
Abstract
Background
Restricted weight-bearing is still used after lower extremity fracture surgery in elderly patients. The long-term effect on gait recovery in elderly patients with distal femur fractures (DFF) and their ability to comply with the restrictive weight-bearing regime is unknown. This study aimed to investigate the effect of restricted postoperative weight-bearing on gait recovery (actual weight-bearing and cadence) during a 1-year follow-up.
Methods
This study evaluated secondary outcomes from a randomized controlled trial (32 patients ≥65 years, with a traumatic DFF). Internal fixation was achieved using an anatomical lateral plate. Patients were allocated to either immediate full weight-bearing (FWB) or partial weight-bearing (PWB) (30% of body weight) for 8 weeks. Pressure-sensitive sensors (F-scan™ system, Tekscan, Massachusetts, USA) were used to measure weight-bearing and cadence postoperatively and at 8-, 16-, and 52-week follow-ups. Twenty-six patients with at least 1 measurement were included.
Results
There was a statistically significant difference in actual weight-bearing between the PWB and FWB groups postoperatively of 32.3% (95% confidence interval CI, −50.0; −13.0, P < .001) and at the 8-week follow-up of 36.8% (95% CI −61.0; −18.0, P = .01), but not at later follow-ups. The PWB group presented a consistently lower cadence compared to the FWB group, which was statistically significant at the 16-week follow-up with 9.0 steps/min (95% CI -16.2; −1.1, P = .047) and 52-week follow-up with 9.3 steps/min (95% CI −18.0; −3.9, P = .009).
Conclusions
Restricting postoperative weight-bearing in elderly patients with a DFF had a significant effect on postoperative weight-bearing. The effect lingered with a delayed return to FWB and persistent significantly lower cadence in the PWB group. These findings suggest that even temporary weight-bearing restrictions most likely have negative long-term effects on gait function at 1 year and, therefore, cannot be recommended.
Keywords
Background and Introduction
Different weight-bearing protocols for optimizing fracture healing in distal femur fractures (DFF) have been used for decades. 1 Partially restricting weight-bearing postoperatively is meant to be a compromise between offloading the fracture to protect the osteosynthesis while maintaining function and independence during rehabilitation. 2 Although of debated value, 3 it is still used in DFF. 4 Recent research indicates that restricting postoperative weight-bearing in elderly patients with lower extremity fractures could have negative long-term effects on recovery and increase mortality.5-7 Other studies have also reported that restrictive weight-bearing in elderly patients did not decrease the rate of complications or, in fact, even increased complication rates.3,6,8-11
Recovery of gait function is a central goal in the rehabilitation after a lower limb fracture, as it is essential for recuperation to the preinjury level of function and independence. 12 Reduced gait function and speed also predict future adverse health outcomes and death.13,14 In the elderly patient, recovery is slower and less complete than in younger age groups 15 when assessed as the ability to perform physical activities of daily life and usually reaches a steady plateau at 1 year after a hip fracture. 16
Several reports have demonstrated the difficulties for individuals to follow restricted weight-bearing instructions, not only in patients with injuries but also in healthy subjects regardless of age.17-20 Studies on geriatric patients with hip fractures show a low ability to comply with restricted weight-bearing protocols in the early postoperative phase.5,21,22 The compliance is even lower after a 6- to 8-week period of weight-bearing restrictions for both patients with lower extremity fractures and hip replacements.19,23-25 Studies on elderly patients with DFFs have, to our knowledge, not been published.
Despite the potential impact of restricted weight-bearing on pre-existing functional impairment, comorbidity, sedentary behavior, and sarcopenia in the elderly,26-28 there are no studies beyond the early postoperative period on elderly patients with DFFs. It is, therefore, essential to investigate the long-term impact on actual weight-bearing and gait following weight-bearing restrictions in this group of patients.
This study aimed to investigate whether a period of restricted postoperative weight-bearing had a long-term effect on gait recovery (actual weight-bearing and cadence) for elderly patients with DFFs during a 1-year follow-up period. To differentiate between actual weight-bearing and the effects of the imposed weight-bearing restrictions, the secondary aim was to assess the ability of these patients to adhere to the restricted weight-bearing protocol.
