
Abstract
The Chronic Kidney Disease (CKD), taking the lives of thousands in poor farming communities in Sri Lanka, is commonly seen as a problem peculiar to the island’s north central dry zone agricultural region. The prevailing bio-medical focus is on identifying one or more “environmental nephrotoxins.” While delineating important controversies on the etiology of the disease, this article seeks to broaden the discourse on the hitherto neglected political economy of CKD in Sri Lanka. In so doing, it seeks to bring together the bio-medical debate on the impact of widespread and unregulated use of agrochemicals on public health and kidney disease with broader global interdisciplinary perspectives on the industrialization of agriculture and the consolidation of food production by transnational agribusiness corporations. The article concludes pointing out environmentally sustainable and socially equitable development and organic agriculture as the long-term solutions to CKD in Sri Lanka and elsewhere.
Introduction
The new form of Chronic Kidney Disease (CKD) pervading the dry zone of Sri Lanka constitutes a humanitarian tragedy with vast implications for the society, economy, and the environment. First detected in the early 1990s in the Anuradhapura and the Polonnaruwa Districts in the dry zone agricultural region in North Central Province (NCP), the disease is now spreading to neighboring districts in the North Western, Eastern, and Uva as well as the Central and Northern Provinces. The CKD prevalent area covers approximately 17,000 km with a predominantly rural population of 2.5 million (Figure 1; Chandrajith et al., 2010). CKD is the most prevalent among male farmers in the 40 to 60 age group engaged in rice cultivation, although lately, it has also been detected among women, children, and even cattle (Centre for Science and Environment [CSE], 2012).
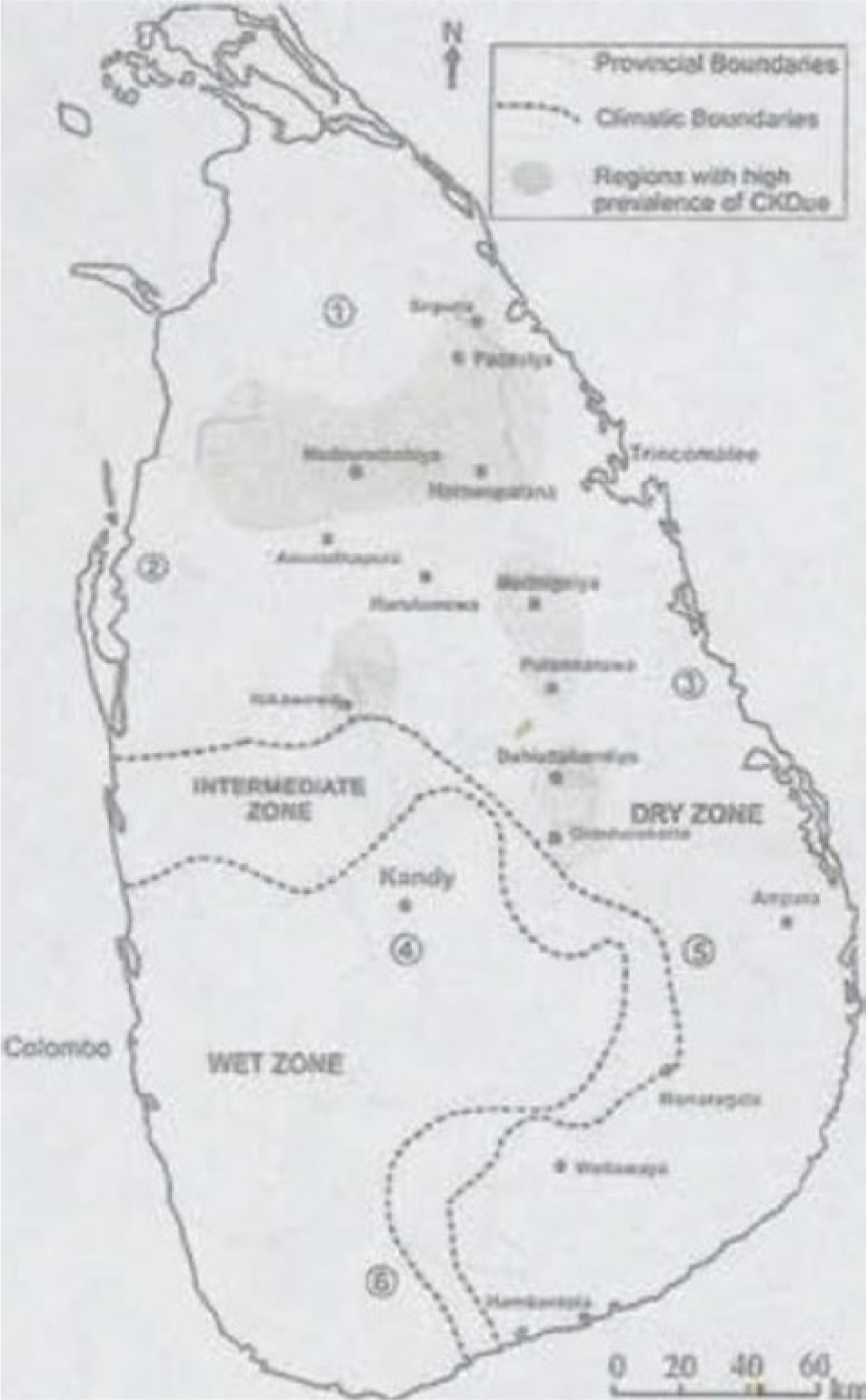
CKD prevalent areas in Sri Lanka.
There is scientific consensus that this fatal disease in Sri Lanka is not related to known causes commonly identified with kidney disease, such as, diabetes, hypertension, obesity, or other factors such as snake bite (World Health Organization [WHO] & Ministry of HealthCare and Nutrition, Epidemiology Unit, Sri Lanka, 2009). The exact cause of this disease is being determined. The WHO and the Sri Lankan government continue to designate it as “Chronic Kidney Disease of Unknown Etiology” (CKDu; WHO & Ministry of Healthcare and Nutrition, 2009). This rare form of tubule-interstitial disease involves slow, asymptomatic progressive kidney damage over 3 or more months, making diagnosis and treatment difficult. Nearly 80% of patients experience total kidney failure within 2 years following diagnosis. Given the inadequacy of medical services, the high cost of treatment—dialysis and organ transplantation—and the poverty of most victims, death becomes inevitable for most (Handunnetti & Daniel, 2012).
