
Abstract
Purpose
To examine five-year trends in 30-day readmission and length of stay (LOS) among the geriatric population after surgical fixation for hip fracture in a large database model.
Methods
Patients ≥ 65 years of age in the American College of Surgeons National Surgical Quality Improvement Program Targeted Hip Fracture (ACS-NSQIP THF) were identified using Current Procedural Terminology (CPT®) codes 27 236, 27 244, 27 245 for intramedullary nailing or Open Reduction and Internal Fixation (ORIF) of fractures involving the femoral head, neck, peritrochanteric, intertrochanteric, and subtrochanteric regions. The primary outcome was incidence of ≥1 30-day hospital readmission and secondary outcome was total hospital length of stay in trend analysis.
Results
Overall, there were 64 794 patients who met inclusion criteria, of which 7.85% (95% CI: 7.64% to 8.05%) were readmitted within 30 days of hip fracture surgical fixation. The proportion of patients with ≥1 30-day readmission were presented over time and Cochran-Armitage Trend Testing indicated a statistically significant decreasing trend in the 30-day readmission incidence from 2016-2021 (P < 0.0001). The mean absolute change in incidence from year-to-year was −0.24% (mean relative change, 0.97) and the total absolute difference in incidence from 2016 to 2021 was −1.20% (relative difference, 0.85). LOS data were missing for 1048 cases (1.62%). Mean and median length of stay data was similar across all years.
Conclusion
The probability of having ≥1 30-day readmission decreased 0.85-times from 2016 to 2021, with a statistically significant downward trend over time. There were no meaningful changes in length of stay. Healthcare providers, policymakers, and stakeholders can utilize these findings to implement initiatives that enhance value-based care in hip fracture management and benchmark institutional metrics, ultimately improving patient outcomes and optimizing healthcare resources.
Introduction
Hip fractures in the geriatric population are common orthopaedic injuries that represent a significant public health concern due to their association with substantial morbidity, mortality, and healthcare expenditures.1-3 In fact, recent cost-analyses estimate the direct medical costs could approach $446.3 billion by 2050.4-6 As the population continues to age, the burden of hip fractures becomes increasingly pronounced, emphasizing the need for a comprehensive understanding of contemporary trends in hip fracture outcomes to inform effective and value-based care strategies. Recently, there has been a nationwide push to optimize care for geriatric hip fracture patients, aimed at reducing complications and improving recovery. This has included the implementation of multidisciplinary care models, such as orthogeriatric co-management programs, which integrate orthopedic and geriatric expertise to optimize patient outcomes.7,8 Additionally, standardized pain management protocols and early mobilization pathways have been increasingly adopted, with the aim of enhancing functional recovery and minimizing complications9,10 Although studies have examined hip fracture outcomes in the past, there is a dearth of recent literature assessing these trends.11-13 Therefore, there is a critical need to investigate current patterns of 30-day readmission and length of hospital stay (LOS) among older adults who have undergone surgical fixation for hip fractures.
Hip fractures in older adults not only lead to immediate consequences but also have long-term implications for patients' overall well-being.14-16 The incidence of complications, such as readmission, can further exacerbate the already considerable morbidity associated with these fractures. Understanding the current landscape of readmission rates following surgical fixation is crucial for identifying areas of improvement and implementing targeted interventions. By analyzing the temporal trends in readmission rates, healthcare providers can gain insights into the effectiveness of existing interventions and develop novel strategies to reduce readmission rates and associated healthcare costs.
In addition to readmission rates, LOS is another important outcome measure that provides insights into the efficiency of care delivery and resource utilization. 17 Prolonged LOS not only affects patient satisfaction but also increases healthcare costs and limits hospital capacity.18,19 Identifying trends in LOS following hip fracture surgery is essential for evaluating healthcare system performance and optimizing care pathways. By examining changes in LOS over time, healthcare providers and policymakers can pinpoint areas where interventions may be needed to streamline care, enhance patient recovery, and allocate resources more effectively.
