
Abstract
The objective of this article is to define the underlying dimensions of psychosocial barriers to obtaining and providing dental care for young children among recent immigrants. Fifteen focus groups were conducted with 99 primary caregivers from African, South Asian, and Chinese recent immigrants. A secondary analysis of identified barriers using dimensional analysis methodology was performed to determine dimensions and properties of barriers. The analysis continued until irreducible properties were found or emerging dimensions were not relevant to the study. Identified dimensions were associated with barriers and individuals. Type, number, level, objectiveness, nature, and impact were barrier-related; awareness and controllability were individual-related dimensions. Type refers to barriers themselves. Number and level indicate the amount and location of barriers, respectively. Objectiveness refers to the extent that perceived barrier reflects reality and nature indicates its intrinsic characteristic. Impact concerns behaviors, goals, and outcomes compromised by barriers. Awareness alludes to the extent that individuals are aware of the barriers and controllability explains how much control people perceive to have over barriers. Identified dimensions are useful for better understanding and addressing existing barriers to children’s optimal oral health.
Introduction
Two contrasting realities coexist in oral health. While the most common oral diseases are preventable and treatable (Dubay, Parker, & DeFriese, 2005); a large number of individuals still suffer from their physical, psychological, social, and economic consequences (Edelstein, 2002). Oral diseases and their consequences are not equally distributed, but concentrated in vulnerable segments of the population, including low-income individuals, immigrants, ethnic/racial minorities, and young children (Watt, 2007). Although the prevalence of caries decreased in schoolchildren in the last three decades, a 15% increase was found in children below the age of 6 (Kagihara, Niederhauser, & Stark, 2009). Canadian surveys have shown that children from immigrant families experience more dental diseases and are less likely to receive professional dental care than their Canadian counterparts (Locker, Clarke, & Murray, 1998; Werneck, Lawrence, Kulkarni, & Locker, 2008).
These contrasting realities mainly result from the impact of psychosocial barriers. Studies conducted in the United States and Canada have consistently indicated lack of dental insurance, low acceptance of public dental coverage, high cost of dental services, lack of transportation, low priority to oral health, no perceived need for dental care, dental fear and anxiety, and shortage of dentists as noticeable barriers to dental care (Hilton, Stephen, Barker, & Weintraub, 2007; Mofidi, Rozier, & King, 2002; Newbold & Patel, 2006; Vargas, Monajemy, Khurana, & Tinanoff, 2000). Self-dental care, including parental care of children’s oral health, is also affected by psychosocial barriers, although this care is more likely to be influenced by ethnicity-related factors than by environmental constraints (Gao et al., 2010).
Studies on barriers to optimal oral health have become popular in the dental literature. This secular interest contrasts with a very superficial analysis of barriers usually limited to the recognition of factors that hinder the performance of oral health behaviors and the accomplishment of desired oral health outcomes. Barriers themselves have scarcely been examined. Even the concept of barrier is rarely defined in most of the studies on this topic. Thus, barrier seems to be seen as a self-explanatory concept with no dimensions other than the type of impediment preventing study populations from accomplishing certain health outcomes.
Barriers can be examined in relation to behaviors or goals. Theories of health behavior such as the Health Belief Model (Becker, 1974), Theory of Planned Behavior (Ajzen, 1991), and Social Cognitive Theory (Bandura, 1982) have mainly focused on the first type of analysis. In these models, barriers and the perceived control over them are thought to influence behavior directly by impeding its performance and indirectly by discouraging individuals from taking action.
In the Behavioral Model (Andersen, 1995), instead, barriers are examined with respect to access to health services, which encompasses numerous behaviors. In this model, barriers are seen as individual, family, and community factors that impede the use of services believed to be also determined by predisposing and need factors. Empirical research in dentistry has adopted a broader view in which barriers are considered as any factor preventing individuals from both utilizing dental services and having optimal oral health. From this perspective, no perceived need for dental services and dental beliefs, viewed as predisposing factors in the Behavioral Model, are also considered barriers.