A group of Sri Lankan doctors estimates that as many as 400,000 people in Sri Lanka’s north central region may be affected by the disease (Perera, 2012a). Some 22,000 people have died from CKD over the past 2 decades in the NCP with at least 5 or 6 out of 100 people there currently affected (N. Gunawardena, 2012). In other words, more people in the NCP have died from CKD than from the armed conflict in Sri Lanka (Rathnasooriya, 2009). Some have speculated, without any evidence, that given the proximity of the NCP to the region claimed by Tamil secessionists, CKD could well be the result of bioterrorism—calculated use of micro-organisms to bring ill health or death to humans and the environment (Weerasekara, n.d.). In contrast to the bloody 30-year secessionist war (which ended in May 2009) and post-conflict politics, which continue to draw national and international attention, the structural violence of poverty and environmental destruction underlying CKD has received relatively little attention. The basic needs of poor farming communities for affordable medical attention, safe water, and food do not fall within the mainstream conflict resolution or human rights discourses (Meister, 2011)
Scientific researchers and government authorities are overwhelmingly concerned with identifying one or more “environmental nephrotoxins” to eradicate the disease (Nanayakkara et al., 2012; Senevirathna et al., 2011; Soderland, Lovekar, Weiner, Brooks, & Kaufman, 2010; Wanigasuriya, Peris-John, & Wickremasinghe, 2011; WHO & Ministry of Healthcare, Sri Lanka, 2009). This focus has delayed action on immediate health and social needs of patients and their families. It has also contributed to a relative neglect of the broader political-economic and social-psychological dimensions of the problem; an exception is the work of Chandani Liyanage and Ramanie Jayathilaka (Liyanage & Jayathilaka, 2009). In Sri Lanka, CKD is commonly seen from a limited perspective as an isolated issue particular to the island’s dry zone agricultural region. Its local designation is “Rajarata Kidney Disease,” Rajarata (country of the kings) being the ancient Sinhala name for the dry zone agricultural civilization (Rathnasooriya, 2009). CKD is not commonly found in other rural areas of the country that have rice cultivation practices and lifestyles similar to the north central dry zone. Some researchers consider the “unique hydrochemistry of the drinking water” in the Rajarata to be the reason for the prevalence of CKD (Chandrajith et al., 2011). Other researchers consider the “hardness of the ground water” and the “heavy metal retention capacity” of the soil in the region to be the causative factors (de Silva et al., 2013).
This article is based largely on a review of the literature on CKD in Sri Lanka. While incorporating the findings of bio-medical research, it seeks to provide a broader interdisciplinary and global approach to CKD. It draws on the theoretical perspectives of political economy, international development, ecology, and environmental justice as well as comparative information of spreading CKD in agricultural regions in Nicaragua and India. The Sri Lankan case is placed within the context of globalization and unsustainable economic development, specifically industrialization of agriculture and the widespread use of controversial agrochemicals. The article concludes emphasizing organic agriculture and access to safe water and food as the long-term solutions to CKD in Sri Lanka and related problems of public health and environmental sustainability worldwide.
The literature review and theoretical approach of this study are informed by many years of fieldwork. The study has its origin in the late 1990s in the author’s work in Sri Lanka as a consultant to the Sarvodaya Women’s Movement (Sarvodaya is considered to be the largest village-based NGO in the world) and its organic cultivation and income generation program for women. The author’s field research and Report for Care International on Integrated Pest Management in Sri Lanka in 1998 has greatly helped this work (Bandarage, 1998). The author first came into contact with kidney patients, kidney donors, and doctors in the Kidney Unit of the Kandy hospital in Sri Lanka in 2005. Since then, she has been investigating CKD through discussions with kidney patients, donors, scientists, physicians, and environmental and health rights activists in Sri Lanka (Bandarage, 2005). The research has benefitted greatly from communication with colleagues in activist organizations, such as, the Center for Environmental Justice, an affiliate of Friends of Earth International in Sri Lanka and the Kandy Kidney Protection Society, an NGO that was organized largely by volunteer doctors.
Spreading CKD
CKD is rising at an alarming rate in Sri Lanka, but the exact extent is difficult to determine given that many people may not be receiving hospital treatment. There is an estimated 2% to 3% prevalence rate in all affected provinces with a 15% prevalence rate in the 15 to 70 age group in the NCP and Uva Province (Mendis, 2011). Between 1990 and 2007, hospital admissions due to all diseases of the genitourinary system in Sri Lanka doubled with hospital deaths due to such diseases rising from 2.6 to 9.1 per 100,000 people. As the August 2012 Report from the CSE in New Delhi, India noted, “CKD has been the predominant contributor to this rise in hospital morbidity and mortality” (CSE, 2012)., According to the estimates of some Sri Lankan physicians, 300 to 600 CKD related deaths occur in hospitals annually. However, the total number of deaths due to CKD could be as much as 1,400 annually nationwide because home deaths are not included in death registries (Athuralia, Abeysekara, Amerasinghe, Kumarasiri, & Dissanayake, 2009; A. Gunawardena, n.d.).
Sri Lanka has a relatively comprehensive and free public state health care system but finds it difficult to keep pace with the alarming rate of growth of CKD. Current dialysis units can serve only a small proportion of patients and existing facilities are considered to be grossly inadequate. About 5% of the Annual Health Budget is spent on the management of CKD patients (N. Gunawardena, 2012; Irin Asia, 2008; WHO & Ministry of Healthcare and Nutrition, 2009). Many more dialysis machines and other equipment and services are needed to meet the growing demand (N. Gunawardena, 2012). The Kandy Kidney Protection Society points out that “awareness programs regarding prevention, screening programs for early diagnosis, provision of financial and other support for needy patients, improvement of infrastructure and promotion of kidney donations for transplant have to be carried out in a well organized manner” (Kandy Kidney Protection Society, n.d.)
In 2005, a kidney patient had to spend approximately Rs. 10,000 (approximately USD 79) for dialysis and Rs. 800,000 (approximately USD 6,320) for a kidney transplant (Gunatilleke, 2012). Lacking funds, patients pour into the kidney units of the few public hospitals that provide free kidney dialysis and transplants. The vast majority of the patients who come there are so poor that many of them have to forego some of the procedures and medications that require payment. The dialysis patients have to come several times a week traveling great distances. Being too weak to travel alone, they come with family members. Frequently after dialysis, some of the patients and their families sleep together on the hospital floors because there are not enough beds. When a breadwinner develops kidney disease and can no longer work, the entire family goes into financial ruin and debt. In some cases, children have had to forego schooling to find employment and women have had to engage in prostitution for economic survival (Bandarage, 2005).
