
Abstract
Introduction
Surgical treatment of distal femoral fractures (DFFs) in osteoporotic bone is challenging despite improvements in hardware and surgical techniques. The occurrence and degree of secondary displacement during healing after bridging plate fixation are still unknown. This study aimed to assess the occurrence and degree of secondary displacement in healing DFFs in elderly patients and correlate the secondary displacement to body mass index, bone density, and weight-bearing regimen.
Patients and Methods
The study involved 32 patients, 65 years or older, with a DFF of AO/OTA types 33 A2-3, B1-2, C1-2, and 32(c) A-C,1-3, including peri-prosthetic fractures with stable implants. Twenty-seven patients had at least 8 weeks of follow-up, and 21 patients had a complete 1-year follow-up. Minimally invasive surgery was performed using a distal anatomical femoral plate as a long bridge-plating construct. Secondary displacement was assessed with computed tomography of the entire femur postoperatively and at 8, 16, and 52 weeks. Femoral length, coronal angulation (varus/valgus), and subsidence as the change in distance between the distal joint surface and a specified locking screw were measured.
Results
There was a statistically significant mean femoral shortening at 52 weeks of 4.7 mm (SD 3.9, (95% CI 2.9–6.5), P < 0.001) mainly by subsidence of the distal fragment. Most patients experienced limited coronal angulation. There was no correlation between body mass index or bone density and secondary displacement. At the 1-year follow-up, no patient needed revision surgery for non-union or plate breakage. Restricted weight-bearing for 8 weeks did not prevent secondary displacements or adverse events such as cut-outs.
Conclusion
Modern dynamic plate osteosynthesis could not prevent commonly occurring fracture subsidence in DFF in an elderly cohort. Restricted weight-bearing for 8 weeks did not prevent secondary displacements or mechanical adverse events.
Introduction
The incidence of distal femoral fractures (DFF) in the elderly is increasing, mainly because of the growing aged population.1-3 In this age group, surgical treatment is frequently complicated by previous surgery and femoral implants,2,4,5 and also age-related deterioration of bone quality that will affect osteosynthesis stability.6-9 Anatomical distal femoral locking plates are standard treatment, as they also can be used for peri-implant fixation.9,10 When applied as a long bridging plate, biomechanical advantages include lower incidence of loss of fixation, more flexibility, and better capability to withstand permanent deformation.11-14
Although fracture subsidence of the metaphyseal fragment or even cut-out of the osteosynthesis is common in osteoporotic bone in other locations such as hip and proximal humerus,8,15-17 it has not been perceived as a problem in DFF. In DFF, metaphyseal migration and cut-outs have been studied mainly in experimental models.12,18,19 Still, only one study has been published on secondary displacement during the healing phase of DFF. 20 Increased knowledge of secondary displacement in a strictly bridging plate fixation in elderly patients with osteoporotic bone is therefore needed.
The primary aim of this study was to assess if secondary displacement was common during healing in a cohort of elderly patients treated for a DFF with a bridging distal femur locking plate. Secondly, the correlation of secondary displacements to body mass index (BMI), bone mineral density (BMD) and postoperative restricted weight-bearing was evaluated.
Patients and Methods
This study evaluates unpublished secondary outcomes from a published randomised controlled trial which investigated the influence of weight-bearing regimens on patient-reported outcomes in surgically treated elderly patients with DFF. Thirty-two patients were allocated to either immediate full weight-bearing (FWB) or partial weight-bearing (PWB) for 8 weeks. 21
Inclusion criteria were patients 65 years or older who suffered a traumatic fracture of the distal part of the femur of AO/OTA types 33 (A2-3, B1-2, C1-2) or 32(c) (A1-3, B2-3, C2-3). Periprosthetic fractures with stable implants were also included according to the unified classification of periprosthetic fractures of types IV (3B1, 3C-D and V. 3B1, 3C-D). 22 Exclusion criteria were open fractures of types II and III according to the Gustilo-Andersson classification, 23 concurrent injuries or pre-existing conditions that could substantially affect postoperative rehabilitation, inability to ambulate independently with or without walking aids, or severe cognitive impairment (≤ 6 points) according to the Short Portable Mental Status Questionnaire. 24 Eligible patients giving informed consent to participate in the study were included and surgically treated according to a standardised surgical protocol. The follow-up of the study was 1 year.
For the current analysis, all patients with an immediate postoperative and minimum 8 weeks postoperative computed tomography (CT) scan were included (n = 27). Two patients who died before the 8-week follow-up and three patients having no or incomplete postoperative CT scans were excluded. Twenty-one patients completed the 1-year follow-up.
AO/OTA Classification.

AO/OTA; Arbeitsgemeinschaft für Osteosynthesefragen/Orthopedic Trauma Association, UCPF; Unified Classification System for Periprosthetic Fractures.