To address these critical knowledge gaps, a comprehensive analysis of the American College of Surgeons National Surgical Quality Improvement Program Targeted Hip Fracture (ACS-NSQIP THF) data was conducted. This study aimed to investigate the trends in 30-day readmission and LOS among older adults who underwent surgical fixation for hip fractures between 2016 and 2021. By investigating these outcomes, this study served as a first step in providing valuable insights for healthcare providers, policymakers, and stakeholders, facilitating the implementation of evidence-based initiatives to improve value-based care in hip fracture management. Ultimately, these efforts have the potential to enhance patient outcomes, optimize healthcare resource allocation, and reduce the burden of hip fractures in the aging population.
Methods
Study Design and Data Source
This study was determined to be exempt from institutional review board (IRB) approval. This study employed a retrospective study design utilizing data from the American College of Surgeons National Surgical Quality Improvement Program Targeted Hip Fracture (ACS-NSQIP THF) database. The ACS-NSQIP THF collects comprehensive data on surgical procedures and outcomes from a large number of participating sites and specifically captures patients who underwent surgical fixation for hip fractures. With a rigorous and standardized data collection process, the ACS-NSQIP THF program aims to improve the quality of care and patient outcomes by tracking a range of perioperative variables, including surgical complications, readmission rates, length of hospital stay, and mortality rates.
Patient Selection and Inclusion Criteria
The ACS-NSQIP THF was queried for patients who underwent surgical fixation of hip fractures from January 2016 through December 2021. This period represents the most up-to-date sample available from the NSQIP database. Patients were identified using Current Procedural Terminology (CPT®) codes 27 236, 27 244, and 27 245, which correspond to internal fixation techniques such as intramedullary nailing and open reduction and internal fixation (ORIF) for femoral neck, intertrochanteric, peritrochanteric, and subtrochanteric fractures. While CPT code 27 236 also includes hemiarthroplasty, patients specifically coded with arthroplasty procedure codes (e.g., 27 125 for hemiarthroplasty and 27 130 for total hip arthroplasty) were excluded to minimize heterogeneity. We acknowledge that some hemiarthroplasty cases may still have been captured under 27 236 due to coding variability. CPT code 27 235 (percutaneous skeletal fixation of femoral neck fracture) was not included, as its use is rare in the geriatric population and is more commonly performed in younger patients with nondisplaced fractures, which were outside the scope of this study. To ensure a targeted analysis on the population most susceptible to hip fractures, only patients ≥65 years old were included in the study. Patients who underwent arthroplasty, including hemiarthroplasty (27 125) or total hip arthroplasty (27 130), were excluded from analysis. The study included only those treated with internal fixation techniques such as intramedullary nailing and ORIF, including cases of displaced femoral neck fractures managed with fixation. Exclusion criteria included patients with femoral shaft fractures, isolated acetabular fractures, pathologic fractures or malignancy, or incomplete records. The index dataset included a total of 72 326 patients from an average of 130.7 participating sites annually. After applying exclusion criteria, a total of 64 794 patients were eligible for and included in the cohort analysis.
Study Variables
The following variables were collected for all patients included in the final cohort: sociodemographics, Elixhauser Comorbidity Indices, fracture-related characteristics, clinical and surgical data. In addition, primary diagnoses, secondary diagnoses and primary procedures were recorded.
Outcomes Measures
The primary postoperative outcome measures included incidence of at least one 30-day readmission following surgical fixation for hip fractures and total hospital length of stay (LOS, in days), during the study period. All adverse events and postoperative outcomes were recorded as secondary outcomes.