Many patients wait years in pain and agony and many die due to chronic shortage of kidneys (Bandarage, 2013b). Due to the “frantic and sometimes futile search by desperate victims . . . to find a donor with a matching kidney,” doctors in the Kandy Teaching Hospital have initiated new efforts, such as “double transplants” with four patients, two kidney donors and two recipients side by side (Hettiarachchi, 2011). According to the WHO, organ trafficking accounts for 5% to 10% of all kidney transplants in the world (Budiani-Saberi & Delmonico, 2008). Kidney sales and all organ sales are illegal in Sri Lanka. Until September 2010, kidney donations were accepted only from relatives and members of the clergy. The desperate need for kidneys led to the change in government policy allowing kidney donations by non-relatives (Tops.lk, 2010).
Buddhist monks, many of them young men and from rural agricultural communities themselves, continue to be the predominant kidney donors. Like the patients, these monks have hardly any money or material possessions; but their compassion and generosity are enormous. As one mother whose son was to receive a kidney said of his donor monk, “he is not doing it for money. I can only bless him as I have nothing to give.” The donor monk responded, “I thought about the impermanence of life and how our bodies will anyway be absorbed to the soil one day. If one can make a sacrifice when we are alive, one can gain some spiritual happiness” (Chavkin, 2012b). Such selflessness is the most admirable, but long-term solutions to CKD require attention to scientific controversies and the political economy of the disease.
Identifying the Cause
Despite its emergence more than 20 years ago, the mystery surrounding the Rajarata Kidney Disease has not yet been resolved. People fear attending medical clinics due to the stigma attached to being classified as a “kidney patient” carrying the dreaded CKD. This has contributed in part to delays in understanding the origins and spread of CKD (Kulatungaarachchi, 2011). The scientific community continues to be perplexed as to why CKD is peculiar to the north central region and not the other rural areas of the country that have similar rice cultivation practices and lifestyles including extensive use of agrochemicals and aluminum utensils for cooking and storing water (Chandrajith et al., 2011). A study published in 2011 comparing three rural populations in Medawachchciya in the NCP, Yatinuwara in the Central Province (CP), and Hambantota in the Southern Province (SP) concluded that while CKD of an “unknown etiology” was prevalent in the NCP, known risk factors, notably diabetes and long-standing hypertension were the main factors for CKD in the other two provinces in Sri Lanka (Athuralia et al., 2011). As the national controversy over the cause of the Rajarata kidney disease expands, the disease’s etiology continues to be classified as “unidentified” (Mendis, 2012b).
A study by a team of Sri Lankan scientists published in April 2009 attributed CKD to heavy metals from various forms of fertilizers and agrochemicals entering the human body through the food chain (Chandrajith et al., 2010). Several other studies of the north central region revealed CKD prevalence in areas where drinking water was drawn from the ground from wells or pipelines and non-prevalence of CKD in areas where drinking water was obtained from natural springs (CSE, 2012; Liyanage & Jayathilaka, 2009). Another study published in January 2010 by a team of Sri Lankan and Japanese scientists hypothesized that “the unique hydrogeochemistry of the drinking water,” specifically high levels of fluoride, to be the decisive factor in the emergence of the disease in the north central region (Chandrajith et al., 2011). Aluminum utensils used for cooking and storing water, which enhance fluoride intake into the body, and Cynotoxin that comes from blue green algae have also been hypothesized as possible causes (CSE, 2012; Desalegn et al., 2011; LankaJournal, 2011).
The high temperatures in the dry zone and the need to consume higher volumes of water to regulate water balance by farmers working long hours have also been postulated as factors in CKD (Chandrajith et al., 2010). Global warming, climate change, and increasing droughts and water shortages in Sri Lanka’s dry zone may not bode well for the eradication of CKD. As a researcher from Sri Lanka’s University of Peradeniya who co-authored a 2011 Report on CKD put it, “if the temperatures are going up, the situation is likely to worsen” (Perera, 2012b). The Government Ministry of the Environment has reported 1,400 droughts island wide between 1985 and 2004, mostly in the dry zone with the most severe ones in 2001, 2004, and 2012 (Perera, 2012b). According to the Climate Change Unit of the Ministry, temperatures in the island have risen by about 0.45° Celsius in the past two decades (Perera, 2012c). In some of the CKD prevalent areas, such as, the Polonnaruwa District, temperatures have reached record levels of 34° to 35° Celsius (Perera, 2012b).
Research findings released in January 2011 by scientists in the Medicine and Allied Science Faculty of the Rajarata University in the NCP concluded that the “contamination of water resources by extensive and continuous use of agro-chemicals” that contain high percentages of arsenic and mercury are the causes of CKD in the NCP (LankaJournal, 2011). They also found the “total hardness of drinking water of CKDue patients [in the region] to be very high” (CSE, 2012). The calcium content in the hard water in the NCP when combined with the arsenic in fertilizers and pesticides reportedly forms calcium arsenic crystals. When transported to the kidneys, the calcium arsenate crystal “disturbs the antioxidant defense system in the renal tissues” (CSE, 2012). Postmortem tests have found deposits of arsenic in diseased kidneys of CKD patients. Even a very tiny amount of arsenic is believed to be toxic to the environment and human health (Jayasumana, 2012). A study conducted by a research team from the Kelaniya University in Sri Lanka also found a “strong positive correlation between the arsenic content and ground water hardness in CKDue prevalent areas” (CSE, 2012). Dr. Priyani Paranagama of the Kelaniya Team reported finding hyper-pigmentation and keratosis in the soles and palms of CKD patients signifying chronic arsenic poisoning (de Silva et al., 2013; Handunnetti & Daniel, 2012).