For such a level of inclusiveness to have conceptual and practical value, dimensions of barriers need to be defined. Otherwise, the identification of barriers may become a mere list of factors to be handled to improve utilization of dental services and, ultimately, oral health outcomes. The medical and dental literature lacks a conceptualization of barriers, even though barrier has been consistently reported as one of the strongest predictors of health behaviors and outcomes (Conner & Norman, 2005). This study aims to bridge this conceptual gap examining dimensions underlining psychosocial barriers to prevention of early childhood caries (ECC) among children of recent immigrant families residing in Edmonton, Canada.
Materials and Method
Design
University of Alberta Research Ethics Board provided the ethics approval for the study, which is a secondary analysis of psychosocial barriers to prevention of ECC among immigrant parents, identified over the course of 2-year period. Psychosocial barriers affecting parents from Northeast African communities have been previously documented (Amin & Perez, 2012). For the recognition of barriers, a normative view was adopted, which allows us to identify them regardless of the individuals’ awareness of barrier and with respect to normatively defined dental behaviors, goals, and outcomes. The study was framed within the dimensional analysis methodology, which provides principles, procedures, and operations for developing a grounded theory of a social phenomenon (Schatzman, 1991).
Participants
A purposive sample of immigrant parents from African (Ethiopia, Eritrea, and Somalia), South Asian (India, Pakistan, and Nepal), and Chinese communities was selected. Participating parents had lived in Canada for 10 years or less, had at least a 2- to 5-year-old child, were permanent resident or citizens, and perceived themselves as a member of the target communities. The study focused on immigrant parents because of the prominent role they play in their young children’s oral health and the additional challenges they face to provide them with optimal oral health care (Mouradian, Huebner, Ramos-Gomez, & Slavkin, 2007). Ninety-nine immigrant parents in total were recruited via advertisements, community activists, and settlement agencies with which the researchers have long-standing partnerships. Recruitment strategies were developed based on the input of experienced front-line community workers.
Data Collection
Focus groups were conducted to determine psychosocial barriers to prevention of ECC among immigrant parents and the dimensions underlying them. Trained facilitators conducted the focus groups in participants’ first language, which lasted approximately 2 hr. Conversations were recorded and transcribed verbatim. In each focus group, participants completed a brief questionnaire on demographics (age, educational attainment, ethnicity, income, number of children, time lived in Canada, and status) and dental history of the child. Dental history included means and frequency of dental cleaning, main cleaner, independent cleaning, frequency of sugar intake, last dental visit, and reasons for and for not seeking dental care. Question asked in the focus groups concerned the concept of oral health, perception of ECC, value of primary dentition, perceived oral health status, measures to prevent dental diseases, reasons for dental attendance, attitudes toward dentists and dental services, perceived role/responsibility of parents and dentists, and barrier/challenges to prevention and treatment of dental diseases. Probing questions about each of these topics were also asked when necessary to add depth to the answers. Additional focus groups were conducted to expand salient dimensions and sub-dimensions of identified barriers. Field notes and theoretical memos were analyzed as a source of additional data. Data were collected until a critical mass of dimensions, sub-dimensions, and properties of barriers were assembled, and no new significant component of the study phenomenon emerged from data.
Data Analysis
Data analysis was conducted according to dimensional analysis methodology, which encompasses three main stages: dimensionalizing, differentiation, and integration (Kools, McCarthy, Durham, & Robrecht, 1996). As the study aimed to examine the underlying dimensions of barriers, data analysis was centered on the first stage in which salient dimensions and corresponding properties of the study phenomenon are identified. A dimension is an abstract concept representing a component of a social phenomenon, whereas a property is a quantitative or qualitative descriptor of a dimension (Kools et al., 1996). Salient dimensions and corresponding properties represent the building blocks of an in-development grounded theory.
Dimensionalization of identified barriers consisted of identifying and labeling features of barriers without consideration of their importance, meaning, or status. Relevant features of barriers became dimensions that were further expanded into sub-dimensions and quantitative and qualitative properties. Some qualitative properties were also expanded into a new set of dimensions and respective properties. Two forms of comparison were used to determine dimensions and properties: comparisons between events representing features of barriers and between events and assigned codes or labels. Differences between these two forms of comparisons indicated new features (dimensions and properties) of barriers. The analysis continued until irreducible properties were found or emerging dimensions were not relevant to the study. The expansion of each dimension depended on its internal density.
