues. However, if an employer has reason to believe that a worker may have a mental health condition based on their work behaviors they have a duty to inquire about the worker’s mental state and provide appropriate accommodations (Alberta Human Rights Commission, 2010). The province of Alberta, like other Canadian provinces, offers various levels of support to people with disabilities who wish to work or are working. The Alberta Employment First Strategy in particular aims to increase hiring and retention of workers with disabilities by providing resources and supports for employers and enhanced employment supports for persons with disabilities, including youth and mental health clients (Alberta Human Services, 2014).
Despite the existence of human rights legislation and programs to increase hiring and retention of workers with disabilities, many studies have consistently shown that people with disabilities face significant barriers particularly in the area of employment (Prince, 2010), a situation that also exists in the United States (Burns & Gordon, 2010). Some of the reasons for this include lack of knowledge and understanding among employers about the disability and what constitutes a reasonable accommodation, concerns around high accommodation costs and training time, attendance issues, attitudes of coworkers, discomfort during interviews and reduction in performance and quality levels (McCary, 2005). In the case of WWMI, these concerns are even more pronounced. Specific work-related concerns about WWMI include poor quantity and quality of work, brief tenure, absenteeism and low flexibility. Employers also hold beliefs that WWMI need excessive supervision, take little pride in work, have difficulty following instructions, are socially incompetent, and have low work persistence (De Waal, 2001; Diksa & Rogers, 1996; Johnson, Greenwood, & Schriner, 1988; Macias et al., 2001; Schriner, Greenwood, & Johnson, 1989). A recent Canadian study on stigma of mental illness defined five distinct assumptions held within the workplace that contribute to the disposition toward acting in a discriminatory manner: the assumption of incompetence, the assumption of dangerousness and unpredictability, the belief that mental disorder is not a legitimate illness, the belief that working is unhealthy for persons with mental disorders, and the assumption that employing these individuals represents an act of charity inconsistent with workplace needs (Krupa et al., 2009). Employees with mental health problems report that once their mental disorder becomes known they experience discrimination from coworkers, feel socially marginalized, have to cope with negative comments from workmates, and are forced to have to return to positions of reduced responsibility (Schulze & Angermeyer, 2003; Stuart, 2006; Wahl, 1999). WWMI are often fired when their psychiatric disability is revealed, and they encounter negative attitudes, behaviors, and comments by coworkers and supervisors (Stefan, 2002; Stuart, 2006). Even when in complete remission and in the absence of aberrant behavior, people with mental disorders often find that they are subjected to social discrimination and rejection (Thornicroft, 2006). Studies show that employers are largely uninformed about illnesses such as schizophrenia, and many believe that the condition is permanent or that the person has a split personality leading to the stereotype of the person being unpredictable and dangerous (Crisp et al., 2000; Foster, 2006). People who experience depression are often blamed for being emotionally weak or unproductive, although there is less stigma associated with depression than schizophrenia, especially in terms of violent episodes (Crisp et al., 2000). Surveys conducted in the United States show that approximately 70% of employers are reluctant to hire someone who is currently taking antipsychotic medication (Link & Phelan, 2001; Scheid, 1999), while almost a quarter would dismiss someone who had not disclosed a mental illness (Sartorius & Schulze, 2005). Also, WWMI are among the first to be retrenched in times of economic downturn (Stuart, 2006). In recent years, in Canada, there have been a growing number of educational programs, training workshops, and online resources that aim to change employer attitudes about WWMI and to increase their awareness about mental disorders in the workplace. In keeping with the employers’ needs (Cockburn et al., 2006 ; Hand & Tryssenaar, 2006; Kirby & Keon, 2006; Mizzoni & Kirsh, 2006; Strong, 1998; Tse, 2004), these programs also educate employers about their responsibilities as supervisors and provide skills to frontline supervisors/managers on dealing with performance issues of workers and crisis situations in case they occur. Noteworthy among these programs are Mental Health Works (www.mentalhealthworks.ca), and Workplace strategies for Mental Health initiated by Great-West Life Centre for Mental Health in the Workplace (http://www.workplacestrategiesformentalhealth.com). In the case of people who have serious mental disorders and intermittent periods of employment, there are an increasing number of employment placement providers who are funded to help these individuals find competitive employment in integrated work settings and offer ongoing support in keeping with the principles of supported employment (Bond, 2004; Bond et al., 2008; Xie, McHugo, Halliday, & Martinez, 2006). Often these service providers also provide guidance to employers on how to support and accommodate workers with mental-health-related disabilities.