The above multi-factorial findings implicating agrochemicals and water quality soon became controversial given wide media coverage of opposing perspectives. At a press conference “Croplife Sri Lanka,” an industry group representing 26 agrochemical companies criticized “dubious research” of the Rajarata and Kelaniya University researchers asserting that there was no arsenic in the pesticides used in Sri Lanka (AgroNews, 2011; ColomboPage, 2011). The research was also subjected to media ridicule because one researcher claimed that he derived the insights into the cause of CKD through divine intervention (BBCSinhala.com, 2011; Wansapura, 2011). A study by a team of Sri Lankan and Japanese scientists published in June 2011 yet again concluded that CKD was the “outcome of exposure to an unknown nephrotoxin” (Nanayakkara et al., 2012). In light of conflicting analyses and divergences, the Sri Lankan Government Health Ministry announced that it would declare the “real cause” of CKD by June 2012 after the release of a specialist report “from a medical institution in Belgium” (Gunatilleke, 2012).
The “real cause” has not yet been declared. The controversy has only intensified taking attention away from the broader political and economic and global context of the disease and the urgent health and survival needs of victims and families. Recently, the debate has been focused on two reports recently released to the media, one associated with WHO and the other by a leading New Delhi–based NGO, CSE. The WHO study was commissioned by Sri Lanka’s Health Ministry’s epidemiological unit in 2008/2009 as an extensive 10-part study to test “people and the environment—blood, urine, tissue samples and the region’s food, water and air” (Countercurrents.org, 2012). The CSE Study was done in collaboration with the Sri Lankan Government’s Ministry of Water Supply and Drainage and the NGO, the Center for Environmental Justice in Colombo (N. Gunawardena, 2012). It tested drinking water as well as soil and food in the affected and unaffected regions to determine the cause of CKDue (CSE, 2012).
While the WHO findings still remained classified, a group of Sri Lankan doctors associated with the WHO study commissioned by Sri Lanka’s Health Ministry’s epidemiological unit in 2008/2009 released a report on August 14, 2012. According to that report, heavy metals in water caused by “unregulated use of fertiliser and pesticides” is the main cause of CKD (Perera, 2012a). Other progress reports from the WHO Study also implicate heavy metal toxicity, particularly Arsenic and Cadmium in either water or food as reflected in raised levels of these found in urine samples of patients (Perera, 2012a; Mendis, 2012a, 2012b). WHO progress reports claim that “drinking water is unlikely to be the source of the Arsenic and Cadmium exposure that is causing CKDu” (Mendis, 2011). WHO recommends “urgent action to improve safe use and quality control of agrochemicals and quality control of fertilizer” (Mendis, 2011). However, the CSE Report released just 1 day later, on August 15, 2012, ruled out Arsenic and heavy metals in food and water attributing CKD instead to poor water quality in the affected region. Arguing that “the quality of drinking water is at the base of all theories linked with CKDu,” it called for improvement of the quality of drinking water in the affected region (CSE, 2012).
Divergent opinions highlight scientific gaps and the need for better data collection and dissemination. Even more importantly, it highlights the need for a multi-factorial and integrated approach that goes beyond the fragmented search for a single “real cause” of CKD. Instead of waiting to identify one bio-medical cause, the seemingly mysterious and isolated Rajarata disease needs to be seen in the broader context of unsustainable economic growth and the degradation of the environment and public health. The controversy over CKD in Sri Lanka also highlights a host of political issues pertaining to transparency and accountability of government authorities, international organizations, and agrochemical corporations.
Local and international activists have accused the Sri Lankan government for maintaining complete silence about the findings of the 10-part WHO study commissioned by the Health Ministry for 3 years despite “growing public pressure and repeated promises of definitive answers” (Chavkin, 2012a). Dr. Channa Jayasumana, a member of the team of doctors that released the earlier mentioned report to the media in August 2012 has accused the authorities for failure to make the WHO Report public and to take action based on its results (Perera, 2012a). Local journalists and activists were also asking why the findings of the WHO Report had not yet been released (N. Gunawardena, 2012). As one journalist wrote: “We cannot afford bureaucratic apathy in a matter of such urgency and importance. The outcome of public science must be shared with the public and media in the public interest” (N. Gunawardena, 2012). In the CKD affected Rajarata, there is growing frustration with seemingly endless testing of people and their environment, bureaucratic apathy, and the contradictory explanations given by outside experts. No real progress is evident in eradicating the disease or in improvement in people’s lives. There is a sense that because they are poor, they are being treated as “lab rats” (N. Gunawardena, 2012). The local people who have lived in the villages since birth have their own explanations of the etiology, origin, and spread of the disease (Liyanage, 2011). They have an experiential understanding that the “real cause” of CKD does not lie in one isolated cause but the entire trajectory of unsustainable social and economic development set in motion in recent decades. A local Buddhist monk from the NCP gives voice to the general consensus in the local villages when he says, in the good old days none of these problems were evident. Those days no chemicals were used to gain harvests. They indulged in pure cultivation methods. Today the water content that is used is not subjected to checks. This results in people coming into contact with poisonous and harmful substances. (Kulatungaarachchi, 2011, p. 13).
In certain CKD affected regions in the NCP in Sri Lanka, the environment is extensively affected: Species of fish are disappearing and cattle are affected with interstitial nephritis (CSE, 2012). Pesticides are also contributing to the decline of amphibians, such as, the common hourglass tree frog (Jayawardena, et al., 2010). A bio-medical approach alone is not sufficient for understanding the depth of environmental and social destruction or long-term solutions. CKD has to be demystified from a broader ecological and political-economic perspective. The industrialization of agriculture and the model of social and economic growth it represents need exploration.
Industrialization of Agriculture
Rajarata, home to the CKD tragedy, was the seat of the ancient hydraulic civilization and is still the “rice bowl” of the island producing much of its staple food. A vast interconnected irrigation system of reservoirs and canals formed the basis of the prosperous economy and the Rajarata culture (Bandarage, 1983). Even after the demise of the dry zone civilization in 12
Traditional agriculture in Sri Lanka, as in other parts of the world, was characterized by ecologically sound practices such as inter-cropping, crop rotation, use of compost and animal manure, and natural pesticides. Swidden (chena) cultivation, which complemented rice cultivation, was characterized by diversified cultivation of millet, legumes, beans, and so on and the abandonment of land after each season until re-cultivation years later. Such practices helped maintain ecological harmony including balance between crops and pests. Unnatural increase in pests or contamination of water and soil were not common problems (Thirugnanasuntharan, 1989). Labor-intensive traditional agriculture was also characterized by well established collective labor sharing arrangements with neighbors helping each other plant, safeguard, and harvest crops (Bandarage, 1983).