Methods
Study Design
This study evaluated previously unpublished secondary outcomes from a randomized controlled trial investigating the influence of weight-bearing regimens on patient-reported outcomes following surgically treated elderly patients with DFFs. 29 Between January 2013 and June 2016, 32 patients were allocated to immediate full weight-bearing (FWB) or partial weight-bearing (PWB) regimens for 8 weeks.
Inclusion criteria were patients aged 65 years and older with a traumatic DFF. Exclusion criteria were prior physical impairment that could significantly affect the postoperative rehabilitation, concomitant injuries or ongoing systemic infections, pathological fractures, alcohol or drug abuse, and the inability to walk independently before the injury. The need for walking aids such as crutches or walkers did not exclude participation. In eligible patients, intellectual status was screened with the short portable mental status questionnaire (SPMSQ). 30 Patients with a score of ≤6 were excluded, as well as patients unable to communicate in Swedish.
Three patients declined participation in this study, 1 died postoperatively, 1 sustained a secondary coronal femoral condyle fracture postoperatively and could not be mobilized to walking, and 1 was missed for postoperative measurement and then lost to follow-up, leaving 26 patients for analysis with at least 1 measurement. Of the 26 patients, nine were randomized to the FWB group and 17 to the PWB group. The unevenly sized groups resulted from using a simple randomization web-based software.
All patients were surgically treated using a standardized surgical protocol with a mini-invasive plate-osteosynthesis (MIPO). A long lateral anatomical bridging plate was used for fixation.
Patients randomized to PWB were instructed to bear 30% of their body weight on their fractured leg up until the 8-week follow-up but were allowed to fully weight-bear at the 8-week measurement. Patients in the FWB group were allowed to bear 100% of their body weight as tolerated from the first postoperative day. Physiotherapists gave standard postoperative instructions regarding rehabilitation and weight-bearing directly after the operation. Once discharged, physiotherapy continued in an outpatient setup, customized for each patient depending on their living conditions.
Demographic and Patient-Related Data.

BMI; Body mass index, ASA; American Society of Anaesthesiologists, FRS; Function recovery score.
Gait Measurement
The postoperative weight-bearing measurement was performed 5 days postoperatively before hospital discharge and at 8-, 16- and 52-week out-patient follow-ups. An in-shoe pressure sensing system, F-scan™ (Tekscan, Massachusetts, USA), was used. The wireless setup comprised a belt connected to the in-shoe pressure sensors worn by the patient and a computer provided with F-scan Clinical 6.7 software™ (Tekscan), which enabled the patient to walk unrestricted within 5 meters of the computer (Figure 1). The F-scan™ system (Tekscan Massachusetts, USA) has in-shoe pressure sensors, connecting cables, a belt with a battery holder, and a wireless transmitter.
The patients used the same pair of walking shoes for each measurement. Ten different-sized new shoes (only used for measurements in this study) were available. Damaged sensors presented as missing areas of the footprint on the screen of the F-scan™ software, and when noticed, sensors were replaced. They were sandwiched between the inner sole and the shoe to protect the sensors from being damaged.
Calibration
New F-scan™ sensors were used for calibration in a Tekscan™ Equilibration device.32,33 An individual calibration was performed for each patient. Using the foot contact area (provided by the F-scan™ system) and the patient’s weight, the individual pressure (kPa) could be calculated.
Measurements
The patients were asked to wear shoes fitted with sensors for about 5 minutes to warm up the sensors and perform 3 walking series. The system needed the patient to complete at least 4 support phases of each foot to calculate a valid series.
The data was analyzed with F-scan research™ software. The first and last steps (stance phase) were discarded (default setting by the software). Each session’s mean vertical peak ground reaction force (GRF) gave the actual weight-bearing measurement. Cadence was calculated by measuring the mean time for 3 consecutive steps (complete walking cycles, both stance and swing phases) of the fractured leg and was used in this study as an equivalent for gait speed. 34
Missed Measurements During Ther Follow-Up Period.

Statistical Methods
SPSS version 29 (IBM, Illinois, USA) was used for statistical analyses. A Q-Q plot was used to assess the normality of the data distribution. Normally distributed data are presented as mean and standard deviation (SD). Due to small sample sizes, the Mann-Whitney U test was used to calculate statistically significant differences between groups.