Despite the importance and availability of such programs, there has been little change in employers’ attitudes toward hiring or accommodating WWMI (Stuart, 2006). There is a dearth of research that examines employers’ access to these resources, the practical challenges they experience on an ongoing basis when dealing with mental health issues in the workplace and the specific kinds of supports they need to hire and accommodate WWMI. In the current context, businesses are increasingly using employment practices that cut costs, such as encouraging casual and precarious employment, outsourcing, contractual arrangements, and organizational restructuring (Brun, 2007; Quinlan, 2007). Frontline managers are also under constant pressure to maintain the productivity of their units. Knowledge and information about employers’ understanding and experience with mental health issues at the workplace become particularly important in helping WWMI enter the workforce and retain their jobs. This current study aimed to examine the perspectives of a diverse group of employers on hiring and accommodating WWMI and the kinds of supports they will need. For the purpose of this study, “employer” refers to all those who play an active role in hiring, supervising, and supporting WWMI. The specific research questions were as follows: (a) What are employers’ perspectives on WWMI and related disability? (b) What are employers’ challenges and barriers to hiring and accommodating WWMI? (c) What kinds of supports do employers need to hire and accommodate these workers?
Method
This study employed a qualitative exploratory grounded theory approach to examine the research questions. In all, 28 employers from 27 business enterprises were interviewed. Consumer-run businesses were exempted from the study as they only employ WWMI and are governed by the principles of recovery and empowerment of persons with mental illness. The sample size was determined by the principle of theoretical saturation and maximum variation. This meant that sampling continued as long as new concepts kept emerging. The sampling was purposive as we wanted to capture the perspectives of employers who play an active role in hiring and supporting workers with disabilities, especially WWMI. The sample thus included 14 frontline managers, 4 human resource (HR) personnel, and 10 disability consultants/case managers from within the organization. Two employers reported that they had very little experience with WWMI. Table 1 provides the demographics of the employers in terms of the nature of industry and size of the organization. The majority of employers were from in and around the city of Edmonton in Western Canada.
Demographics of Employers by Industry, Interviewed Stakeholders, and Size of Organization.
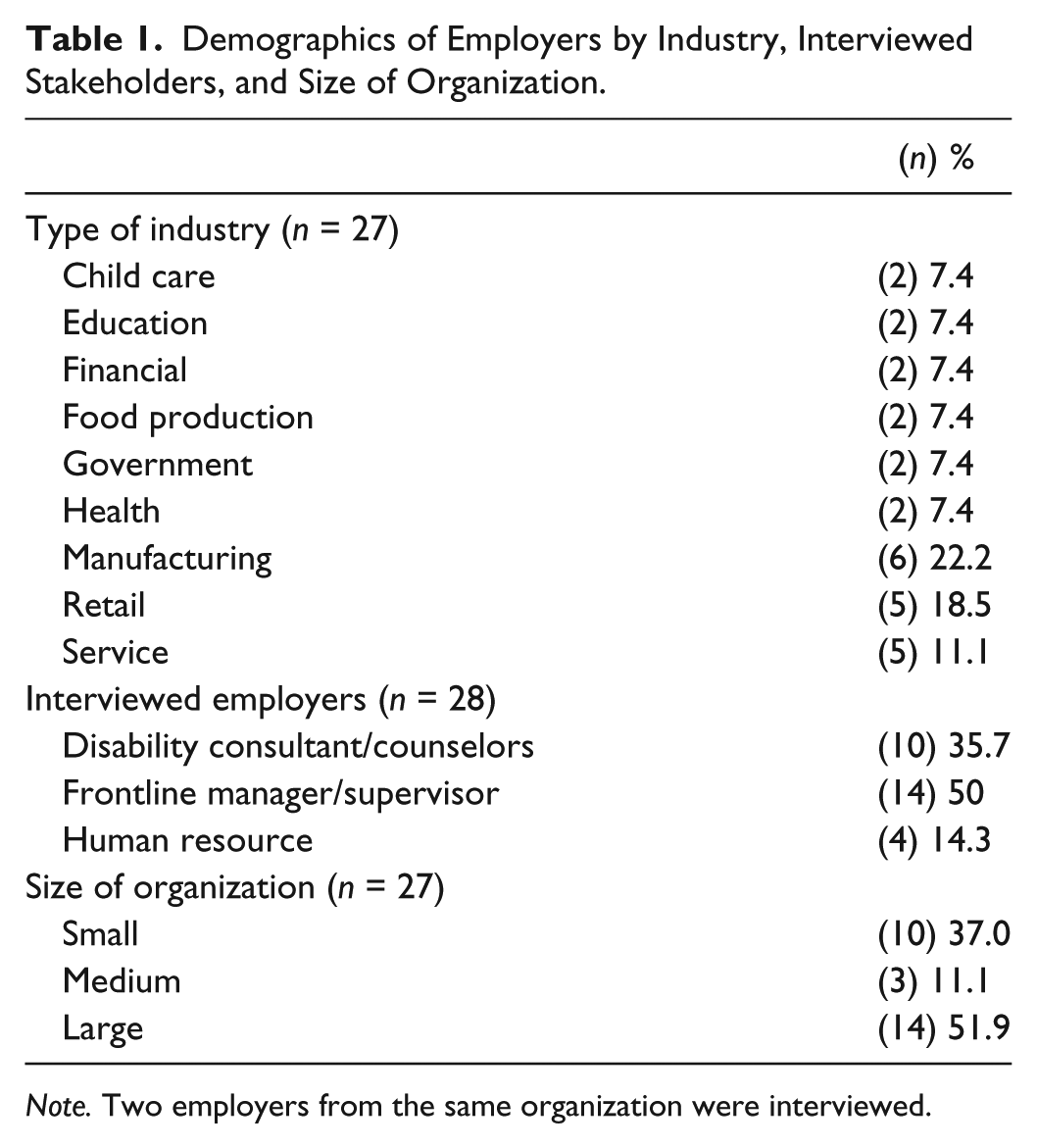
Note. Two employers from the same organization were interviewed.