Statistical Analysis
Statistical analysis was conducted using JMP®, Version 21 (SAS Institute Inc., Cary, NC) using Student t-tests and one-way analyses of variance (ANOVA) for continuous variables, while chi-square tests were applied for categorical variables. Descriptive statistics were reported as mean ± standard deviation and count (percent) for continuous and categorical variables, respectively. To determine significant variability in 30-day readmission and length of stay (LOS) over the study period, LOS was treated as a continuous variable, and linear regression was used to evaluate trends in LOS over time. Additionally, the Cochran-Armitage Trend Test was applied to assess trends in 30-day readmission rates. Furthermore, in handling missing data, a complete case analysis approach was utilized to ensure that only cases with complete information for the variables of interest were included in the analyses. Statistical significance was set a priori at a P value of less than .05.
Results
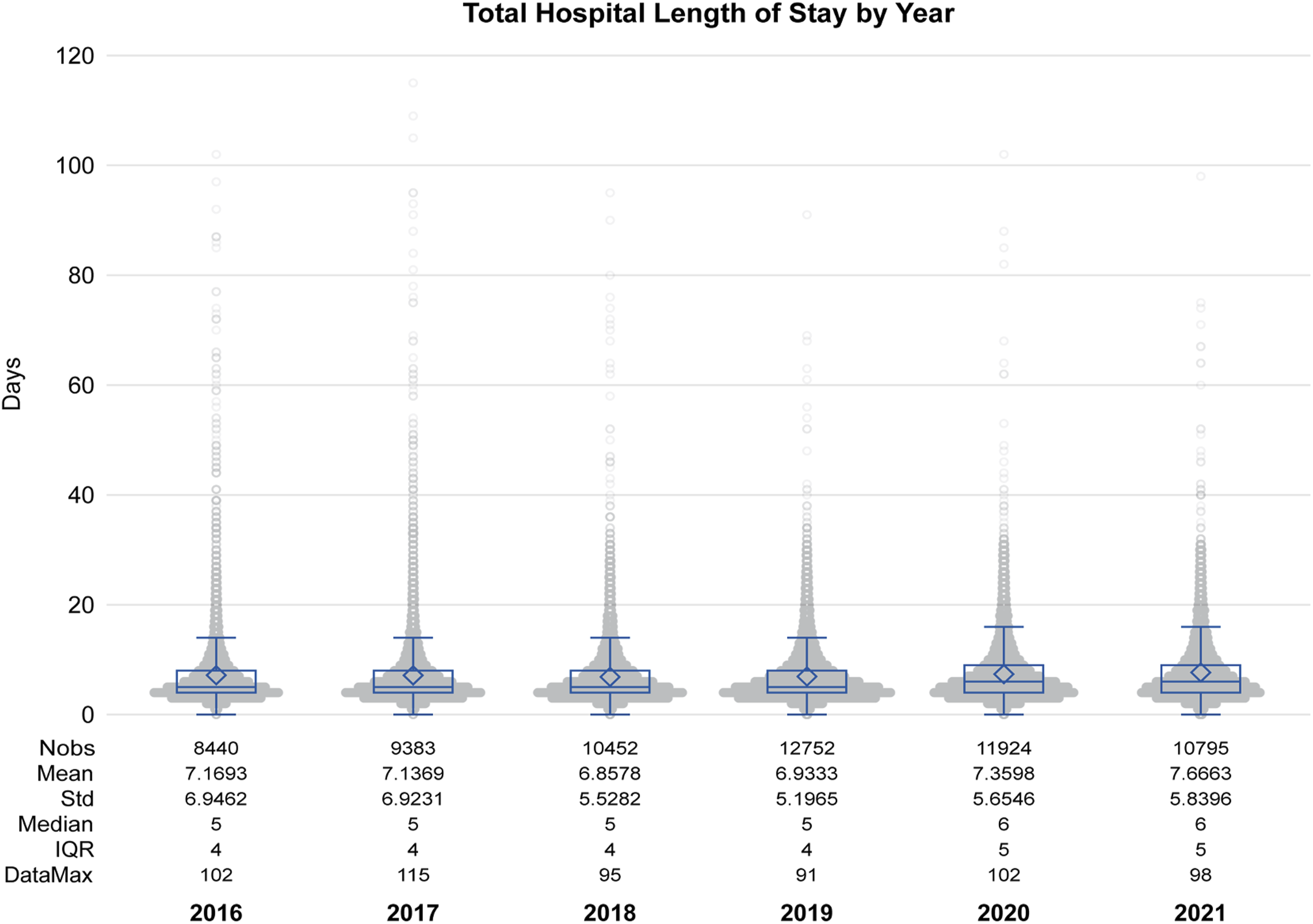
Baseline Patient Sociodemographic, Comorbidity, and Injury Characteristic Data
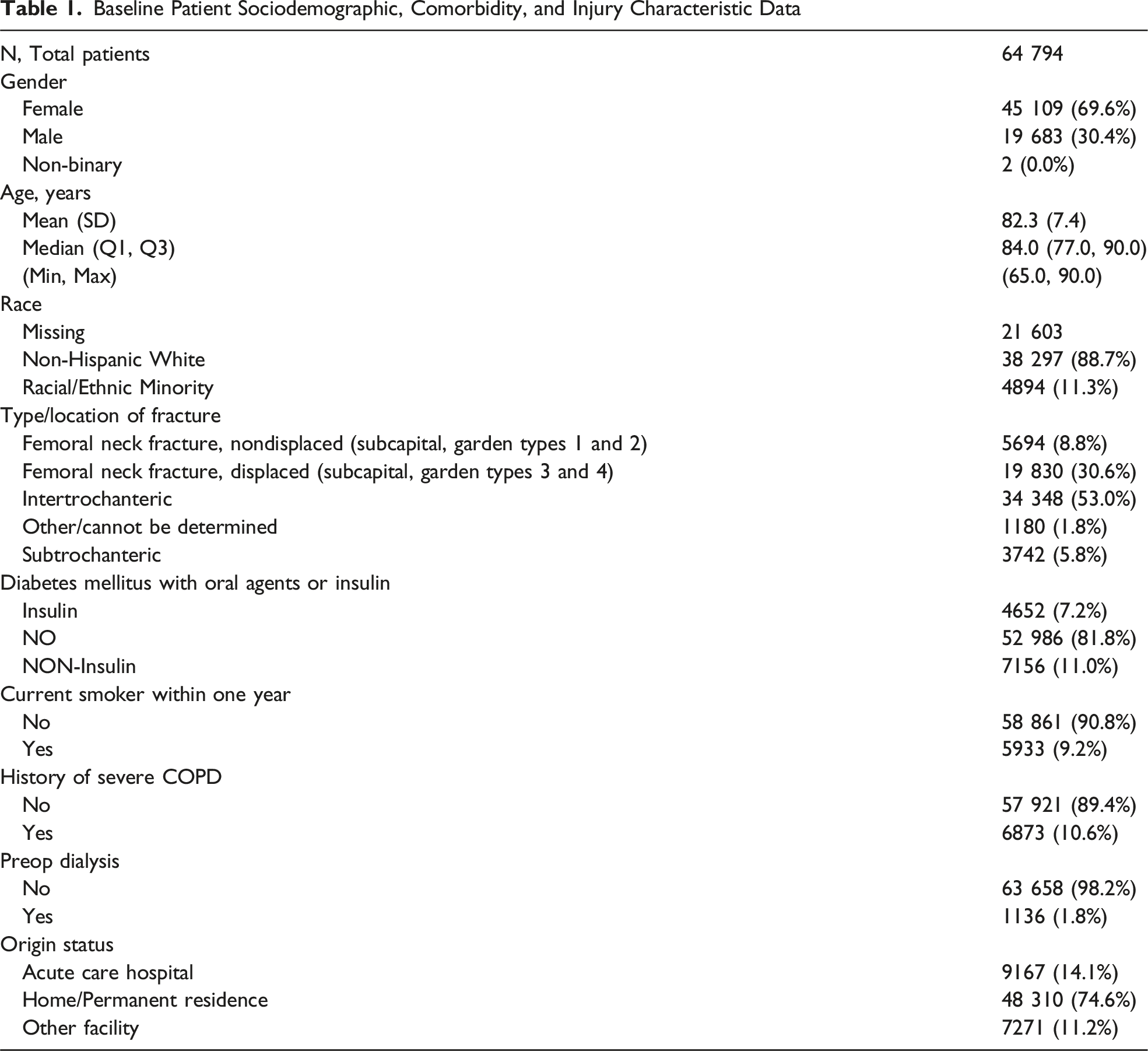
There were no missing data regarding 30-day readmission. After applying eligibility criteria, the final cohort included 64 794 patients, of which 7.85% (95% CI: 7.64% to 8.05%) were readmitted within 30 days of hip fracture surgical fixation. The proportion of patients with ≥1 30-day readmission over time were presented in Figure 1; the Cochran-Armitage Trend Test indicated a statistically significant decreasing trend in the 30-day readmission incidence from 2016-2021 (P < .0001). The mean absolute change in incidence from year-to-year was −0.24% (mean relative change, 0.97) and the total absolute difference in incidence from 2016 to 2021 was −1.20% (relative difference, 0.85). LOS data were missing for 1048 cases (1.62%). Mean and median LOS were consistent across all years (Figure 2). Hip Fracture Readmission