Results
Weight-Bearing Measured in Percent of Fractured Leg Compared to Unfractured During
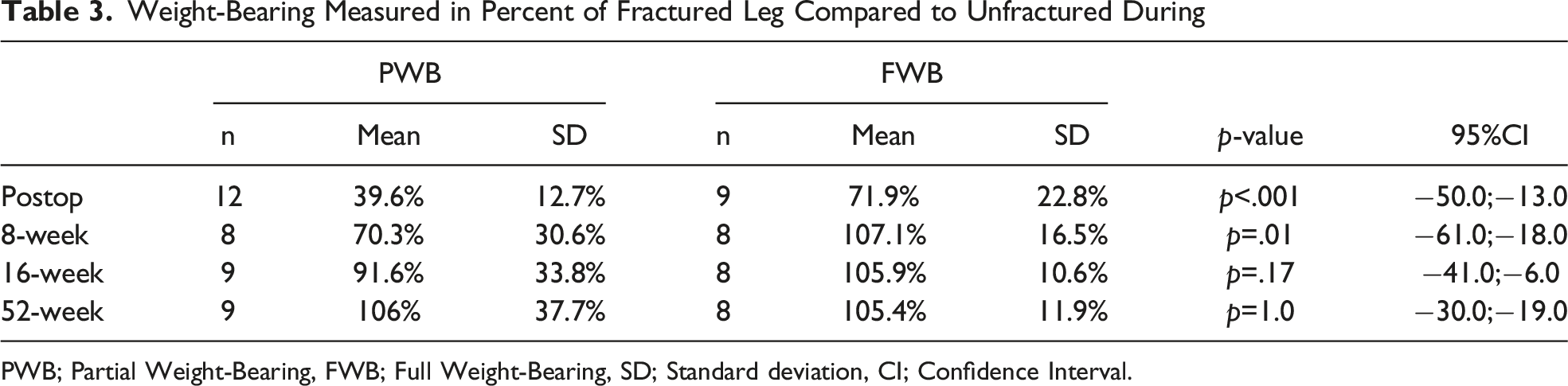
PWB; Partial Weight-Bearing, FWB; Full Weight-Bearing, SD; Standard deviation, CI; Confidence Interval.
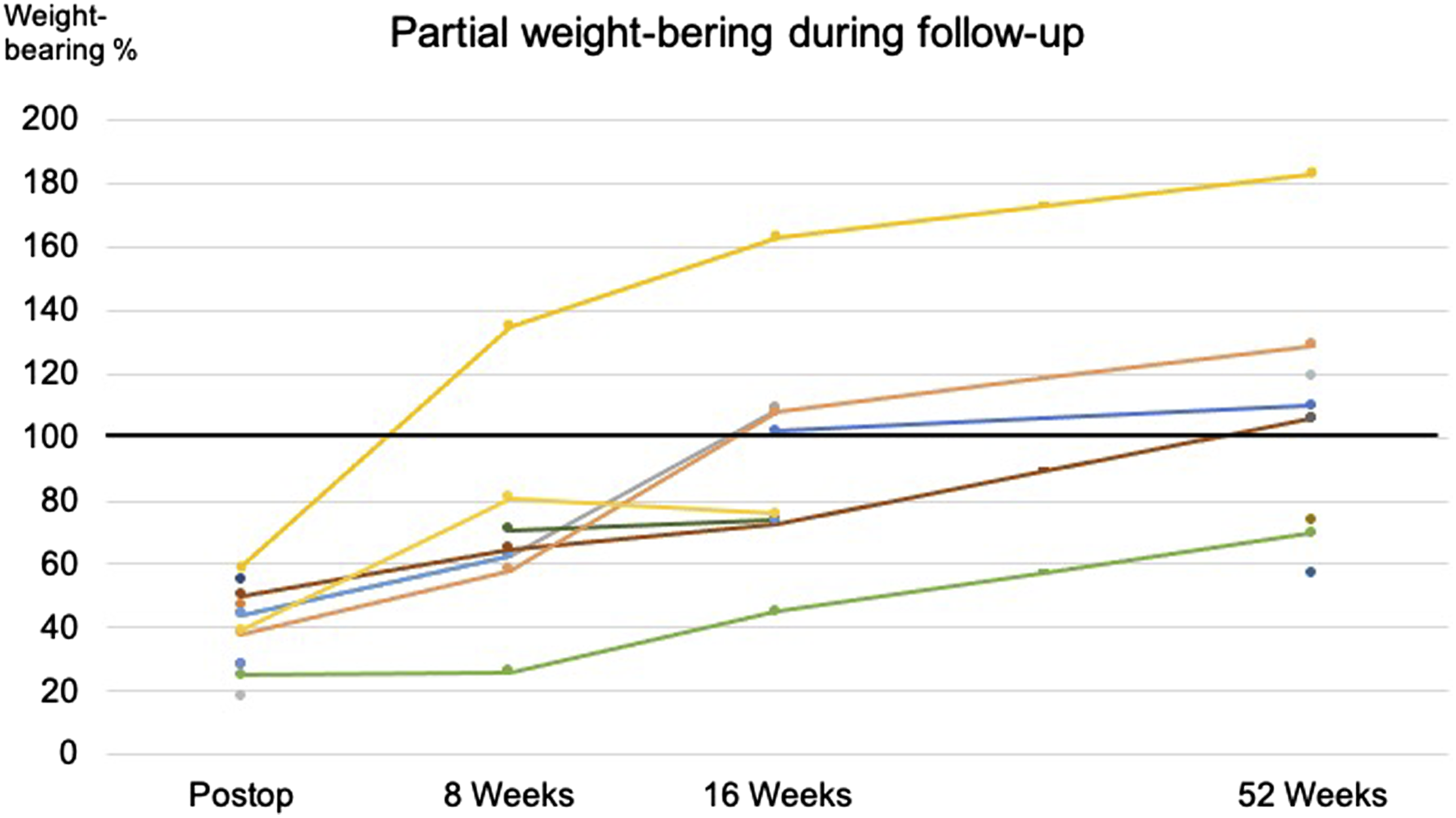
The individual time course for each patient of the partial weight-bearing regimen during follow-up. Equalized weight-bearing difference between the fractured and the unfractured leg is seen first between the 16- and the 52-week follow-up.

The individual time course for each patient of the full weight-bearing regimen during follow-up. Equalized weight-bearing difference between the fractured and the unfractured leg is seen at the 8-week follow-up.
Cadence (Steps/Minute) of Fractured Leg During Follow-Up.

PWB; Partial Weight-Bearing, FWB; Full Weight-Bearing, SD; Standard deviation, CI; Confidence Interval.

The mean cadence, per group, with standard error bars measured as steps per minute during follow-up. A consistent difference throughout the follow-up period is seen between the PWB (blue) and FWB (orange) groups, which was statistically significant at the 16-week and 52-week follow-ups (*).
Discussion
The present study investigated both weight-bearing and cadence from 5 days postoperatively to the final follow-up at 52 weeks in elderly patients with DFF. The patients in the PWB group clearly had a slower recovery of weight-bearing ability than those in the FWB group. At the 52-week follow-up, gait function, measured as cadence, was still significantly lower in the PWB group than in the FWB group. Thus, restricted weight-bearing, even for a limited period, appears to limit the long-term functional outcome following DFF in this population.