Studies aiming to explain a social phenomenon using dimension analysis also differentiate and integrate identified dimensions. Dimensions are differentiated by choosing the dimension with the greatest explanatory power, also called perspective. Dimensions are then organized around the chosen perspective according to which they may acquire the status of context, conditions that block or facilitate actions, actions themselves, and consequences of actions. The emerging framework is later integrated by challenging its explanatory power with new data and alternative accounts (Kools et al., 1996).
Results
Identified dimensions were classified into two groups: barrier-related and individual-related dimensions. Type, number, level, objectiveness, nature, relationship, and impact were barrier-related dimensions. Awareness and controllability were found to be individual-related dimensions.
Barrier-Related Dimensions
Type refers to the specific barriers preventing individuals from accomplishing self-defined or normatively defined goals. Thus, this dimension indicates what the barriers are. Several barriers were identified in the study. Some have been extensively reported in previous studies such as lack of insurance or ability to pay, transportation, social support, and no perceived need for dental services (Hilton et al., 2007; Mofidi et al., 2002; Newbold & Patel, 2006; Vargas et al., 2000). Other barriers including being overconfident in detecting ECC, defining optimal oral health as absent of dental symptoms, perceiving the identity of ECC as a black spot or a hole on a tooth, and reducing the role of dentists to fixing problems and the role of parent to seeking dental care when a problem arises have been documented to a lesser extent.
Number concerns the amount of barriers affecting the performance of dental behaviors or the accomplishment of dental goals. Level indicates the location of barrier in a factorial structure. Properties of this dimension were individual, family, community, and systemic level. Lack of English skills to either make dental appointments or communicate with dentists was deemed as an individual barrier, while lack of family support and limited dental insurance for needed dental services were barriers at family and systemic level, respectively. Objectiveness defines barriers as either real or self-created, these two being the main properties of this dimension. In our study, some barriers were misperceptions and as such self-created impediments to accomplishing oral health outcomes. The misperceptions that only jobs provide dental insurance and that the Alberta Child Health Benefit does not cover dental services represented self-induced barriers to access to dental services, as they do not reflect reality.
Nature refers to the character of the barrier under consideration. Its salient properties were skills, knowledge, attitude, perceptions, values, norms, and constraints. These qualitative properties were also expanded, but results are not presented in this article as the resulting set of sub-dimensions and properties were not relevant to the purpose of this study. Some of the skill-related barriers were lack of skills to assist children in toothbrushing and difficulties in communicating with in-front staff and dentists. Limited knowledge of preventive dental measures and available dental insurance for low-income families were among the identified knowledge-related barriers. Unfavorable attitudes toward dentists and dental services were seen as attitude-related barriers. Perceiving dentists as repairers and assuming that children are ready to brush their teeth independently at the age of 3 represented perception-related barriers. The value placed on, for instance, treatment over prevention, permanent teeth over primary teeth, dental appearance over dental function, became value-related barriers. Flossing and preventive dental visits were not normative practices among African families in this study. Consequently, they were recognized as norm-related barriers. Lack of time, transportation, and insurance were among the identified constraints to access to dental services. Limited social capital of immigrant parents was viewed as another constraint affecting their children’s oral health.
Relationship concerns the linkages between barriers (Figure 1). It refers to how barriers affecting a given outcome or goal are connected. The analysis of identified barriers showed that outcomes and goals are often compromised by more than one barrier and that compromising barriers may be related. Three sub-dimensions were associated with relationship between barriers: number, barriers involved, and type. Number and barriers involved indicate the amount and the specific barriers compromising the outcome/goal being considered. Type indicates the character of the relationship between barriers. Two types of relationships were identified representing the properties of this sub-dimension: dependent and independent. A dependent relationship was observed when some barriers seemed to act as a condition for others to exist. For example, believing that only jobs provide dental insurance, unawareness of existing public dental insurance for low-income families, and perceived or actual inability to do the paper work required to apply for public dental insurance led some participants to be uninsured, which in turn influenced their access to dental services. Barriers had an independent relationship when they influenced the same outcome/goal directly and not through other barriers. Perceiving that dentists only treat dental problem and parents’ overconfidence in detecting caries in primary teeth were two barriers that affected early detection of caries independently.

Dimensionalization of relationship.