Incidence Over Time, ACS-NSQIP Targeted Hip Fracture Patients 2016-2021. Presentation of Annual Incidence of 30-Day Hospital Readmission From 2016 to 2021, With Corresponding 95% Confidence Intervals (Shaded Area). Each Point Represents the Yearly Incidence, Expressed as a Percentage, With Exact Values Annotated Above Each Data Point. The Confidence Intervals for Each Year’s Incidence are provided in Parentheses Below the Respective Points. The Incidence Fluctuated Between 7.0% and 8.6% Over the Six-Year Period. The Note Below Clarifies that Some Cases May Involve Multiple 30-Day Readmissions Hospital Length of Stay Over Time, ACS-NSQIP Targeted Hip Fracture Patients 2016-2021. Illustration of the Distribution of Total Hospital Length of Stay (in Days) for Patients From 2016 to 2021, Represented by Violin-Box Plots for Each Year. The Box Plots Within the Violins Display the Interquartile Range (IQR), Median, and Mean Hospital Stay. The Diamond Shape Marks the Mean Length of Stay for Each Year, while the Whiskers Extend to 1.5 times the IQR. Outliers Beyond This Range are Shown as Individual Points. The Sample Sizes (Nobs), Means, Standard Deviations (Std), Medians, IQRs, and Maximum Data Points for Each Year are Presented Below Each Plot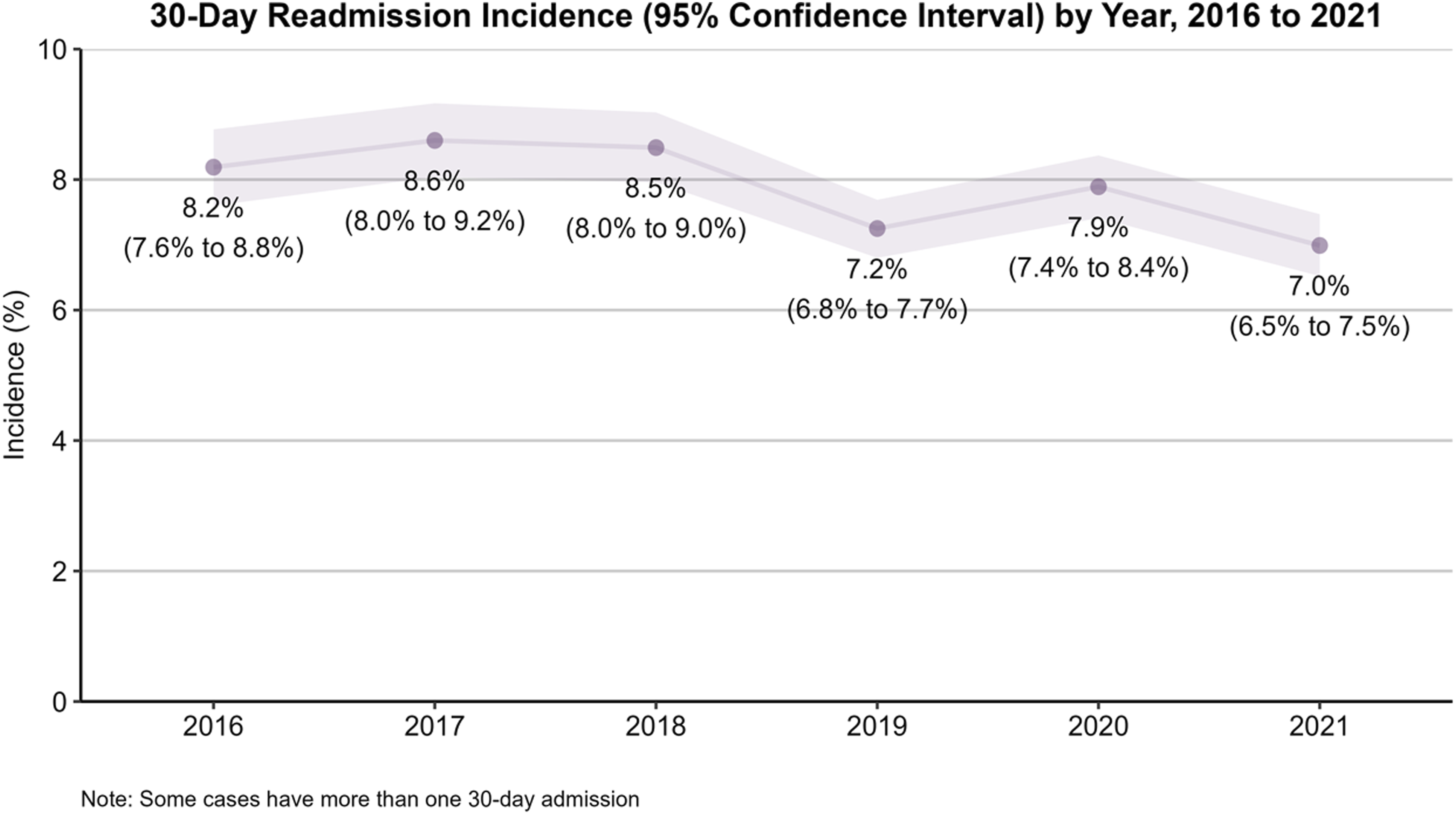
Discussion
This investigation revealed a significant but modest decrement in 30-day readmission rates, amounting to an absolute difference of −1.20% and a relative difference of 0.85 across the years 2016 to 2021. This decline is consistent with broad national trends aiming for healthcare optimization.20-22 Several factors may have contributed to this trend. Non-clinical factors may include the increasing frailty of the hip fracture population over time and disruptions in inpatient and post-acute care related to the COVID-19 pandemic. Additionally, many co-management strategies and other quality improvements may have already been well established by 2016 at high-volume centers