
Abstract
Purpose:
To compare and contrast postoperative complications in the geriatric population following open reduction and internal fixation (ORIF) for (DF) fractures relative to femoral neck (FN) fractures.
Methods:
Patients aged 65 years and older in the American College of Surgeons National Surgical Quality Improvement Program database who underwent ORIF for FN fractures or DF fractures from 2005 to 2012 were identified. Differences in rates of any adverse events (AAEs), serious adverse events (SAEs), infectious complications, and mortality between groups were explored using univariate and multivariate analyses.
Results:
The DF cohort had a higher proportion of females (81.95% vs 71.35%, P < .001), were younger (79.41 ± 7.93 vs 82.11 ± 7.26 years old, P < .001), and had a lower age adjusted modified Charlson comorbidity index score (4.22 ± 1.32 vs 4.49 ± 1.35, P = .02). Cases with DF and FN did not differ in AAE (20.05% vs 20.20%, P = .94), SAE (12.03% vs 13.19%, P = .51), infectious complication (4.26% vs 4.22%, P = .97), hospital length of stay (7.32 ± 6.73 days vs 7.02 ± 10.67 days, P = .59), or mortality rates (4.51% vs 5.99%, P = .23). Multivariate analyses revealed that fracture type did not impact AAE (P = .28), SAE (P = .58), infectious complications (P = .83), or mortality (P = .85) rates.
Conclusion:
Postoperative morbidity and mortality of geriatric patients who sustain DF and FN fractures treated operatively were comparable. This information can be used when risk stratifying and prognosticating for elderly patients undergoing these procedures.
Introduction
Hip fractures in the geriatric population are readily recognized to have high perioperative morbidity and mortality. 1 –3 In addition to being debilitating and potentially fatal injuries, hip fractures also incur a tremendous economic cost with projections of direct medical costs expected to reach US$446.3 billion by 2050. 4,5 Distal femur (DF) fractures are also severe lower extremity injuries that present several challenges to orthopedic surgeons with regard to implant choice and postoperative management decisions. 6 –8 However, outcomes of operatively treated DF fractures in the elderly are underreported in the literature. 9,10 As the population continues to age and incidence of these fractures is expected to increase, 11 an understanding of the risks associated with surgical interventions for the elderly is critical.
The American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) is a multi-institutional outcomes database that presents a unique opportunity to better elucidate factors contributing to adverse events in the perioperative period. Numerous studies have utilized NSQIP in the surgical literature, with increasing use in the field of orthopedic surgery. 12,13 Studies directly comparing early outcomes of operative managed DF and femoral neck (FN) fractures in the elderly patients are lacking, and none have utilized a database such as NSQIP for analysis of short-term outcomes for these fractures. This study sought to compare and contrast preoperative characteristics, rates of mortality, adverse events, and postoperative length of stay in geriatric patients sustaining DF and FN fractures. Our null hypothesis was that there would be no differences between the 2 injury cohorts.
Materials and Methods
The ACS-NSQIP database consists of prospective data on a defined set of patient demographics, medical history, and adverse events collected across numerous hospital sites. Throughout data collection, measures such as site visits and system auditing of institutional records are implemented to ensure integrity and validity of data. 14,15 This study was institutional review board exempt.
The NSQIP database was queried initially for DF fractures using International Classification of Diseases, 9th Revision (ICD-9) codes 821.20-821.39. Patients with DF fractures were then cross referenced to primary Current Procedural Terminology (CPT) codes 27509, 27511, 27513, and 27514. Femoral neck fractures were similarly queried in the database by ICD-9 codes 820.00 to 820.19, and cross-referenced to CPT codes 27130, 27235, and 27236. This was done to ensure accurate characterization of the injury types and operative procedures being investigated. Only patients aged 65 and older who underwent either a FN or a DF fracture repair between 2005 and 2012 were included.
A comorbidity score was calculated with a modified Charlson comorbidity index (CCI) calculated to fit available data as described previously by Bohl et al. 16 Patient groups were compared in terms of demographic factors including age, sex, functional status prior to injury, modified CCI, body mass index (BMI) and American Society of Anesthesiologists (ASA) status. In addition to patient demographics, total hospital length of stay and operative time were compared between groups. Differences between groups were explored using Pearson chi-square tests for categorical variables and independent t tests for continuous variables.
Postoperative complications were recorded and coded to be any adverse event (AAE), serious adverse event (SAE), infectious event, or mortality. The SAE was defined as any of the following: death, a coma for more than 24 hours, ventilator for more than 48 hours, unplanned intubation, stroke/cerebrovascular accident, pulmonary embolism, cardiac arrest, myocardial infarction, acute renal failure, sepsis, septic shock, or return to the operating room. An infectious complication was defined as superficial surgical site infection, deep surgical site infection, organ/space infection, sepsis, or septic shock. These were incorporated as a unique category for analysis but also included in the SAE and AAE categories. The AAE category included all SAEs and infectious complications as well as deep vein thrombosis, failure to wean from ventilator, renal insufficiency (rise in creatinine by >2 mg/dL above baseline), urinary tract infection, peripheral nerve injury, graft/implant failure, and reoperation within 30 days. This categorization of adverse events and infectious complications was consistent with methods used in similar previous studies utilizing the NSQIP database. 12
Pearson chi-square tests and Fisher exact test were used to assess differences between groups for complication rates. Multivariate logistic regression analyses to identify independent predictors of AAEs, SAEs, infectious complications, and mortality rates were carried out. P < .05 was considered significant for all tests. Statistical analysis was conducted using SPSS (SPSS, Chicago, Illinois).