Impact concerns the consequences of barriers (Figure 2). Object and scope were the salient sub-dimensions of impact. Object indicates what is compromised, which was dimensionalized into type of care, behaviors, stage of the process, and goals. Type of care was in turn expanded into at-home dental care and professional dental care. Some barriers like lack of skills to properly assist or supervise children in toothbrushing affected at-home dental care, while unfavorable attitudes toward dentists and lack of awareness of existing public dental insurance affected professional dental care. Some barriers including the concept of oral health, limited knowledge of preventive dental measures, and time constraints negatively influenced both professional and at-home dental care. Barriers also compromised the performance of specific behaviors like regular dental visits, tooth flossing, and control over child’s sugar intake, which in turn compromised the achievements of oral health goals such as prevention of ECC, early detection of ECC, and timely dental treatment. Barriers also affected different steps of the process of seeking dental care. The perceived need for dental care, a necessary condition for dental services to be sought, seemed to be affected by barriers such as being aware of a serious dental problem as the primary trigger for seeking care, unawareness of existing caries, and a perception of caries which represent advanced tooth decays. Once the decision of seeking care was made, another set of barriers including lack of English skills, transportation problems, and low-self efficacy to manage access-related challenges seemed to affect its implementation. The scope of the impact of barriers was dimensionalized into two main properties: individuals being affected and issues being compromised by barriers. Some barriers affected a few individuals and very specific behaviors and outcomes, while others had a broader impact.
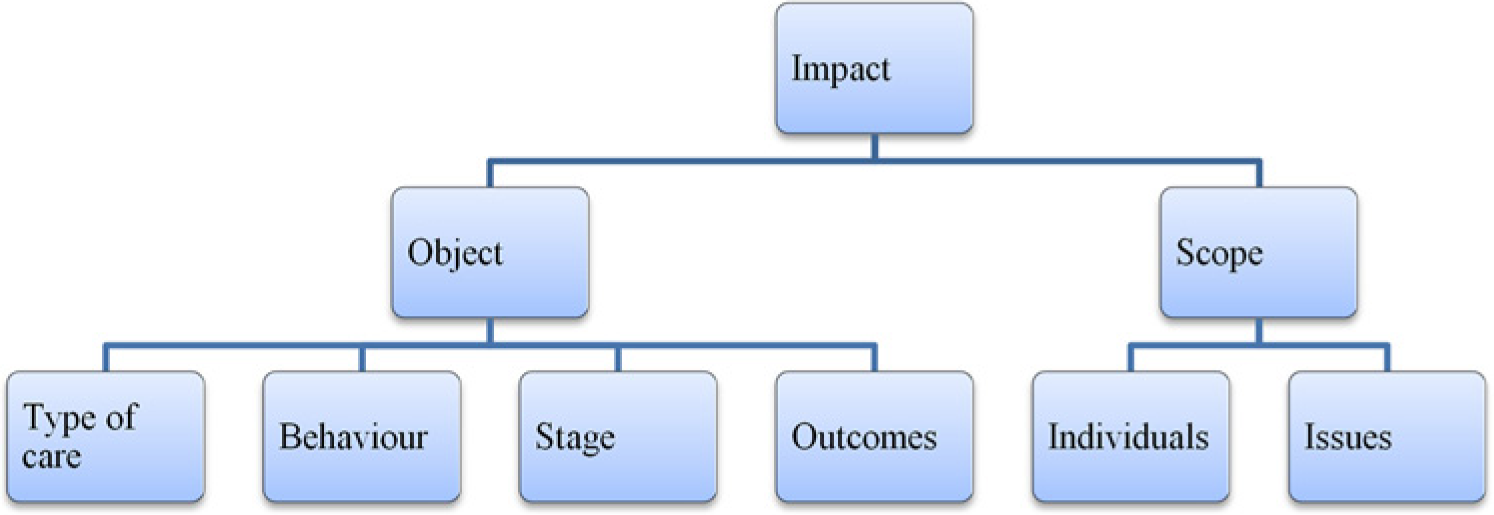
Dimensionalization of impact.