performing hip fracture repairs. Clinically, broader healthcare initiatives aimed at improving the quality of care for hip fracture patients likely played a role. Notably, the rise of orthogeriatric co-management programs, which provide a collaborative approach between orthopedic surgeons and geriatricians, has been shown to enhance clinical outcomes by addressing both the surgical and medical aspects of care.10,23 Additionally, the adoption of standardized pain management regimens and early mobilization protocols has become more widespread, with studies demonstrating that these strategies can reduce complications such as pneumonia, deep vein thrombosis, and post-operative delirium, all of which are associated with increased readmission risk.24,25 Despite these improvements, the pace of change remains gradual, as reflected in the relatively stable LOS trends observed in this study, evidenced by the nominal year-to-year change of −0.24% signals a rate of progress that is less than optimal from a macro perspective, given the advent of sophisticated patient management techniques and protocols in recent years. While we did not directly capture these programs and protocols, these persistently elevated readmission rates warrant analysis to identify contributory factors that may hindered more substantive improvements. These likely include, but are not limited to, suboptimal pain management, hospital-acquired infections, and lapses in the transition from in-hospital to home-based care. Recent studies have also indicated that effective pain management can also significantly reduce 30-day readmissions for both hip fractures and general medicine/surgery.26,27
Few studies have utilized national databases to track changes in orthopedic 30-day readmissions, and even fewer have examined these trends over time in hip fracture fixation. In 2019, Ramaswamy et al identified a 0.7% decrease in the 30-day readmission rate for hip fracture patients from 2010 to 2015, supporting the decline in readmissions observed in the present study. 