Results
A total of 4236 patients (3837 FN cases and 399 DF) met the inclusion criteria. The DF cohort patients consisted of more females (81.95% vs 71.35%, P < .001), were younger (79.41 ± 7.93 vs 82.11 ± 7.26, P < .001), had a lower age-adjusted modified CCI score (4.22 ± 1.32 vs 4.49 ± 1.35, P = .02), a higher BMI (27.14 ± 12.16 vs 22.07 ± 9.82, P < .001), and a higher proportion of diabetic patients relative to patients with FN (26.07% vs 16.13%, P < .001). There were no differences between DF and FN groups with regard to smoking history (8.73% vs 10.28%, P = .30), proportion of patients with ASA < 3 (18.88% vs 18.55%, P = .87), or dependent functional status (30.79% vs 32.99%, P = .37). Comprehensive information on patient characteristics is included in Table 1.
Patient Characteristics.

Abbreviations: BMI, body mass index; CCI, Charleston comorbidity index; ASA, American Society of Anesthesiologists; LOS, length of stay; COPD, chronic obstructive pulmonary disease.
There was no significant difference between cases with DF and FN in rates of AAE (20.05% vs 20.20%, P = .94), SAE (12.03% vs 13.19%, P = .51), infectious complication (4.26% vs 4.22%, P = .97), or mortality rates (4.51% vs 5.99%, P = .23; Table 2). There was no difference in hospital length of stay between the 2 groups (7.32 ± 6.73 days vs 7.02 ± 10.67 days, P = .59).
Thirty-Day Postoperative Complications in Distal Femur Versus Femoral Neck Fracture Repair.a
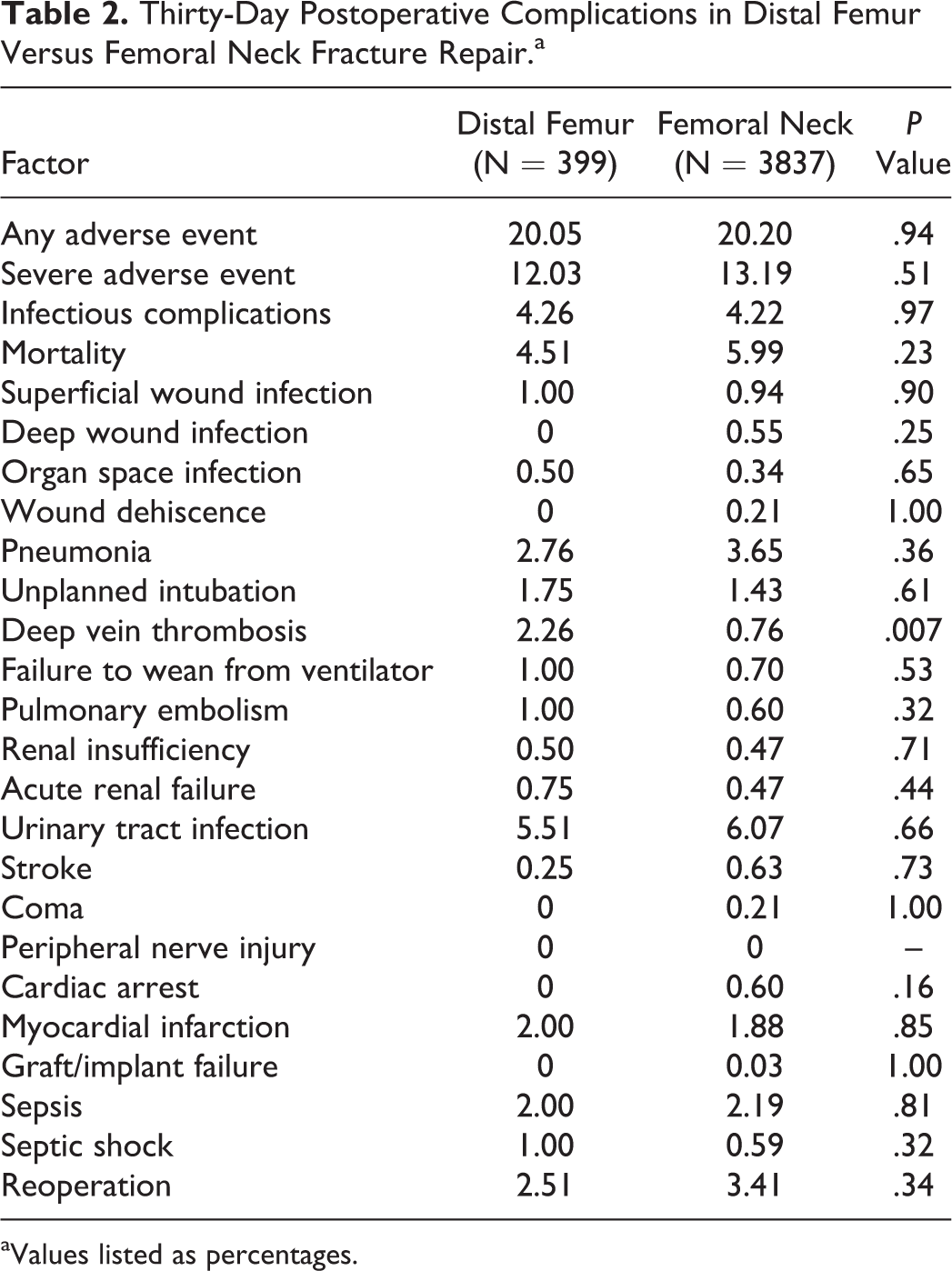
aValues listed as percentages.