With European colonialism, a new form of export oriented plantation agriculture was introduced in the wet zone of the island. In the pre–World War II period, even this sector relied on traditional methods, such as “cut and burn or bury” for purposes of pest control (Thirugnanasuntharan, 1989). The plantation sector became dominant taking land, labor, and state support away from subsistence agriculture. The dry zone rice cultivating areas were neglected and the rice or paddy farmers were marginalized. As rice cultivation suffered and as the population increased, the country became more and more dependent on imported rice and the vagaries of the global market (Bandarage, 1983).
After 1948 in the post-independence period, the Sri Lankan Government introduced massive projects to resuscitate rice agriculture through irrigation schemes and settlement of families from the populous wet zone areas to the sparsely populated dry zone. Many of the people stricken with CKD in the dry zone today are likely the descendants of those who settled in projects aimed at improving farmer self-sufficiency and prosperity. While a few farmers have prospered, the long-term result has been political patronage, class differentiation, and impoverishment of peasant rice producers. The resettlement projects that could not reproduce traditional labor sharing arrangements and community-based lifestyle, introduced a more competitive and individualist approach to agriculture and social relations (Bandarage, 1988; Udyanganie, Prasada, Kodithuwakku, Weerahewa, & Little, 2006).
Given hypotheses implicating the hydrogeochemistry and waterborne chemicals as causative factors for CKD in Sri Lanka, the impact of the Mahaweli River Development and Resettlement Program on the dry zone needs investigation. The controversial World Bank and other donor-funded programs involving the diversion of the Mahaweli, the longest river in Sri Lanka, cover nearly 39% of the entire island. This massive program was initially meant to be completed in 30 years but accelerated in 1977 to be completed in 6 years. Researchers have stated that at least a third of the money for the program was lost though graft. Faulty and hasty construction of dams, reservoirs, and so on are believed to threaten the ecological balance of the hill country where the Mahaweli originates and the dry zone through which the massive river flows into the ocean (Bandarage, 1988). As a joint research study published in 2010 by Sri Lankan and Japanese scientists pointed out, change in the hydrogeochemistry and salinity in the CKD affected areas “could well be caused by the large irrigation scheme that commenced two decades ago” (Chandrajith et al., 2011).
The “Green Revolution” using “miracle” hybrid varieties of seeds and dependent on extensive use of agrochemicals including fertilizers, hormones, soil treatments, and pesticides was introduced to Sri Lanka in the 1970s. Agrochemicals that enhance crops began to be used extensively in Sri Lanka’s plantation and traditional agricultural sectors with the introduction of the “Open Economy” and import liberalization in 1977. Between 1983 and 1997, the quantities of formulated pesticides (insecticides, herbicides, and fungicides) imported increased tenfold (Sim, 1989; Taylor, 1999). While imports leveled off in subsequent years, increasing commoditization and industrialization of agriculture kept pesticide use at high levels. Pesticide use has been particularly heavy in the Mahaweli Development Program and the NCP (Udyanganie et al., 2006). Graeme Taylor who conducted a field study of pesticide use in the Mahaweli H area in 1999 noted that 89% of paddy cultivated areas there were chemically weeded. He described aspects of the industrialization of agriculture: . . . Usually the field is first treated with paraquat, and then treated with two different herbicides. New strains of rice have been produced that are more responsive than traditional varieties to inputs of fertilizers, leading to improved yields. However, increased fertilizer inputs will also result in increased weed growth, so herbicides are commonly applied throughout the crop cycle. (Taylor, 1999).
A study published in 2009 by Rohana Chandrajith and a team of Sri Lankan scientists reported that paddy soils in areas experiencing rapid economic development are polluted with potentially toxic metals. The study observed widespread application of phosphate fertilizers with uranium and other elements known for their nephrotoxic effects: The paddy soils in Sri Lanka are . . . highly modified by artificial fertilizer applications. During the period of waterlogging in rice cultivation, the chemical nature of the soil can be drastically changed and pollutants can be leached easily into subsurface, which eventually contaminate the ground water that rural people use as a drinking water source. (Chandrajith et al., 2010)
In Sri Lanka, where rice is cultivated in two or some cases three seasons per year, fertilizers tend to be applied 3 times every season. Chandrajith et al explain that the recommended amount of application is 270kg per hectare of fertilizers such as urea, triple phosphate (TSP), and potash per season. However, over the past few decades, their application has increased by more than a factor of two exceeding the recommended levels. They attributes this massive increase to fertilizer subsidies granted by the government and the use of “very low quality” imported fertilizer due to “the unavailability of a proper controlling mechanism” (Chandrajith et al., 2010). The search for causes of the CKD epidemic necessitates consideration of the bio-medical as well as the ecological and political-economic dimensions of agrochemical use.
Agrochemicals
Chemical pesticides have their origin in modern warfare: Nazi Germany experimented with them as weapons to be used against human enemies. Malathion and Parathion were originally developed as neurotoxins during World War II. It was only later that they came to be applied against pests in agriculture (Sasi, 1996). Pesticide pollution is one of the most serious global environmental and health problems today. Consumer agitation has led to banning and restricting of some of the most dangerous pesticides and improving safety standards in the global North. However, many dangerous pesticides banned in the North are still being “dumped” in some countries in the South where regulation and safety standards are far more lax (CorpWatch, 2002; Pellow, 2007). Ultimately, however, the cycle of poison created by chemical agriculture envelops all life on earth. The countries in the North do not escape the poison: It comes back via pesticide-laden food imported from the South and through the ecosystem.
Hybrid seed varieties promoted by the Green Revolution require large amounts of water from irrigation systems and dams, which in turn aggravate pest problems. Populations of harmful pests increase as they become resistant to chemical inputs. As newer, stronger, and more serious insect diseases and weed problems develop, even smallholders cultivating tiny plots of land are caught in a “pesticide treadmill” that they find difficult to escape (Bull, 1982). Excessive use of chemical pesticides in Sri Lanka have introduced insects, such as the brown planthopper, infecting rice crops as well as weeds and diseases that were never problems previously. As pesticide problems worsen, poor farmers have to buy expensive and stronger varieties of pesticides before they could earn any money from the harvest. Chemical pesticides kill harmful pests, but they also kill beneficial life-forms disturbing the delicate balance of ecosystems depleting soil of nutrients and rendering lands unsuitable for cultivation. The short-term approach leads to quick returns—high yields and profits—but poses fundamental threats to environmental sustainability, global food security, and human health (Bull, 1982; Centre for Science and Technology of the Non-Aligned and Other Developing Countries, 2005).