19 Similar trends have been assessed within total knee arthroplasty (TKA) and cervical spinal arthrodesis patient populations, both of which have shown declines in 30-day readmissions after 2010; however, these declines were not statistically significant.20,21
The overall incidence of 30-day readmissions after hip fracture fixation remains heterogeneous. A systematic review conducted by Ali et al reported an average readmission rate ranging from 5.1% to 18.3% for those over 65 years after hip fracture fixation, although most of the studies included in the review reported incidence rates higher than those observed in the present dataset. 22 Only Radcliff et al identified a lower incidence of 7% in 30-day readmissions after hip fracture fixation over a multi-year period. 23 Previous literature indicates a length of stay consistent with the current study.24,25 However, studies conducted on hip fracture outcomes in Sweden and Singapore have reported lengths of stay of 11 and 15 days, respectively.26-28
Implications for Value-Based Care
While direct cost data were not available in the NSQIP dataset, the principles of value-based care—such as minimizing readmissions and optimizing hospital LOS—remain relevant metrics for assessing system efficiency from a top-down approach. Future studies incorporating cost analysis are warranted. For this study, the relatively constant rates in LOS combined with the slight but significant decrease in readmissions offer valuable insights for value-based care models. The data suggest that while efforts to reduce early readmissions have been somewhat successful, there is little effect on reducing LOS, a key metric that correlates with healthcare resource utilization. As value-based care models gain traction, these findings can serve as a reference for stakeholders looking to improve care quality and cost-effectiveness in the management of hip fractures. The