Recruitment and Data Collection
The study was widely advertised to employers by our community partners through their daily contact with employers, study information clips in their newsletters, email information to employers about the study, information handouts and presentations at employer meetings. The researchers’ own contacts based on employer relationships from previous research were also used to recruit employers. Those who agreed and met the criteria for participation were contacted either by the first author or by a trained research assistant for arranging interviews. Except for five interviews that were conducted by phone, all interviews were face to face and were conducted at the employer’s offices. Data were collected through the use of semi-structured in-depth interviews that lasted for 1 to 1.5 hr each. Indirect questions were used to minimize social desirability bias (SDB) in responses.
Data Analysis and Rigor
With the consent of the participants, all the interviews were audio-taped and transcribed verbatim for coding and analysis. For data analysis, we used a constant comparative approach. It involved studying the data on a case-by-case basis, coding the data, analyzing the data across employers (in comparison), collapsing the initial codes into “categories of meaning” that represented themes (Charmaz, 2006). Based on the transcripts of the first few interviews, an initial coding framework was established. Two trained research assistants conducted independent coding of the interviews. The resulting codes were compared to ensure that the inter-coder reliability was achieved and maintained.
Rigor of the study was established by the following strategies: maintaining an audit trail of the research process, using data saturation, using inter-coder reliability, and peer debriefing. We also used several illustrative excerpts throughout the analysis process to add strength and authenticity to our analysis and the generated theory.
Results
Several key findings with themes and subthemes emerged from the data in response to the three research questions. The themes and subthemes under each research question are discussed below.
Employer Perspectives on Workers With Mental Disorder and Disability
Positive experiences
The majority of employers had some previous experience with people who had mental disorders. While three employers also had personal experience with the illness, some others had close relatives like parents or siblings who had disorders such as major depression and bipolar illness. Many employers had interacted with workers with mental disorders either in the capacity of facilitating their return to work or had worked with employment placement providers by offering their workplaces as training sites and supervising trainees with mental health disorders.
Many employers claimed that they had positive experiences with these workers. In response to an indirect question, “do you think businesses should hire and accommodate workers with mental health disorders,” the majority were in agreement. In fact, some employers said that they had hired trainees on work placement after a successful period of work training. For these employers, the work placement was their first experience of observing trainees with mental disorders in work situations and it had increased their confidence to employ these workers.
I’ve never had any challenges with anything like that—depression, anxiety, bipolar or schizophrenia. In most cases they’re on medication and so, um, they are—I don’t know what the proper medical term is, but they’re level, they’re centered. (Frontline manager who had worked with an employment placement provider) He was great. He got along good with the children and staff, did the job very well. I would have kept him as an employee but he chose to move on to something else . . . they (employment placement provider) would come out and visit and you know, um, talk to the employee, their person and talk to us. I’ve never really had a problem with any of the employees from them, they’ve been very good. (Line manager who had worked with an employment placement provider)
Negative experiences
Some employers however had negative experiences with some of the trainees on work placements. All of these were small employers with few resources to invest in providing supervision support to these trainees. Often, the trainees were young with little or no work experience. One of these employers felt that the trainees had been placed too quickly without adequate preparation to assume work responsibilities, while some others felt that as the trainees had mental illness they processed things slowly and exhibited poor work behaviors. Thus, for these employers, the placement had reinforced negative attitudes about WWMI. Table 2 provides examples of these employers’ impressions and the negative attitudes they reinforced.
Employer Impressions About Unsuccessful Placements.