A Food and Agriculture Organization (FAO) study in 2005 reported more than 1,000 brand pesticide products registered marketed and/or handled by private sector organizations in Sri Lanka (Sumith, 2005). Due to “commercial pressure and competition” between the agrochemical companies, credit facilities for purchase of pesticides are widely available to Sri Lankan farmers (Taylor, 1999). Since the 1980s, synthetic pesticides have been “freely available over the counter with no controls or restrictions on sales” and in rural areas often sold “through general stores alongside food stuffs and household goods.” (Taylor, 1999).The sales-driven promotional strategies of agrochemical firms seem to pay little attention to farmer education of the toxicity and proper use of pesticides. Studies have shown that some vegetable farmers in Sri Lanka apply pesticides to their crops before appearance of any pests as a measure of precaution (Bull, 1982; Chandrasekara, Wettasinghe, & Amarasiri, 1989). It is also common among farmers to spray vegetable crops just before harvesting and marketing. Most of the fruits and vegetables grown in Sri Lanka may thus be laden with chemicals posing threats to producers and consumers locally and internationally (Sumith, 2005). Sociologists Ramanie Jayathilaka and Chandani Liyanage who conducted field based research in the Anuradhapura District report that the villagers they interviewed believe that “all the food items including tank fish available in their locality are not suitable for consumption” because of chemical contamination and CKD risk (Liyanage & Jayathilaka, 2009).
Even when Sri Lankan farmers are aware of the extreme dangers of some of the agrochemicals, they lack the proper equipment and protective gear for safe use or the facilities for safe storage. As a result, occupational and accidental pesticide poisoning is rampant. In the late 1970s, Sri Lanka had the highest rate of pesticide poisoning in the world (Bull, 1982; Chandrajith et al., 2010; Taylor, 1999). According to FAO figures in 1997, Sri Lanka still ranked “very high in the Asia Pacific Region with regard to pesticide related health hazards” with an annual total number of pesticide accidents around 20,000 (Sumith, 2005). As David Bull noted in his Oxfam sponsored study of pesticides and the Third World poor, Most of the victims of pesticide poisoning in Sri Lanka are rice and vegetable farmers. These are not rich farmers. Over 90% of . . . paddy (rice) holdings are of 10 acres or less. It is among the mass of the rural poor in this poor country that pesticides take their toll. (Bull, 1982)
Minor pesticide poisoning contributes to nose bleeds, depression, dizziness, and headaches, as well as long-term health problems such as cancer and Parkinson’s disease and may be traceable to inhalation of the widely used herbicide Paraquat (also known as Gramoxene) and other chemicals (Taylor, 1999). The toxic effects are not limited to male farmers. Entire communities are affected. Long-term reproductive health problems associated with pesticides including sterility, miscarriages, and birth defects are particularly high in the Mahaweli areas (Care International, Sri Lanka, 1997; International Water Management Institute, 2002). Purchase of expensive pesticides has also put many farmers in debt forcing some to sell their lands and become landless laborers. As in India, suicide by pesticide poisoning is not uncommon among indebted farmers in the agricultural regions in Sri Lanka (Frontline, 2005).
Despite growing awareness of the risks of chemicals and pesticides and possible link to the epidemic kidney disease, farmers in the CKD affected regions are extremely reluctant to give up the use of agrochemicals. They now have little confidence in themselves and in the organic, traditional agricultural methods of their ancestors. They have been made to believe that the new chemical-industrial approach represents progress and that chemical pesticides are indispensable for their survival. As one farmer in the NCP put it, It is difficult for us to earn our day to day living without using chemicals for our cultivations. This is the stark truth. If we do not use them our harvest will not be as bountiful as it is right now. But then again we know the health hazards posed to us by constant use of such products. This is the never-ending struggle that we are facing and we have no alternative. (Kulatungaarachchi, 2011)
Recognizing the deep psychological conditioning of farmers and difficulties they have giving up “addiction” to agrochemicals, village leaders are calling for strong governmental action. As a Buddhist monk in the region, says, There is no use in debating on the merits and demerits of such products [agrochemicals] because no matter what we say these people are beholden to these products . . . Officials must strictly ban the use of products which imperils the lives of people. It is only through such a measure that the government will be able to save the lives of countless others who would otherwise succumb to this dread in the years to come. (Kulatungaarachchi, 2011)
This, however, is not an easy task. The import of agrochemicals is financed by the Sri Lankan government. Establishment of a definitive link between agrochemicals and CKD may have significant implications for the corporate–state relationship (Chavkin, 2012a).
Battle Over Pesticides
Ten companies in the Global North now control 90% of the 44 billion dollar global pesticide market. Those consist of the “Big Six”—Syngenta, Bayer, Monsanto, Dow, BASF, and Du Pont—(ETC Group, 2011). Corporate control is not restricted to pesticides; it extends to other agricultural inputs, notably seeds and biotechnology. Fifty of the global seed markets are dominated by 10 corporations many of whom are also the top pesticide corporations (Pesticide Action Network, 2013b). According to Robert Fraley, co-president, Monsanto’s Agricultural Sector (now Monsanto’s executive vice president and chief technology officer), “what you are seeing is . . . a consolidation of the entire food chain” (McCauley, 2013; Pesticide Action Network, 2013a). The Pesticide Action Network points out that this consolidation is achieved through the “revolving door” between government and corporate sector employment and lobbying in Washington, D.C., and other capitals around the world: Many of the agrochemical industry’s former executives, lawyers and scientists serve in the government agencies that are charged with keeping watch over their industries . . . The agricultural input industry maintains an army of lobbyists in Washington D.C., state capitals and countries worldwide to protect their interests . . . agribusiness spends over $100 million a year lobbying Congress. (Pesticide Action Network, 2013c)
Pesticide use is supported by governments and donor agencies, which often require funds granted to the South to be used to buy a pesticide of a specific origin. Pesticide use has been growing at higher rates in the poor countries than in the North in recent decades. In addition, no strict guidelines exist in the United States to prevent a company from exporting banned pesticides (Environmental Protection Agency, 1992). The World Bank, which promotes export agriculture in the Third World, has also earmarked large sums of money specifically for pesticide purchases (Bandarage, 1997). While practically all chemical pesticides were manufactured abroad in the past, now, local formulation is increasingly undertaken in the South by subsidiaries of Northern corporations (Bull, 1982).