Individual-Related Dimensions
Awareness indicates the extent to which individuals are aware of the barriers preventing them from accomplishing a goal or an outcome (Figure 3). Actual and perceived statuses were the salient sub-dimensions associated with awareness. Actual status is determined by comparing perceived and actual barriers. Properties of actual status were awareness and unawareness of existing barriers. In this study, parents were more aware of constraints-related barriers such as transportation, family support, and lack of insurance and less aware or unaware of perception-related barriers such as perceived role of dentists and caregivers, perceived identity (signs and symptoms) of ECC, and perceived effectiveness of parental checking to detect cavities among others. Properties of perceived status were perceived awareness and perceived unawareness. Perceived awareness concerns the extent to which individuals think they are aware of the barriers, which does not necessarily mean that they really are. In the focus groups, a large number of parents affected by barriers of different nature were very confident indicating lack of insurance as the only barriers preventing them from regular dental attendance. Regarding the oral health status of children, many parents who were unaware of it were also confident in rating it as very good or excellent. Their perceived awareness was high, whereas their actual awareness was low. Parents showed their perceived unawareness when admitting that factors they were not aware of could also prevent them from either identifying ECC at earlier stages or impeding its development.
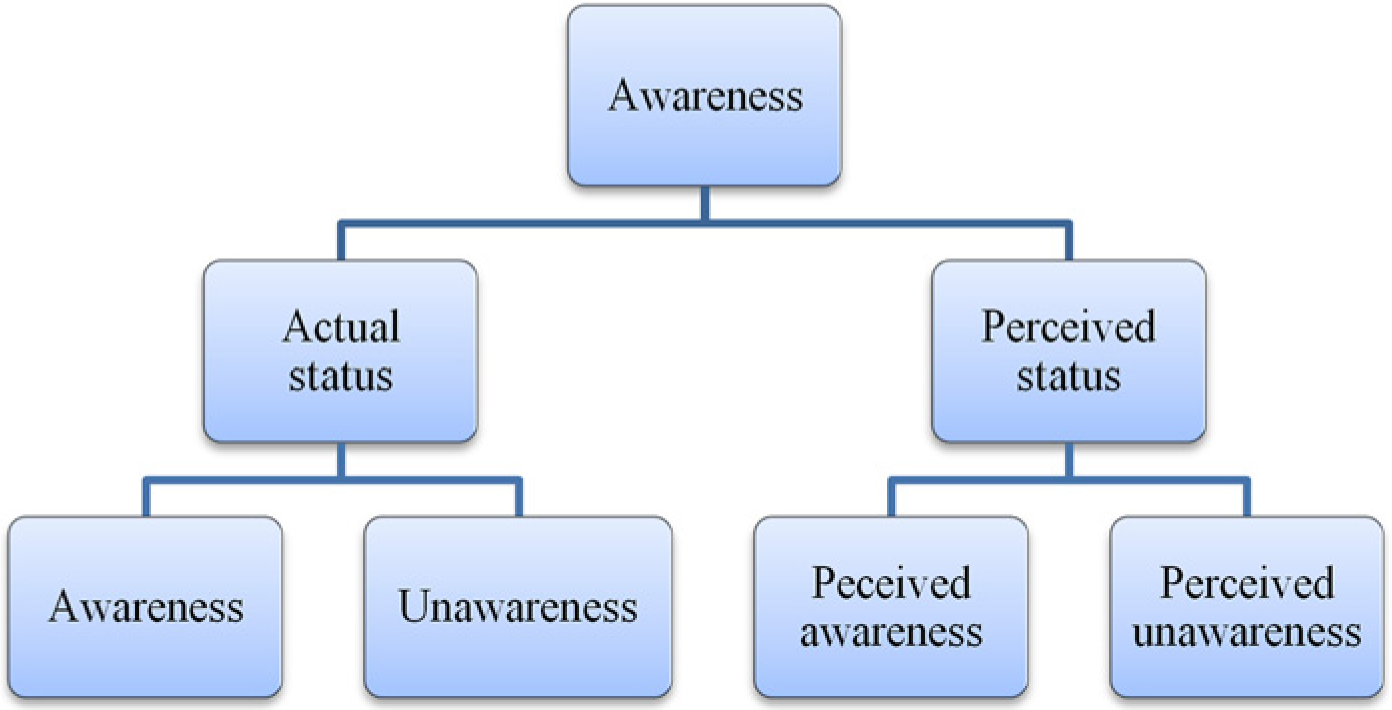
Dimensionalization of awareness.