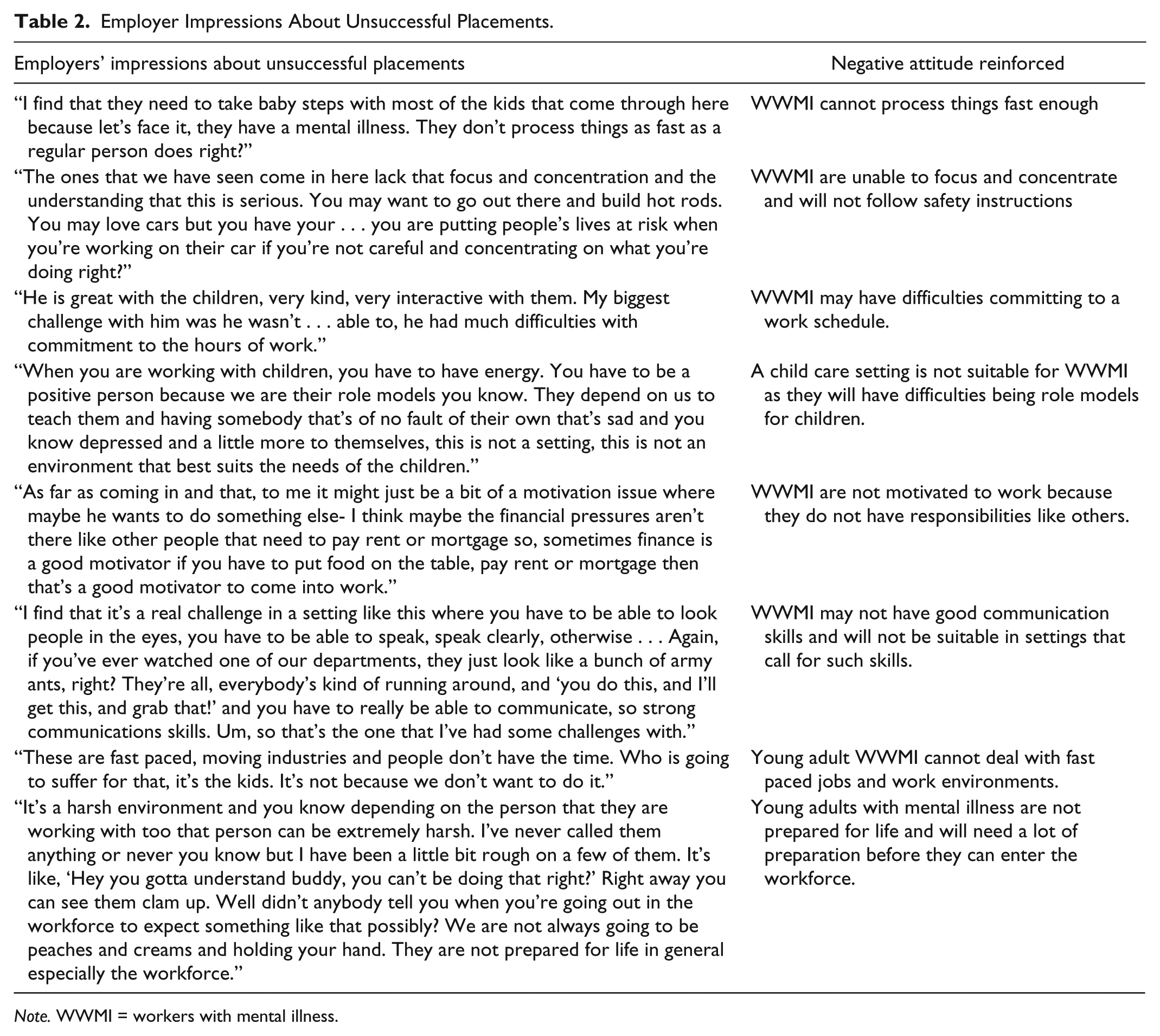
Note. WWMI = workers with mental illness.
Despite their negative comments, these employers stated that they would be willing to hire trainees with mental disorders and also accommodate them if they could demonstrate appropriate work behaviors, “right” work attitude, motivation to learn, and ability to do the job. This is illustrated by the following: I don’t see why not . . . you know what—if they are capable of doing a job . . . if they needed a few little special accommodations . . . Like I said if they needed to take five minutes out because they suffer from anxiety attacks or this and that . . . if the guy is on the floor working hard, constantly working and you can see he’s got it in him. He’s picking up things quickly. He’s got a good understanding, very helpful, here on time, doesn’t leave . . . I don’t see why not eh? (Manager in a small organization)
Causes of mental disorder and disability—Employer perspectives
As employers’ willingness to hire WWMI can be influenced by their perspectives on the illness, one of the first questions to them was aimed at exploring what they knew about mental illness and related disability. Employers were presented with a hypothetical vignette of a worker with a pseudonym John whose appearance, behaviors, and productivity in the last 4 to 5 weeks had been noted by coworkers to be in stark contrast with his usual. Employers were asked to comment on likely causes for these changes and how they would deal with the situation.