To our knowledge, no reports have been published on elderly patients with DFFs studying postoperative compliance or the long-term effects on gait recovery with different weight-bearing regimens. Instead, patients with proximal femur fractures with similar demographics (age, comorbidities, and risk of mortality) as patients with DFFs can be used for comparison.35,36 Even so, gait (speed or cadence) and actual weight-bearing recovery after a period of restricted weight-bearing have not been studied beyond 6 weeks. 24 However, restricted weight-bearing for 2 to 4 weeks in patients with hip fractures was found to be a strong negative determinant. 37 A registry study assessed modifiable predictive factors affecting the probability of regaining pre-fracture ambulation in 25607 hip fracture patients. It was concluded that in addition to performing surgery in less than 24 hours with early mobilization, allowance of early full weight-bearing was crucial for recovery. 38
Apart from having negative long-term effects on recovery, imposed restricted weight-bearing is also challenging to achieve for elderly patients with hip fractures. Pfeufer et al. 5 found that patients with restricted postoperative weight-bearing had lower mobility and gait speed at 5 days post-surgery than those without restrictions, even though their actual weight-bearing was not different from that of patients allowed FWB. Unfortunately, no long-term follow-up was done. In the present study, most patients in the PWB group could not comply with the weight-bearing limitation. However, there was still a significant difference between the groups (40% vs 72%) at the postoperative measurement, indicating that the patients tried to comply with the restrictions.