Controllability encompasses the individuals’ control over the barriers (Figure 4). Object, locus, status, position, coping strategies, and amount were the salient sub-dimensions of controllability. Object refers to the barrier to be addressed as, for example, access to dental services or child’s resistance to brush his or her teeth. Locus was expanded into internal and external. Some barriers were seen as out of participants’ control (external) and others as part of their responsibilities, especially those related to at-home prevention like behavioral control of children when performing dentally risky behaviors. Status of controllability highlights the difference between perceived and actual controllability. As the present analysis was based on participants’ self-report, it was difficult to differentiate perceived from actual control. Parents who admitted having little control over their child’s sugar intake, for example, may be referring to actual control, perceived control, or both. Position was expanded into passive and proactive, reflecting the stand of participants when facing barriers. Some were more proactive and others more passive perceiving barriers as restrictions under which to act. Passiveness and proactiveness varied depending on the individual and the barrier in question. Coping strategies point out the actions undertaken to address barriers perceived under participants’ control. Getting dental treatment in the country of origin and emphasizing proper oral hygiene and sugar intake to prevent dental problems were among the strategies in place to address the cost of dental services. Amount was the sub-dimension referring to the extent of control over perceived barrier whose properties showed a continuum from little to relatively high control.

Dimensionalization of controllability.
Discussion
This study aimed to examine the underlying dimensions of the psychosocial barriers to prevention of ECC among children of recent immigrants in Canada. Dimensional analysis was used to identify salient dimensions, sub-dimensions, and corresponding properties. Found dimensions were related to barriers and individuals, which suggests that barriers are not only context-specific but also subject-related. What becomes a barrier for an individual, group, or community may not be a barrier for another. Type, number, level, relationship, nature, objectiveness, and impact were the dimensions associated with barriers, whereas awareness and controllability were associated with individuals.
Currently, an extensive body of empirical literature exists about oral health-related barriers. Those affecting utilization of dental services in general have received a great deal of attention (Bedos, Levine, & Brodeur, 2009). However, barriers associated with preventive dental visits in particular have been less documented and require further examination (Sohn, Ismail, Amaya, & Lepkowski, 2007). Findings of barrier studies are very consistent with respect to the type of barriers affecting specific social groups such as low-income individuals, minorities, and immigrants. The number of existing barriers with respect to same populations and unit of analysis (access to dental care, receipt of dental advice, satisfaction with services, etc.) vary from one study to another depending on its scope and methodological approach. Qualitative studies in general describe more barriers than quantitative studies, which usually focus on a limited number of variables and levels of influence. Unfortunately, much oral health research has examined a reduced number of individual-level factors (Fisher-Owens et al., 2007) and includes minimal contextual variables. Overall, it can be assumed that when the number of the identified barriers is lower than the number of existing barriers, the intended goal is less likely to be achieved. This explains why removing financial barriers does not ensure access to dental services (Ismail & Sohn, 2001), which is often influenced by other barriers including availability of these services, acceptability of public dental insurance, and prevention/treatment orientation of the patient (Sohn et al., 2007).
Psychosocial barriers affecting oral health have been found at individual, family, community, and systemic levels (Cruz, 2002), which is in line with the results of our study. This dimension of barrier seems to be critical when determining the scope of the intervention and the allocation of resources. As oral health is determined by multiple factors at different levels (Newton & Bower, 2005), multilevel interventions seem to be more appropriate. Inter- and intra-level relationships among barriers have been less documented in previous studies. However, these two dimensions, level and relationship of barrier, reflect the multilevel and reciprocal causation of the factors influencing oral health outcomes (Fisher-Owens et al., 2007). Our study also suggests that relationships between barriers should also be examined due to their potential cause–effect relationships. For example, previous research has indicated that barriers related to the quality of experiences at dental settings may lead to patients’ dissatisfaction with services and dental personnel (dentists and front-line staff), which in turn becomes a barrier for further dental visits (Lam, Riedy, & Milgrom, 1999).