Although employers’ answers to the question varied, the majority said that worker John could be reacting to stress triggered by some events in his personal life like loss and grief, long-term caregiving demands or even torture and trauma experienced in the past. Some employers also cited anxiety, addiction issues, and depression as likely reasons for changes in John’s appearance and behavior. Only a minority of employers expressed that certain jobs and work environments could also trigger or exacerbate mental illness in some workers. These included shift work, entry-level employment, and performance-driven competitive work environments.
I don’t have the exact number, but more than 60% of us have problems at home. And I can give myself as an example, where my duties have led to a breakdown of my marriage, um, led to what I would call a dysfunctional in terms of my son now trying to find himself, and me becoming despondent, you know, and depressed enough to see a clinical psychologist. (Employer who currently holds a job as a senior administrator in a large organization highlighted the impact of the work environment and its demands on the home–work interface.)
Systems failing to support WWMI
Most frontline managers said that their first reaction toward the worker John would be to talk to him to gain firsthand information about what was troubling him and then discuss options for support depending on his needs. Disability consultants and HR personnel could identify some of the work-related difficulties that mental disorders could cause. These included frequent absenteeism, turning up late for work especially at the beginning of the week, and declining work performance.
In this context, some employers shared that the worker John would not get timely and appropriate support. Instead, he would be put on a performance plan and then terminated, if performance was still unsatisfactory: John would be called into the office and told that you know you’re not, you’re not measuring, you’re not meeting expectations of your position and so you know we, we want to help you, you know get, get to a point where you can manage all of your responsibilities, and that would be just a note documented in his file, and they’d give him probably 3 or 4 weeks to improve, failing that if he doesn’t improve and after that little discussion he may not, then it goes to a formal written letter of expectation, and it outlines the deficiencies and it outlines the expectations and sets a time frame for, for improvement. (Disability consultant who also experienced mental illness)
HR personnel and disability consultants commented that despite mental illness becoming increasingly common among workers little was being done by to address the issue. Workplace training that was very much needed to improve mental health literacy of frontline managers and other employees was sporadic and infrequent.
We’re seeing a lot more of it—I’d say more of the mental illness side versus the addictions side. I think the whole system fails people that have these impairments, you know from us as employers, from the medical system, the GPs, I don’t think as a society we’re dealing well with what seems to be a significant, if not an epidemic. (HR manager from a large corporation)
Challenges and Barriers to Hiring and Accommodating Workers With Mental Disorders
Despite their willingness to hire or accommodate, WWMI employers highlighted several challenges and barriers they faced in the process.
Lack of resources to address mental health issues of workers
Employers from small- and medium-sized organizations said that they may not hire workers who disclose mental illness because of a lack of needed resources such as HR department, staff trained to deal with mental health issues of workers, and time to dedicate to supporting workers who were unable to meet expectations because of their mental health problems.
Education about mental health is hard to come by—an organization may not have time or resources to dedicate to this area and currently, my organization only addresses such issues as they arise. (HR manager of a small/medium organization)
This placed WWMI, especially those in entry-level positions in a vulnerable position because if these workers were unable to meet expectations in the first 3 months, they would be terminated without considering whether a mental illness was an issue.
Productivity-driven focus
Employers also shared that because of the frontline manager’s overriding pressures and focus on productivity, it was difficult for them to look beyond the worker’s declining work performance. This often resulted in failure on their part to recognize early warning signs of declining performance due to mental illness.
Managers and supervisors, sometimes, they don’t have the foresight to look at it and say this is an issue that is performance based. The employee never shows up on Monday mornings, you know there’s a whole bunch of tardiness here, all of the signs, perhaps their performance was wonderful two years ago and its diminished to the point now where they’re on the verge of losing their job and I think for supervisors and managers it’s understanding the signs. I understand they have a job to do, they have production activities to do and they’re looking at it from a business sense and it’s very difficult sometimes for them to get down to the personal side of it. (HR manager from a medium-sized organization)
These employers also highlighted that failure on the part of frontline managers to recognize warning signs could result in turning the issue into a “performance conversation with the worker.” This could lead to further deterioration in productivity to a point where the worker would be terminated. Some frontline managers confided that they lacked guidance on how to strike a balance between obligations to help versus having a healthy business, and balancing employees’ needs versus employers’ needs.
Managers are not mental health professionals
In the context of recognizing warning signs, some frontline managers shared that this was not their job as they were not trained as mental health professionals. As commented by one employer, Employers are managers and we are not trained to deal with people with mental illness. (Frontline manager of a large firm)
Some employers who had experience of mental illness said that sometimes even the WWMI and their treatment provider were unable to recognize early warning signs of a relapse, so how can the supervisor, who had little or no training in mental health be expected to recognize these signs.
Worker must take more responsibility to save his or her job
An important point that was raised specifically by some frontline supervisors and HR managers was the failure on the part of workers to let their supervisors know about the warning signs of a breakdown and take more responsibility to help themselves. Often, they hid the illness or tended to deny it and kept going until they were reprimanded or were pulled up for performance issues.