principles of value-based care dictate a shift from quantity-driven models to those that prioritize patient-centric, high-quality outcomes. However, the present data indicates that the pace of alignment with these principles, at least in the context of 30-day readmission rates for hip fracture surgeries in elderly patients, is sluggish. Enhanced care pathways that incorporate orthogeriatric co-management, better pain control, and comprehensive postoperative rehabilitation are prime candidates for accelerating improvements.
In recent years, DRG (Diagnosis-Related Group) codes 480, 481, and 482, which are commonly utilized for hip fracture cases, are increasingly being shifted towards bundled payment arrangements as a part of value-based care strategies.28,29 This is despite concerns that hip and femur fracture surgeries may not lend themselves to the type of predictable episode of care events noted in hip and knee arthroplasty surgery. 30 These bundled care models often aggregate various costs associated with an episode of care into a single payment. The transition to value-based care prioritizes both efficiency and efficacy, often requiring a coordinated effort among multiple stakeholders, including clinicians, policy makers, and healthcare administrators.30-32 Multi-disciplinary approaches have shown promise in reducing readmission rates in other surgical fields and should be considered in orthopaedic trauma settings.33,34 Tailoring such programs to include not only clinical outcomes but also equity-conscious parameters can make a substantial difference. However, given the present findings, the persistent length of stay and readmission rates should be parameters included when defining the benchmarks for these bundled care episode contracts. The lack of significant change in these metrics over the study period suggests that bundled payments should be designed cautiously to ensure that the quality of care does not decline in the pursuit of reducing cost.