In Sri Lanka, a handful of local firms—Hayleys, Harrisons Chemical, Lankem, and CIC Crop Guard—and their subsidiaries sell base chemicals and patented products of transnational corporations, such as Syngenta, Monsanto, DuPont, Bayer, Ciba-Geigy, Shell Company, and F.M.C. Corporation (de Alwis, 1989). Like the transnational corporations, some of the leading local pesticide companies also control other sectors of local food production—seed production, biotechnology, and food processing and packaging (Hayleys, n.d.) The Capital Maharaja Organization, which acquired Harrisons Chemical in 1989 and is considered to be the “single largest group of private sector companies in Sri Lanka,” also leads in the fields of communication, media, and information technology in Sri Lanka (Capital Maharaja, n.d.).
The spread of pesticides throughout Sri Lanka is the result of extremely effective marketing and distribution strategies involving hundreds, if not thousands, of regional dealers and sub-dealers. Agrochemical firms have large advertising budgets, and they use attractive posters, radio, and television advertisements and films to extol the benefits of agrochemicals as the modern and practical way to high yields and farmer prosperity (de Alwis, 1989). Long-term relationships between the agrochemical firms and agricultural officials (from the government’s Department of Agriculture) working at the field level help give legitimacy to pesticide use. Cultivation of close relationships with farm leaders and local pesticide dealers through economic incentives has also proved to be a successful strategy for agrochemical firms (de Alwis, 1989; Staring, 1989). The firms use well-educated, professional marketing personnel and provide high achievers in their dealer networks with lavish rewards and incentives. CKD activists believe that media objectivity on the CKD may also be compromised due to the heavy dependence of the mainstream media on lucrative advertising in newspapers, radio, and television by the agrochemical companies. 1
Sri Lanka’s powerful agrochemical industry disputes the notion that its products are to be blamed for CKD. The Secretary of Sri Lanka’s National Agribusiness Council claims that pesticides produced by many multinational and international companies follow all the WHO and FAO guidelines and “those are not in harmful levels” (Chavkin, 2012a). After tests revealed contamination with small amounts of arsenic, Sri Lanka’s Registrar of Pesticides briefly banned several common pesticides containing the substances glyphosate and carbofuran in June 2011. However, a few months later, the ban was lifted on grounds that “the arsenic levels were too low to pose a serious threat” (Chavkin, 2012b). Investigative reporter Sasha Chavkin of the international NGO, Public Integrity points out that the ban was overturned even when WHO’s internal progress reports on CKDu in the NCP in June 2011 called for stronger regulation of “nephrotoxic agrochemicals” warning that any delay would cause “further accumulation of toxic agents in the environment . . . result[ing] in cumulative damage to the health of the people living in these areas” (Chavkin, 2012b). An internal Progress Report of June 2012 on CKDu in Sri Lanka by Dr. Shanthi Mendis, Senior Advisor and Coordinator, Chronic Disease Prevention and Management of the WHO in Geneva concluded that “contamination of the soil appears to be mainly from fertilizer and also from agrochemicals” (Mendis, 2012b). It recommended that the government strengthen the regulatory framework to improve quality control of imported agrochemicals, particularly with regard to nephrotoxic agents such as cadmium and arsenic, i.e. amendments to existing legislation, capacity strengthening for implementation and monitoring. (Mendis, 2012b)
Anuraddha Padaniya, President of the Government Medical Officers’ Association voices the opinion of growing numbers of Sri Lankans when he says that while tackling CKD “should be a national priority,” “vested interests” are “preventing strict policing of agrochemicals” (Countercurrents.org, 2012). On World Food Day, October 16, 2012, farmers from the NCP staged a protest in front of the office of the United Nations FAO in Colombo. The protest organized by the local NGO Swarna Hansa Foundation claimed that CKD in Sri Lanka is caused by chemical fertilizer use encouraged by the FAO, which supports the multinational agribusiness. The protesters demanded compensation for farmers suffering from CKD and an official ban on imported agrochemicals “with immediate effect” (H. Bandara, 2012).
In comparison with many other developing countries, the Pesticide Registrar in Sri Lanka has been successful in regulating pesticides. A regulatory mechanism was introduced in 1983 through the Control of Pesticide Act No. 33 of 1980 (Eddleton, Manuweera, & Roberts, 2003; Wijegunawardhana, 2010). However, as Michael Eddleston (Centre for Tropical Medicine, University of Oxford, United Kingdom), Gamini Manuweera (Office of the Pesticide Registrar, Government Department of Agriculture, Sri Lanka), and Darren Roberts (Division of Medicine, Royal Brisbane Hospital, Australia) have written in The Lancet, global financial realities make stricter regulation of agrochemicals difficult for the Sri Lankan Government: Industry resources dwarf those available to the government for regulation of pesticides. The size of the marketing department of one agrochemical company active in Sri Lanka is more than three times the size of the whole government regulatory department. It can be difficult to make big changes in complex social issues quickly, especially in view of the financial constraints faced by countries like Sri Lanka. (Eddleton et al., 2003)
Given growing public outcry, the Sri Lanka’s Ministry of Health finally released the final WHO Report on CKDu in early April 2013 (WHO, n.d.). Following recommendations in the Report, the Ministry of Agriculture banned the importation of the pesticides—Carbofuran, Chlorpyrifos, Propanil and Carbaryl—on April 8, 2013, and called for the reduction of the use of triple super phosphate fertilizer (ColomboPage, 2013). However, the battle over agrochemicals is far from over. The Registrar of Pesticides has not issued any “guidelines” on the issue and the banned pesticides are still available in the market and being used by farmers. Many of the leading agrochemical companies are interpreting the ban only as a “temporary measure” (Jayawardana, 2013). CKD and the battle over pesticides are not restricted to Sri Lanka’s dry zone agricultural region. These are global problems (Bandarage, 2013a).