Twenty-three patients had dual-energy X-ray absorptiometry (DXA) measurements available (hip or lumbar). Two patients’ BMD was normal; eight were osteopenic, and 13 were osteoporotic.
Surgery according to a defined protocol was performed within 72 hours of hospital admission. A 15-hole LCP® Distal Femoral Plate (Synthes™, Oberdorf, Switzerland) was used except for short patients, where a 13-hole plate was used. After closed reduction on a traction table, a short incision was used to introduce the plate, which was held with a large clamp against the lateral condyle. Five bi-cortical locking screws were used in the distal part of the plate, and three bi-cortical locking screws in the proximal portion of the plate, the latter through stab incisions. If the patient had a hip replacement with thin bone around the stem, a LAP® Lateral Attachment Plate (Synthes™, Oberdorf, Switzerland) was used for proximal fixation. No screws or cerclage wires were used across the fracture site. 25
CT scans of the entire femurs were done with a metal-artefact reconstruction algorithm and archived as 3-mm contiguous slices. The index scan was performed within 1 week postoperatively. Scans at 8, 16, and 52 weeks assessed secondary displacement. All measurements were made twice by the first author (MP), 6 months apart, using the multiplanar reformations (MPR) tool of Xero Viewer (web-based software) (AGFA, Mortsel, Belgium). Missing CT scans during follow-up are shown in Table 2.
Femoral length was measured in a coronal plane parallel to the most dorsal part of the femur condyles. CT slice thickness was set to 50 mm to facilitate the determination of the femoral outlines. The distal reference was the line joining the distal aspects of the joint surfaces of the femoral condyles. The most cranial outline of the femoral head was used for proximal reference. The coronal plane angle was measured on the same coronal section but between the line joining the femoral head centre with the knee’s intercondylar centre and the line between the distal aspects of the femoral condyles (Figure 1). A; The length and coronal angulation were measured on a 50-mm thick CT slice parallel to the dorsal surfaces of the femoral condyles. A line joining the most distal part of the joint surface of the condyles was used for distal reference. The proximal measuring reference for length was the most proximal part of the femoral head. B; Coronal angle measurement a° the centre of the femoral head.
Subsidence of the metaphyseal fracture fragment relative to the plate construct was measured as the distance between one specified locking screw (the most proximal one of the distal screw cluster) and the most distal point of the joint surface of the medial and lateral condyle (Figure 2). Femoral shortening > 10 mm and/or coronal angulation increased > 3° were considered a significant secondary displacement. Measurement between a specified locking screw and the most distal joint surface. Missed Computed Tomography Scans.

Statistical Analysis
SPSS 28 (IBM, New York, USA) was used for statistical analysis. Continuous data were analysed using a Q-Q plot to evaluate normality. Normal distributions are presented as mean and standard deviation (SD). Student’s t-test was used to assess paired statistical differences. The Mann-Whitney U test was used when comparing subgroups due to the small and not normally distributed sample size. Fisher’s exact test was used to compare categorical data. Statistical significance was set at P < 0.05. Spearman rank correlation coefficient (CC) was used for correlation analysis. Intraclass correlation (ICC) was used to calculate the accuracy and intra-observer agreement of the CT measurements. 26
Results
Fracture Subsidence During Follow-Up.

aStatistically significant difference comparing neighbouring follow-ups, p< 0.05.

Femoral shortening. The numbers indicate individual patients with adverse events or increased secondary displacements (Table 4). (PWB; partial weight-bearing, FWB; full weight-bearing).