I predominantly work with a male work force. T—these guys keep going and going and don’t realize you know perhaps they’re depressed or facing life issues until they really enter the point where they can’t function, because guys just don’t know when and how to reach out for help. (HR manager of a large firm)
The above excerpt also suggests perceptions of gender differences among WWMI.
Poor coordination and communication among service systems
Unlike small and some medium-sized firms, large organizations had several resources such as HR personnel, in-house disability case mangers/consultants, and employment assistance providers (EAPs) to support workers with mental health issues. Many disability support providers and HR personnel stated that frontline managers had access to education programs conducted by EAPs, wellness providers and HR departments, online resources, videos, and consultation services. Despite the availability of such resources, some frontline managers shared that many of their practical concerns were rarely addressed by service providers who included HR managers and disability case managers/consultants. Their concerns were around issues like how the worker’s illness was going to affect them as the manager, how the illness was going to affect other colleagues, whether there were any limitations or restrictions, whether there were any side effects of medications that they should know about, whether the WWMI was accessing appropriate treatment, and whether they were capable of getting the work done. Frontline managers expressed their frustrations about not getting any information on the above issues from HR departments, disability service providers, or doctors. They reported that these issues were important for them because they had implications for allocating resources in their respective departments. Often in large organizations, frontline managers were paying out of their unit funds for the medical treatment of the employee and also had to pay an alternate employee to cover for the sick employee’s missed work. Some frontline managers commented that they were not aware about the range of programs that were available through their organization for employees who experience mental health disorders and sometimes they found out about these by chance or after a crisis. The following excerpts illustrate the frustration and isolation that some of these managers experienced.
Doctors’ notes are notoriously useless actually, they’re pretty bad. They’re not specific enough, they don’t—uh, they certainly don’t give you any reasons . . . We are not allowed to contact the doctor—and have any communication with them—you’re never really told, and you’re not allowed to ask—you can’t share any information with any of the other staff. I . . . I think I would have wanted a better communication. (Department head of a large organization) I would have wanted our disability case manager for example, to facilitate a more open dialogue as to—what’s going on. There has to be a level of trust if you’re going to continue to—work in a particular environment, right? I think the case manager could have facilitated, even if it is just to explain . . . this is the reason we can’t share certain information, or she doesn’t want to . . . it was this grey zone where nobody dared touch the conversation and it was always on her. (Employee’s terms too; unit frontline manager of a large organization)
Prejudice and discrimination—An ongoing challenge
Employers agreed that people react to stress in different ways and that those with mental disorders should be treated like any other worker and receive the same kinds of accommodations and supports as workers with physical disabilities. They were aware that prejudice and discrimination played a major role in how WWMI were treated. Some employers blamed the media for propagating beliefs that mental illness is a weakness and that WWMI are dangerous, lazy, and cannot pull their weight. These beliefs are still widely prevalent in workplaces. Employers who had negative experiences with some WWMI confided that it was hard for them not to be influenced by the media on widely prevalent presumptions and stereotypes. As described by one such employer, Let’s be honest. There’s society that puts it in our head-right? . . . I if this guy’s got a mental health issue, yeah, a—I’m going to be watching him with the corner of my eye. When a guy goes on the Greyhound Bus and cuts people’s heads off, that person had a mental health issue too. Nobody knew about it. It’s society that drills it at least in my head that you gotta keep an eye on this person. Don’t let your guard down regardless. That’s the way I look at it. (Frontline manager of a small firm)
Another employer who had no experience with WWMI raised an important concern about the lack of information and knowledge about recovery from mental disorder and specifically what this means in the context of work: Employers need to know about success rates or how well we are doing at getting these people back to work, back to—back into society and totally functional and normal, and normal in society’s eyes. (HR person from a medium-sized firm)
Support Needs of Employers
In addition to the challenges faced when hiring and supervising WWMI (Table 3), employers also expressed some specific needs. Employers who had more in-depth knowledge of mental disorders, having experienced it themselves or in their relative said that they would be willing to hire, but would need more information about the worker’s present state of recovery: Regarding hiring persons with MH issues—Well the short answer is yes, and, if again we’re talking about someone who’s had you know a mood disorder I’d be more reluctant- as someone who’s had a psychiatric condition, I’d need to know a little bit more about what that’s about. Regarding hiring persons with addictions—Well if they’re in recovery, their recovery has been successful . . . I don’t see that as a huge problem. If they’re still actively using no I wouldn’t. (Disability consultant in big firm)
Challenges and Barriers to Hiring and Accommodating WWMI.

Note. WWMI = workers with mental illness.