A Global Problem
Like in Sri Lanka, today, the kidney disease epidemics in the Pacific Coast of Nicaragua and in Uddanam in the remote agricultural belt of Andhra Pradesh, India are also classified as mysterious diseases of “unknown etiology.” According to the WHO, more than 16,000 men died of kidney failure in Central America between 2005 and 2009 (Chavkin, 2012a; Conner, 2013). In Uddanam as much as 24% to 37% of the population in some villages are estimated to be affected by the disease (Chavkin, 2012b). The CKD epidemics in Sri Lanka, Nicaragua, and India have important features in common: The victims are farm workers; all suffer from “a rare form of kidney damage known as tubule-interstitial disease, consistent with severe dehydration and toxic poisoning”; few suffer from diabetes and hypertension, common risk factors for kidney disease (Chavkin, 2012b). CKD activists in Nicaragua see the sugar industry where most of the victims work as a root cause of the disease. According to the trade group for Nicaragua’s sugar companies, however, “the agricultural sugar industry in Nicaragua has no responsibility whatsoever for the spreading disease” (Aleman & Wessenstein, 2012). In 2006, the International Finance Group, the private sector arm of the World Bank, provided more than US$100 million to two privately owned sugar plantations in Nicaragua to promote sugar cultivation and biofuel production (Aleman & Wessenstein, 2012; Sanders & Seville, 2012). The workers at Ingenio San Antonio, one of the plantations funded by the Bank, however, have been protesting for close to a decade alleging that pesticide use and labor practices of the plantation have caused the disease (Chavkin, 2012a).
The search for causes and solutions to CKD whether in Sri Lanka, Nicaragua, India, or elsewhere must go beyond the bio-medical focus on the delineation of illness and treatment. To understand root causes, it is imperative to consider the industrialization of agriculture and the “consolidation of the entire food chain” by transnational corporations (Pesticide Action Network, 2013a). Through privatization of resources and technological domination, corporate control is being extended beyond the food chain to all of nature. The long-term result is not the promised progress and prosperity for all but structural violence—environmental degradation, poverty, ill health, and loss of livelihoods for the majority. These issues are discussed in the author’s book Sustainability and Well-Being: The Middle Path to Environment, Society and the Economy (Bandarage, 2013c).
In 1962, Rachel Carson warned in Silent Spring that “for the first time in the history of the world, every human being is now subjected to contact with dangerous chemicals from the moment of conception until death” (Benson, 2011; Carson, 1987). Today, the cycle of poison created by chemical agriculture envelops almost all life on earth—water, soil, air, plants, and animals—threatening the very survival of humans and the health of ecosystems. The Sri Lankan Government’s recent ban (August 2013) of imported milk powder from New Zealand that was allegedly contaminated with dicyandamide (DCD) is a case in point. An editorial in the Sri Lankan newspaper, Daily Mirror, voices growing public fear of poisoned food and drink when it says that Hundreds of people may be silently dying due to a daily intake of poisoned or polluted food. Even post-mortem examinations may not reveal the root cause . . . the verdict will be recorded as death due to natural causes. They are far from natural. In addition to the use of agro-chemicals, trans-national companies have invaded Sri Lanka with their genetically modified foods and terminator technology . . . The long-term effect may be the destruction of an agriculture system that has been part of our civilisation and culture for thousands of years. The . . . solution . . . is for the Government . . . to work out an effective national policy on food and nutrition. (Daily Mirror, 2013)
Policies on food and nutrition at the national level are not sufficient. The elimination of CKD and contamination of food and water call for a transformation of consciousness and an integrated global policy approach (Bandarage, 2013c). CKD is a complex issue requiring multi-dimensional, short- and long-term approaches. The struggle against toxic chemicals represents a challenge to the dominant model of development and its emphasis on economic growth and profits over environmental sustainability and human well-being. It calls for a fundamental shift from the dominant individualistic and competitive approach toward a partnership approach to human interaction with nature and with each other. The global movement away from industrialized agriculture, imported and fast foods toward organic agriculture, “food sovereignty,” and “slow food” are integral aspects of this shift (Amin, 2011; International Federation of Organic Agriculture Movements, 2013; Slow Food International, 2013)
Toward Sustainability and Well-Being
Unlike agribusiness, which pursues a fragmented, highly techno-bureaucratic approach, organic agriculture is an integrated approach that helps maintain an appropriate agroecological balance between the soil, water, people, animals, and insects. It depends on the use of local inputs such as indigenous seed varieties, compost, animal manure, and the cultivation of a diversity of crops. Organic agriculture also relies on the accumulated knowledge and skills of local farming traditions but can be dynamic and adapted to changing needs and circumstances (J. M. R. S. Bandara, 2009).
It may not be necessary to dismiss all aspects of industrialized agriculture or attempt to return to romanticized pre-modern agriculture. A range of alternatives to the chemical led approach to pest management can be considered. One is Integrated Pest Management (IPM) encouraged by the well-known international NGO, Care International in Sri Lanka (Care International, 1997; Uggalla, 1997). IPM seeks to maximize the use of safe, cheap, and simple pest control techniques by including organic traditional methods with the safest possible use of chemical pesticides where necessary. Another is Effective Microorganism (EM), a multi-purpose organic fertilizer and pesticide. It has been tried with much success in IPM projects in Sri Lanka including control of the brown hopper, which could not be contained by chemical pesticides (Bandarage, 1998; Uggalla, 1997).
Given farmers’ fear of economic survival and reluctance to give up chemical inputs, the switch to organic fertilizers and pesticides must involve a gradual process including research, advocacy, and public education. It calls for partnership among farmer producers, consumers, civil society groups, the government, intergovernmental organizations, such as the WHO and companies that are genuinely willing to support sustainable agriculture. Sri Lankan companies can play an important role in developing local organic alternatives to imported agrochemicals and food products, such as milk powder.
As shortages, prices, and contamination of food increases, more and more people across the world are joining the sustainable agriculture movement. In Sri Lanka, a number of international, national, and local governmental and non-governmental organizations are pursuing organic agricultural ventures. Efforts are under way in CKD prevalent areas to educate farming communities especially the youth on pesticides, kidney disease, and the need to shift to organic agriculture and safe use of water (Jayasumana, 2012). The concept of “learning through doing” relies on farmers’ ability to make appropriate decisions about pest management based on their own observations and discussions with each other and trainers (van den Berg, 2004). The objectives are to minimize use of chemical pesticides, increase agricultural yields and income of farmers, and restore their enthusiasm, self-confidence, and self-respect. Indeed, efforts to eradicate CKD in Sri Lanka and elsewhere are integral aspects of the global social movement toward environmental sustainability and human well-being.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.