Coronal angular alterations (valgus and varus) significantly increased during follow-up (Table 3). The angulation typically made the initial varus or varus angulation more pronounced (Figure 4). At the 16-week follow-up, the coronal angle had increased more than 3° (varus or valgus) in 4 of 25 patients. Alterations in varus/valgus angulation. The numbers indicate individual patients with adverse events or increased secondary displacements (Table 4). (PWB; partial weight-bearing, FWB; full weight-bearing).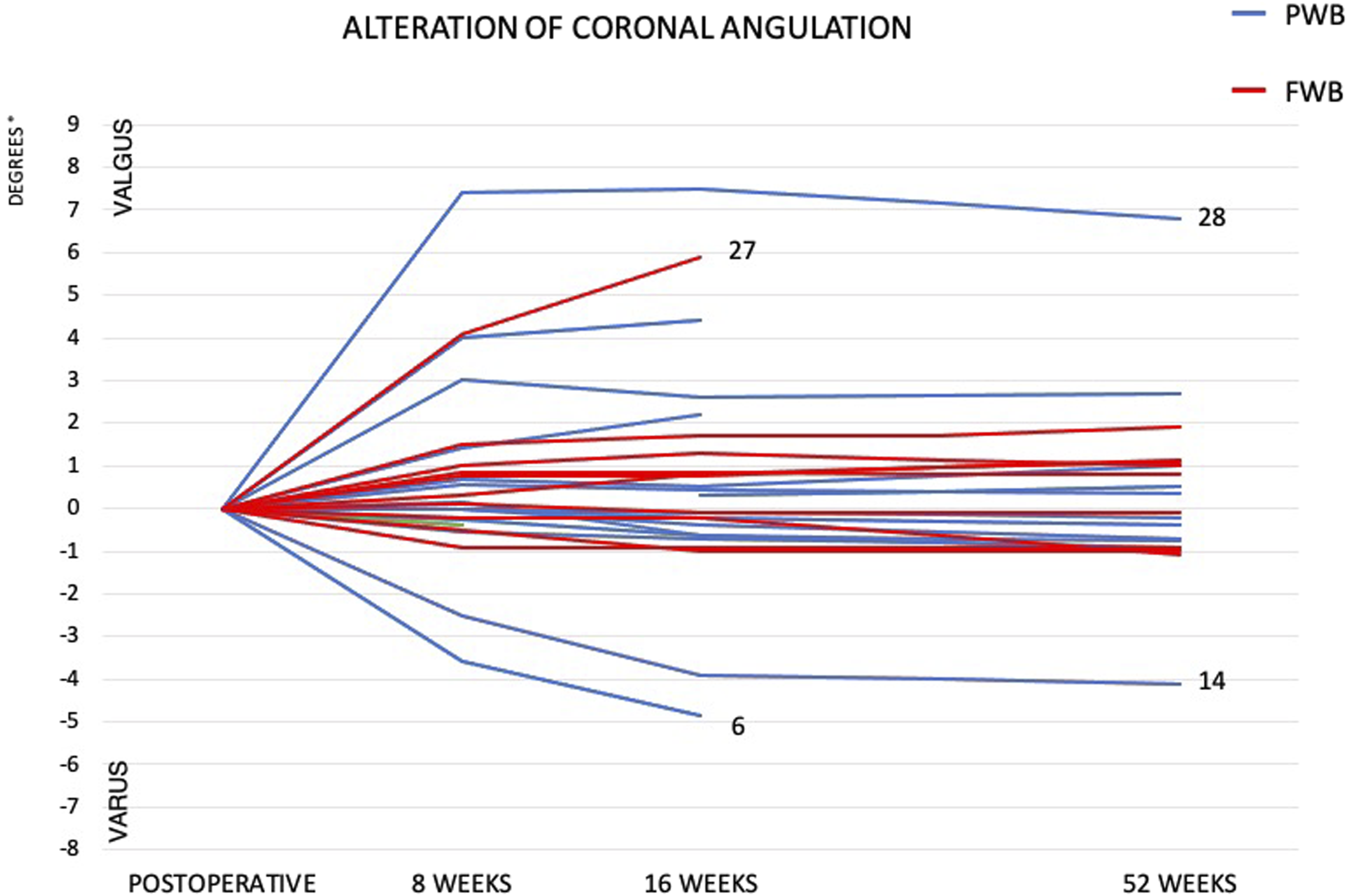
Adverse Events and Significant Secondary Displacments.

AO/OTA; Arbeitsgemeinschaft für Osteosynthesefragen/Othopeadic Trauma Association.

A, Case 28 with severe osteoporosis, allocated to PWB; B, C, postoperative radiographs; The patient suffered a secondary Hoffa fracture of the lateral condyle 1 week postoperatively and later collapse of the medial condyle. The most distal screws were removed 8 months postoperatively. D, E, radiographs at the 52-week follow-up.
One patient with a TKR experienced an accentuated valgus angulation of 6° (Table 4).
All fractures healed during the 1-year follow-up without revision for non-union or plate breakage. One patient with delayed healing was diagnosed with an atypical non-bisphosphonate fracture and was later diagnosed with renal failure.
There was significantly greater femoral shortening at the 52-week follow-up in the PWB group than in the FWB group of median 4.0 mm (SE 14.0, 95% CI (0.5; 4.5), P = 0.023), without significant difference in coronal angulation or secondary displacements at the medial or lateral condyles comparing weight-bearing groups. Adverse events and significant secondary displacements were more frequently observed in the PWB group, although this difference was not statistically significant. BMD or BMI did not correlate with secondary displacement,
The intra-observer agreement results of the measurements for total femur ICC were 0.999 (95% CI 0.999-1.000), and results for condyles vs locking screw ICC were 0.998 (95% CI 0.996-0.999). ICC for varus/valgus was 0.979 (95% CI 0.955-0.990).