Safety at work was an important consideration for all employers. While they acknowledged the importance of confidentiality, employers wanted assurance from the worker or their employment placement provider that they had been certified as medically fit to work. If the worker was on medications for the disorder, employers wanted to know if these would have any side effects that could affect their ability to perform their jobs safely. Dealing with crisis was another area that employers, especially from small and medium-sized firms, were particularly concerned about. They were willing to hire WWMI but wanted guidance and advice on what to expect and what they should do (or not do) in the event of a crisis, including how to prepare other staff. Finally, all employers emphasized that they would be willing to hire and accommodate WWMI as long as it was cost-effective and the business would not suffer. The following excerpt from a frontline manager in a small firm captures these employers’ views.
It sounds kind of heartless to say it, but at the end of the day the business does kind of have to come first. Same deal though with any other employee. If a perfectly normal, uh, well not normal but a person without mental illness isn’t doing his job either, I mean, he’s going to get fired too. (Frontline manager who also experienced a mental disorder)
Discussion
This study expands our understanding of employers’ perspectives on hiring and accommodating WWMI and the challenges they face in this process. The employers were a diverse group with varying levels of experience with WWMI and worked in a variety of roles and contexts. A key finding that is contrary to previous findings is that 85% of employers agreed that their organizations should hire and accommodate WWMI. We do acknowledge that some employers may not have been entirely truthful in stating their objections to hiring and/or supervising these workers due to SDB (this was minimized by asking an indirect question: “Do you think businesses should hire and accommodate workers with mental disorders?”). Nevertheless, our interviews strongly suggest that employers who have previous and positive experiences with WWMI or have worked with employment placement providers have less prejudicial attitudes toward hiring and accommodating these workers. These findings complement findings of previous research (Brockington, Hall, Levings, & Murphy 1993; Kirsh et al., 2006; Shankar & Collyer, 2002). However, the minority of employers who reported having very little experience with these workers said that they would need more information about mental illness. Employers who had negative experience held on to beliefs that these workers may not be competitive enough or reliable.
Although the majority of employers attributed the causes of mental disorder to personal factors outside the workplace, it is interesting that some recognized the role of the working environment in creating or perpetuating the illness. This is in keeping with burgeoning evidence that mental health problems are often integrally related to factors arising from the working environment such as work overload stress, perceived lack of control over work, poor work environment, stigma and discrimination in the workplace, difficult colleagues and supervisors, frustrations around career development, perceived injustice, the impact of oppressive organizational culture and norms, and dilemmas in balancing the home–work interface (Greenberg, 2010; Krupa et al., 2009; Shankar, Barlow, & Khalema, 2011). When employers (including management) attribute the cause of the disorder mainly to personal factors and ignore the importance of the working environment, the onus for change is placed solely on the worker. While this may relieve employers of the responsibility to make changes to the working environment, it can also make it difficult for them to access resources and support from their organization when they are faced with the challenge of accommodating WWMI. Current disability support service systems including EAPs and HR personnel must aim to provide a more holistic service that addresses the needs of both workers and their managers.
The findings identify several challenges employers experienced and suggest that despite their willingness to hire and accommodate WWMI, related decision-making is influenced by the resources they can access, the supports they have, and the quality of the support they received based on previous experiences. Figure 1 highlights the factors that are likely to shape an employers’ decision to hire WWMI. This figure shows that while employers may be willing to hire individuals with mental illness, several other factors are also instrumental in their ultimate decision to hire and accommodate them. Employers who do not have easy access to information about mental illness, lack support services at the workplace, or have previously not felt adequately supported by service providers may not hire and accommodate WWMI even if they are willing to do so.

Willingness to hire versus decision to hire.
These findings underscore the importance of assessing and addressing the support needs of employers, especially frontline managers. Some disability service providers and HR personnel in this study reasoned that frontline managers had access to a growing number of innovative education and training workshops, videos, and online resources to increase their understanding of mental illness as they play out in the workplace. Nevertheless employers are a diverse group with varying levels of knowledge and experience about mental health issues. As indicated earlier, their capacity to access available resources will depend on the context in which they operate, the time and productivity pressures they are under, the commitment and capacity of their management to invest in educating staff about mental health issues of workers and their previous experiences with disability support providers/support systems, employment placement providers, and treatment professionals.
The findings related to negative perceptions of some employers about the work behaviors and attitudes of trainees with mental health issues who were placed in their firms may serve as barriers to hiring WWMI. However, some of these behaviors may not be due to mental disorder but the result of a lack of fit between the employers’ expectations, the training environment, and job match. The findings of this study have implications for practices of disability support providers, HR personnel, employment placement providers, EAPs and treatment providers. The following section discusses some recommendations based on the findings.