The nature of the barriers has also been highlighted in previous studies, which have suggested that barriers related to perceptions–including dental beliefs–attitude, knowledge, values, skills, practices, and constraints significantly affect access to dental services and oral health outcomes (Hilton et al., 2007; Kelly, Binkley, Neace, & Gale, 2005). The nature of barriers may influence the odds of being recognized as such. In a study conducted with recent immigrant mothers from Northeast African communities, it was found that they were less likely to be aware of perceptions and values related to barriers than of contextual constraints such as lack of insurance, time, and family support (Amin & Perez, 2012). Limited success in addressing barriers may be also explained as the mismatch between the character of the barriers to be addressed and the character of the intervention. It is very unlikely that barriers involving skills, constraints, and a strong belief system can be eliminated or mitigated through mere information sharing. Thus, depending on the nature of the barrier in question, counseling can be more effective than lectures or instructions from a professional (Amin & Harrison, 2009). In addition, interventions may influence one or two determinants of a target behavior, which may not be its strongest predictors. Health education, for example, may influence behavioral beliefs and consequently attitudes (Mofidi et al., 2002), but it is less likely that influences self-efficacy deemed as the strongest predictor of general and oral health behaviors (Conner & Norman, 2005).
Previous studies have also indicated the impact of barriers affecting access to dental services, service delivery, clients’ satisfaction, receipt of dental advice, and early detection of caries (Amin & Perez, 2012; Edelstein, 2002; Lam et al., 1999). Consequences of access and service delivery barriers for individuals have also been identified. Missing school hours, persistent tooth pain, embarrassment, and low self-esteem were consequences of barriers for children, whereas stress, long waiting times, feeling of powerlessness, dissatisfaction, being blamed, and also low self-esteem were consequences for parents (Mofidi et al., 2002). Some barriers seem to have a specific and limited impact, while others may compromise several dental goals, behaviors, and ultimately outcomes. Therefore, determining the impact of barriers becomes necessary to set priorities when addressing them.
To our knowledge, the objectiveness of barriers, a dimension that differentiates actual from self-induced barriers, has not been previously documented. Participants showed both lack or limited knowledge and misperceptions regarding sources of insurance and covered dental services. Lack of knowledge and misperceptions are intrinsically different, which may have specific implications. Most participants who lacked knowledge showed interest in being more aware of available resources, while those holding misperceptions were sure that the resources were not available to them. Misperceptions may represent impediments unlikely to be addressed without external intervention or information coming from reliable sources. However, self-created barriers in the form of misperceptions may be easy to remove, which suggests that they can be addressed soon after being identified.
Individuals’ awareness of barriers is also an underreported dimension in the literature on oral health barriers. However, awareness of barriers seems to be a necessary condition for individuals to handle them. Difficulties in addressing barriers may result from lack of resources and inadequate ways of dealing with challenges (Hilton et al., 2007) but also from unawareness of the existing barriers.
Controllability, the other individual-related dimension, has also received little attention in the oral health literature. The examination of perceived and actual control over barriers to prevention of ECC has mainly focused on child’s resistance to regular toothbrushing and flossing and child’s food choices. Studies have shown differences between parents regarding perceived control over these barriers and a relationship between perceived control and oral health outcomes (Buglar, White, & Robinson, 2010; Finlayson, Siefert, Ismail, Delva, & Sohn, 2005). Overall, it has been found that caregivers experience and respond to barriers differently in ways that affect care-seeking behaviors (Kelly et al., 2005). Regardless of the adaptive intention behind the employed coping strategies, they may enhance or compromise oral health outcomes in the long term. For example, postponing or avoiding dental visits have been reported as a way of coping with dental fear, discrimination, and dissatisfaction with dental services (Mofidi et al., 2002). On the contrary, going to more distant places to obtain better dental care (Kelly et al., 2005) seems to be an effective strategy to address the perceived shortage of high-quality services in the area of residence. Despite differences in how barriers are experienced and addressed, it has been suggested that individuals also differ in their attitude toward impediments and challenges they encounter. A more proactive attitude in the face of challenges was found among the no-relapse group of parents whose children were treated for caries under general anesthesia compared with the relapse group (Amin & Harrison, 2009).