In a study by Koval et al. 39 on patients with hip fracture, it was shown that most patients voluntarily self-limited their weight-bearing to 60-80% of their body weight during the early postoperative period, similar to the FWB group in the present study. Only 32 of the 60 included patients completed the 12-week study duration in their study, but the reasons for the missing measurements are not reported. Thingstad et al. 40 conducted an RCT on 2 rehabilitation strategies (comprehensive geriatric care vs orthopaedic care) after hip fractures. They found that participants with a low preinjury function level were more likely to be lost to follow-up than those without. In the current study, FRS 31 was used for assessing preinjury function, and of the 5 patients lost to follow-up at 52 weeks, all were in the PWB group. Two were deceased, and 3 declined further participation. The mean FRS in the lost-to-follow-up group was 98.4% which does not indicate a low preinjury function as a likely reason in the present study.
The recovery of weight-bearing ability after a period of restricted weight-bearing in elderly patients with lower limb fractures has not been studied previously. In the current study, patients in the FWB group had regained their ability to fully weight bear at 8 weeks. In the PWB group, the patients were significantly slower to recover, and some showed improvement also after the 16-week follow-up. From hip fracture patients, it is known that gait speed is lower still after 2 years, 41 but the value of early mobilization and extended rehabilitation appears clear.40,42
The likely reason for the adverse long-term effects on recovery after restricted weight-bearing, particularly in the elderly, is advanced age in combination with metabolic conditions, such as diabetes or physical inactivity, which can induce and worsen sarcopenia. Sarcopenia is a significant loss of muscle mass and strength that negatively affects, eg, walking speed. 43 Sarcopenia is common in elderly patients, and 71% of patients with hip fractures have it. 26 In elderly patients who might already be compromised and have small margins, a comparatively short period of disuse can have a profound effect on metabolic health and muscle atrophy and induce a negative spiral of events, increasing the risk of irreversible metabolic changes, new falls, other complications, and death.27,28,44
Limitations
Although, to date, this is the only study that has assessed long-term weight-bearing and gait patterns during rehabilitation after a DFF, it has several shortcomings. The randomization process should diminish or even rule out confounding factors such as age, 45 some minor differences were, however, observed between the groups. 46 At admission, the median age in the PWB group was 81 years vs 83 years in the FWB group. The mean ASA score was 2.41 in the PWB group and 2.11 in the PWB group, and the FRS score was 94.8% in the PWB group and 97.8% in the FWB group. These differences were, however, not statistically significant and less likely to affect the results. The randomization process was simple without randomization blocks, which led to unevenly sized groups with potentially reduced study precision. 46 In the present study, there were missing measurements and patients lost to follow-up which could potentially cause bias. 47 The versatile and portable F-scan™ in-shoe pressure system was chosen for evaluating weight-bearing. 48 Unfortunately, technical problems contributed to missed measurements.
Conclusion
The restriction of postoperative weight-bearing in elderly patients with a DFF in this study resulted in a significantly delayed recovery of weight-bearing ability and gait (cadence). Importantly, even at the 1-year follow-up, the PWB group still had a significantly lower cadence than the FWB group. Our findings demonstrate an underestimated risk of negative long-term effects on the gate function recovery associated with postoperative weight-bearing restrictions in DFF. Restrictive weight-bearing should be avoided in this group of patients.
Footnotes
Author Contributions
All authors contributed to the study’s conception and design. Martin Paulsson performed material preparation, data collection and analysis, and first draft writing. All authors revised and edited the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Grants from the Swedish state financed the equipment for the study under the agreement between the Swedish government and the county councils (ALFGBG-432511).
Ethical Approval
The study was approved by the Regional Ethical Review Board in Gothenburg (registration number 008-12) and performed in line with the principles of the Declaration of Helsinki.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Disclosure
None of the authors has or will receive benefits for personal or professional use from a commercial party related directly or indirectly to the subject of this article.
Clinical Trial Registration
This study was entered on December 4, 2012, in a regional clinical trial registry (registration number 115861) under the Healthcare Committee, Region Västra Götaland, Sweden.