Periodic In-Service Training to Improve Mental Health Literacy in the Workplace
As noted by many employers, prejudice and discrimination toward WWMI continue to be rife in workplaces. This needs to be addressed systematically and aggressively if these workers are to be hired and accommodated. The fear of discrimination is one of the main reasons why workers do not wish to disclose mental health disability (Russinova, Griffin, Bloch, Wewiorski, & Rosoklija, 2011). From a business perspective, it makes better sense for management to invest in supporting and accommodating a well-trained worker rather than incurring the cost of disability due to mental illness. Management must therefore ensure that periodic in-service training for improving mental health literacy is available for frontline managers and other employees. This can help keep mental health issues in focus and increase the probability that performance difficulties due to mental disorders are identified early and addressed. Such training can also promote understanding that mental health problems and difficulties are not permanent states. Along with awareness about early warning signs of declining performance due to mental disorder, discussing performance with an employee with the disorder, and developing a trusting working relationship, it is important for frontline managers to be educated on how to create and maintain a healthy workplace environment. In such environments, workers who experience disabilities due to mental illness can feel safe to disclose and are less likely to be subjected to a different set of behavioral expectations than their peers. In the case of organizations that do not have the resources for periodic in-service training but are willing take on trainees with mental health problems, the employment placement providers could provide these services.
Individualized Support for Employers Who Hire and Accommodate Workers With Mental Illness
The diversity among frontline managers (and also WWMI) calls for an individualized approach to support managers that is in keeping with their work context and needs. The findings of this study suggest that there can be a disconnect between the kinds of information and support the frontline manager wants to accommodate a WWMI and the service provider’s perspectives on what the manager needs. If the return to work of the employee or hiring a WWMI is to be successful, disability service providers, including HR personnel or employment placement providers, must work closely with the manager to understand their working context, demands, and pressures, their concerns about the worker’s disability and its likely impact on work performance. The frontline manager must be involved in the development of the return to work plan and the accommodations that may be needed. There must be periodic follow-up by the disability service provider to ensure that the return to work is progressing well and he or she must be easily accessible to the manager for consultation. The added benefit of providing such individualized support is that managers may be more amenable to identifying and altering workplace conditions to suit the needs of the worker as well as other employees.
Improving Communication and Collaboration Among Service Systems
The findings also suggest a broader issue related to developing best practices for improving communication and collaboration among the different stakeholder groups serving the WWMI and promoting understanding about what each one is providing and the range of services that are available. Depending on the organization, these stakeholders may include frontline managers, HR personnel, disability service providers, employment placement providers, EAPs and treatment providers. As suggested by HR personnel, General Practitioners with the consent of the WWMI must provide information on what the worker can do, their abilities and limitations, while the EAP/wellness case manager, HR and frontline manager must be involved in developing a collaborative Return to Work (RTW) plan. This collaborative approach can help increase the supervisor’s confidence to engage with the RTW process for the WWMI and also alleviate concerns that they do not have mental health training.
Achieving the Right Job Match and Assessing the Work Environment for Trainee Workers
Job match refers to the degree to which a given job matches the interests, values, and competencies of the worker (Kukla & Bond, 2012). There is evidence suggesting that achieving a proper job match for people with mental disorders who are working competitively and receiving employment support services is associated with higher job satisfaction and longer job tenure (Becker et al., 1998; Mak, Tsang, & Cheung, 2006; Resnick & Bond, 2001). Employment placement providers must therefore aim to achieve a proper job match for the trainee worker as failure to do so can result in job dissatisfaction and dropout. In the case of individuals who have a poor work history or lack work experience, achieving a proper job match can be challenging and may require more than one placement. The training environments for these individuals must be supportive and selected after a thorough assessment of the resources they have to support the trainee’s learning needs. Placing trainees with employers who do not have these resources may result in trainees losing confidence and motivation, and ultimately dropping out of placement. As suggested by the findings, this can reinforce negative attitudes among employers that WWMI are slow learners and lack initiative, commitment and responsibility. To minimize the risk of placement failures employment placement providers who are in the process of helping the trainee to find the right job match must develop partnerships with employers who value diversity in the workplace and are willing to take a little extra time to understand the unique needs of a potentially effective and productive employee.
Limitations
A limitation of this study is that the findings are based on a small sample of 28 employers drawn largely from the city of Edmonton in Western Canada and therefore may not be applicable to employers from other regions or countries. In addition, as the majority of participants were selected on the basis that they had some previous experience with workers who experienced mental health issues, the findings may not apply to employers who have no previous experience with these workers. Future studies should focus on larger samples and include employers who do not have experience with mental health issues as their perspectives and challenges may be very different. Future research can also examine the perspectives of employers who work with employment placement workers to provide supported employment services for individuals with severe mental disorders and developing best practices for improving these outcomes.
Conclusion
Despite the limitations of the study, the findings are significant and add to a growing body of knowledge on employers’ perspectives on hiring and accommodating workers with mental health issues. The challenges that employers face underscore the importance of understanding their practical concerns and addressing their needs for education and support in a timely and efficient manner. Addressing these challenges has the potential to remove a major barrier to the entry and reintegration of WWMI into the workforce and further serves to improve their overall work experience.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This study was funded by Alberta Health Services, Canada