Limitations
This study had several limitations inherent to using large national databases like NSQIP. An important limitation of the study was that it did not account for potential regional disparities in readmission rates and LOS. Factors such as hospital capacity, local healthcare policies, and geographical variations in healthcare access could influence these metrics and should be considered in future research. The NSQIP database restricted the ability to incorporate granular socio-demographic factors, such as the area deprivation index, which have been shown to impact readmission rates. This granularity is essential for tailoring interventions that are sensitive to the disparities in healthcare outcomes.
Regional variations may hold nuanced implications for value-based care efforts, and understanding these could be crucial for policymakers aiming to implement more tailored and effective programs. 35 Incorporating regional trends into future investigations would not only enrich the dataset but also provide a more contextualized understanding, thereby guiding policy recommendations and hospital practices to be more region-specific. The inclusion of regional analyses can also shed light on social determinants of health that are locally relevant, thereby informing the design of more equity-conscious, value-based care paradigms. These findings generate several avenues for future research, particularly in elucidating the underlying factors contributing to the slow but steady decrease in readmissions. Investigations into surgical techniques, postoperative care protocols, and healthcare policy changes during the study period can offer insights. Moreover, future studies should seek to integrate more comprehensive socio-demographic data to provide a nuanced understanding of factors affecting readmissions and LOS. In addition, the authors recognize that total hip arthroplasty (THA) is increasingly utilized in the treatment of displaced femoral neck fractures, particularly in functionally independent patients. However, this study focused exclusively on fixation-based interventions to maintain cohort homogeneity and to better isolate trends in readmission and LOS specific to internal fixation techniques. While this approach improves internal validity, it limits the generalizability of our findings to patients managed operatively with arthroplasty. Future studies should evaluate outcome trends across the full spectrum of surgical treatments, including arthroplasty, to provide a more comprehensive understanding of national hip fracture care. In addition, an important limitation of this study relates to the use of CPT code 27 236. Although this code was intended to capture internal fixation cases, it also can include hemiarthroplasty, and many surgeons preferentially use this code instead of 27 125. While patients with explicit arthroplasty codes (27 125, 27 130) were excluded, it is possible that some hemiarthroplasty cases remained within our cohort, introducing heterogeneity. Additionally, CPT 27235, which describes percutaneous skeletal fixation of femoral neck fractures, was not included. This code is infrequently used in geriatric populations and is more commonly applied to younger patients with nondisplaced fractures, which was outside the scope of our analysis. Nonetheless, the exclusion of 27 235 may limit the generalizability of our findings to this less common treatment group. Finally, only 30-day readmission data are available within the NSQIP Targeted Hip Fracture Dataset. As such, longer-term outcomes, including 90-day readmission, could not be assessed and warrant further investigation with large database models.
Conclusions
The present study highlights a significant but insufficient decrease in 30-day readmission rates and a static pattern in LOS for older patients undergoing hip fracture surgery. This duality calls for a nuanced approach in strategizing value-based care interventions, requiring both healthcare providers and policy makers to evaluate and redesign care pathways that not only aim for clinical efficacy but also incorporate equity-conscious parameters. The efforts of the present study aim to catalyze targeted, value-based improvements in managing hip fracture patients, prioritizing both clinical and equity parameters in future healthcare policies and interventions.
Footnotes
Author Contributions
Jack Twomey-Kozak, MD -- conceptualization, study design, data analysis, and manuscript drafting.
John Lewis Atwater, MD -- conceptualization, study design, data analysis, and manuscript drafting.
Kenneth Adam Taylor, PhD -- statistical analysis, data interpretation, manuscript revisions, figure/table preparation.
Malcolm DeBaun, MD – supervision, study design, interpretation of findings and critical revision of the manuscript.
Christian Alexander Pean, MD, MS – study oversight, study design conception, manuscript writing and revisions.
*All authors reviewed and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data utilized in this study were obtained from the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) and are publicly available; though access is limited to participating institutions through data use agreements.