Discussion
Secondary displacement with a statistically significant femoral shortening was common in this cohort of elderly patients. A mean femoral shortening of almost 5 mm, mainly due to subsidence of the distal fragment, is unlikely to be clinically relevant but, importantly, indicates a likely path for mechanical adverse events. General BMD or BMI did not correlate to fracture subsidence. Restricted weight-bearing did not prevent secondary displacement, and there was a significantly larger femoral shortening in the PWB group.
To our knowledge, only one previous clinical study has assessed the fracture stability of DFFs treated with a lateral locking plate. 20 In that study, radio-stereometric analysis (RSA) was used to measure inducible motion and permanent migration of the metaphyseal fragment during fracture healing. Their 16-patient cohort was younger (mean age 70 years), and the fixation construct was more rigid with a shorter plate. A permanent shortening of the femur was found of the same magnitude as in the present study. In contrast to the present study, two patients required revision of non-unions. The absence of non-unions in our series may be attributed to the different dynamics of the fixation. The minimally invasive bridge plating osteosynthesis used in this study, leaving the fracture site untouched, has been described as beneficial for fracture healing. 28 In addition, the cut-out risk using a fixation with dynamic behaviour is probably lower than when a rigid implant is used.
Only two out of six patients with mechanical adverse events underwent secondary surgery during the follow-up of this study (Table 4). This can be attributed to the nature of the mechanical adverse events. An increased varus or valgus angulation of the distal fragment or screw cut-outs does not necessarily require revision surgery of the fracture itself. Instead, a total knee replacement (TKR) may be required once the fracture has healed.
The fracture subsidence of the total femur of nearly 5 mm on average after 1 year of follow-up is not considered clinically significant on a group level in this age group. 29 However, patients who experienced a mechanical adverse event (as shown in Table 4) during the follow-up are believed to have clinically affected function, increased discomfort, and pain. Fracture subsidence occurred mainly at the distal fixation in the study, with screw migration in cancellous osteoporotic bone leading to mechanical adverse events such as cut-outs and fixation failures.30,31 The results of this study are therefore clinically important; they show that restricted weight-bearing did not prevent screw migration or mechanical adverse events in the cancellous bone of the metaphysis. In fact, the restricted group experienced significantly greater fracture subsidence.
Ricci et al. 32 reported BMI (> 30) to be a risk factor for adverse events in plate fixation of DFF. However, in the current study, BMI did not correlate with adverse events or secondary displacement. Furthermore, secondary displacement did not correlate with a higher degree of general osteoporosis in this study, which correlates with similar findings reported in previous studies. 33 It is primarily regional osteoporosis which increases the risk of secondary displacement and mechanical adverse events.16,34 Unfortunately, we were not able to evaluate regional osteoporosis at the fracture site in this study.
Restricted weight-bearing during 8 weeks did not protect the integrity of the fixation against secondary displacement or adverse events in this study, and similar results have been reported in recent retrospective reports.10,35 Secondary displacement and adverse advents are most likely caused by disuse inducing a local loss of bone mass enough to affect the integrity of the microstructure and, thereby, the mechanical properties of metaphyseal bone.36,37 Considering the lack of evidence in favour of restricting weight-bearing in elderly patients with DFF and the small but growing body of studies indicating an increased risk of mechanical adverse events in weight-bearing restricted patients, the benefit of restricted weight-bearing should be questioned.
There are limitations to the present study. The number of patients is limited, although larger than in the only previous clinical study measuring secondary displacement during healing of DFF. Measurements on osteoporotic bone can be difficult, and the precision of the measuring technique did not allow for measurements of rotational and sagittal displacements. ICC was chosen to assess the reliability of length and coronal angulation, and the agreement was high. However, inter-rater reliability was not determined, which could be seen as a limitation. The mean age of the patients in this study was high, and a large proportion had had previous surgery. However, DFF patients are predominantly elderly in Western societies.2,4,5
Conclusion
Secondary displacement with femoral shortening was common in DFF in elderly patients despite modern dynamic plate osteosynthesis. No correlation was found between the degree of general BMD or BMI and secondary displacements. Restricted weight-bearing for 8 weeks did not prevent the fracture from secondary displacements; interestingly, there was a significantly larger femoral shortening in the restricted weight-bearing group at 52 weeks. In addition, a nonsignificant increase in mechanical adverse events, such as cut-outs, was seen in the restricted weight-bearing group. The benefit of restricted weight-bearing in elderly patients with DFF should be questioned.
Footnotes
Author Contributions
MP: Conception and study design, acquisition, analysis and interpretation of data, drafting and revising the article.
CE: Conception and study design, interpretation of data, revising the article for intellectual content, drafting and revising the article
OR: Interpretation of data, drafting and revising the article
RT: Interpretation of data, drafting and revising the article
MG: Conception and study design, interpretation of data, revising the article for intellectual content, drafting and revising the article
All authors have given final approval for this version to be submitted.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.