Identified dimensions can be used for descriptive, explanatory, and intervention purposes. When describing barriers, proposed dimensions become another set of variables. Thus, it can be described how many subjects are aware or unaware of particular barriers; what percentage of barriers concerns skills, perceptions, or contextual constraints; how much control individuals perceive or have over the barriers; and so on. Barriers, individually or in concert, can be better explained if their nature, impact, relationship, level of influence, controllability, awareness, and objectiveness are also understood. Identified dimensions may also inform intervention strategies intended to eliminate or reduce barriers in several ways. Dimensions such as type, level, and number help specify what should be addressed, namely, the focus of the intervention. Relationship, objectiveness, and impact of barriers can assist in setting priorities. Barriers compromising at-home and professional care, several preventive oral health behaviors, and many individuals should be addressed first as well as those that condition the presence of other barriers. Nature and awareness of the barriers seem to be key when developing intervention strategies. Being aware or unaware of existing barriers can be seen as two different stages of the barrier management process. Intervention must be adjusted to both the stage in which individuals are functioning (Conner & Norman, 2005) and the nature of the barrier.
Although this study focused on the recognition of salient dimensions of barriers and their corresponding properties, it also provided some indications about dimensions that have the potential to become general perspectives. A perspective is a dimension around which core dimensions can be organized as context, conditions, actions-interactions, and consequences. In our study, a promising dimension to become perspective is “controllability,” which can also be labeled as barrier management. From this perspective, awareness of barriers and perceived ability to address them could be considered as conditions that facilitate or block actions intended to address barriers. Actions themselves may be represented by the sub-dimension coping strategies. However, to develop this perspective, more theoretical sampling is required to further identify dimensions and properties related to actions, consequences, and context of barrier management. To our knowledge, no grounded theory has been proposed to explain how parents deal with barriers preventing them from providing and obtaining optimal oral care for their young children.
A distinction should be made between a perceived and a normative view of barriers. Individuals perceive barriers as impediments to what they want to accomplish. However, goal or behaviors that they are not intended to achieve or perform may become barriers from a normative view. Regarding dental visits, individuals may perceive barriers to dental attendance, but not to preventive dental visits. This is not necessarily because barriers do not exist, but because preventive dental visits are not intended in the first place. From a normative view, a major barrier to regular dental visit may be that this behavior is not associated with prevention. Thus, not only the lack of intention but also the definition of the goal may act as a barrier. In our study, oral health was mainly defined as absence of dental problems, and consequently, barriers were seen with respect to this general goal. The analysis of barriers should then encompass both the factors appose to the accomplishment of goals, and the goals individuals set to be accomplished.
The present study has two main limitations. As a secondary analysis of collected data on psychosocial barriers to prevention of ECC among immigrant parents, some dimensions, sub-dimensions, and properties may not have been fully expanded. However, additional focus groups were conducted to ensure that a critical mass of dimensions and corresponding properties had been obtained. However, no new salient dimensions and properties emerged after comparing our results with previous findings on oral health barriers. Proposed dimensions, sub-dimensions, and properties were not sufficiently discussed with experienced researchers in oral health-related barriers as recommended by the dimensional analysis methodology.
Conclusion
Barrier is an overused and undertheorized construct in the oral health literature. To our knowledge, dimensions underlying psychosocial barriers to prevention of ECC among immigrant parents have not been examined rigorously. These dimensions go beyond the type of barriers affecting the performance of behaviors and the accomplishment of goals and outcomes, which has been the main focus of most of the barrier studies. Dimensions also concern the number, level of influence, relationship, nature, objectiveness, impact, awareness, and controllability of barriers. These dimensions seem to be very useful to describe, understand, and manage existing barriers, regardless of the health domain in which the study is situated. Processes such as defining the barriers to be addressed, setting priorities regarding barrier management, and developing tailored interventions can be informed by the dimensions proposed in the present study.
Further research is needed to develop a comprehensive theory on psychosocial barriers and their impact on oral health-related behaviors, goals, and outcomes. Research methods must be also proposed and validated to measure its core categories. Oral health inequalities, especially among children, seem to result not only from existing barriers but also from a limited understanding of how they affect desirable outcomes. Without a deeper understanding of the opposing forces to optimal oral health, oral health disparities are likely to remain or even increase. Barriers studies must then adopt a new approach to better inform oral health policies through which impediments can be replaced by opportunities that benefit undeserved social groups from current prevention and treatment developments in oral health.
Footnotes
Acknowledgements
The authors wish to thank Dr. Ruth Wolfe for critically reviewing a draft of the manuscript as well as the Multicultural Health Brokers Co-Op for helping with recruitment of the participants and data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This study was funded by Prairie Metropolis Centre.