Multivariate analyses revealed that fracture type did not impact AAE (P = .99), SAE (P = .58), infectious complications (P = .83), or mortality rates (P = .85). Predictors of AAE included ASA 3 or 4, older age, higher CCI, dependent functional status, male gender, emergency operation (assigned if the case is deemed “emergent” by the attending surgeon, indicated for surgery as soon as possible, and performed no later than 12 hours after the patient has been admitted to the hospital), and longer operation time (Table 3). Predictors of any SAE included older age, ASA 3 or 4, dependent functional status, emergency operation, higher CCI, open wound/wound infection prior to surgery, hypertension, dyspnea, longer operation time, and male gender. Predictors of any infectious events included ASA 3 or 4, dependent functional status, and longer operation time. Multivariate analysis also revealed that predictors of mortality included older age, ASA of 3 or 4, higher CCI score, dependent functional status, emergency operation, and male gender.
Multivariate Analysis of Risk Factors for Any Adverse Event, Severe Adverse Event, Infectious Event, and Mortality.

Abbreviations: CCI, Charlson comorbidity index; ASA, American Society of Anesthesiologists; CI, confidence interval.
aModified CCI score was included as a continuous variable in the logistic regression model, thus the odds ratio should be interpreted as increased odds of an adverse event occurring associated with a 1 unit increase in modified CCI.
Discussion
In this study, we found that patients who sustain a distal femoral fracture share a similar adverse event profile with those patients who sustain a FN fracture. Femoral neck fractures are a well-studied group of patients whose outcomes are of extreme importance to the health care system, given the numbers and costs associated with their care. The characterization of risk factors for complications in DF and FN fractures in geriatric patients is increasingly important for orthopedic trauma surgeons. Operatively managed DF fractures were seen to have very high rates of overall adverse events in this study on par with those seen in FN fractures.
There are several studies available for comparison to substantiate this study’s findings regarding adverse event rates for these fractures. Streubel et al in a prospective cohort of 92 patients older than 60 years with DF fractures observed a mortality rate of 6% in the 30-day postoperative period. This is comparable to the present study’s observed mortality rate of 4.5% in patients with DF. 9
A modified frailty index put forth by Patel et al in 2013 compiled numerous clinical deficits into a single score that was found to correlate with mortality in FN fractures. 17 Interestingly, in our study, dependent functional status was seen to independently predict mortality in a multivariate analysis of this overall cohort. Dependent functional status in the NSQIP database corresponds to an overview of the activities of daily living the individual patient in the database is capable of performing. 18 This is most analogous to the patient characteristic of ambulatory status used in the modified frailty index. This lone variable may potentially be used in conjunction with other variables in NSQIP to create a more sophisticated validated risk stratification schema for patients with these injuries.
A study by Prestmo et al found comprehensive geriatric care for patients with hip fractures led to improved mobility and functional outcomes. 19 The poor outcomes found among geriatric patients with DF fractures in this study suggest a similar approach warrants consideration for these injuries. These findings are consistent with those noted in a study by Rocca et al, which indicated that geriatric patients with lower extremity fractures below the hip were similar to those with hip fractures in terms of medical comorbidities. 20 We similarly conclude that based on these findings, implementing comprehensive care models for geriatric patients with DF fracture, as those detailed for hip fractures may result in similar improved outcomes.
A notable difference between patient cohort demographics in this study was the substantially higher BMI observed in patients with DF fracture versus FN fracture. Obese individuals have been known to have an increased hip bone mineral density and more robust femur geometry. An observational study by Beck et al found fracture incidence at the hip was lower with increasing BMI. 21 It is possible that increased soft tissue padding with greater BMI is reflected in the patient demographics of this study with more obese geriatric patients less likely to have hip fractures. This protective factor may be diminished at the DF where less soft tissue padding is apparent. Despite a higher BMI, DF fractures did not differ from FN fractures in proportion of patients with dependent status or in overall adverse outcomes suggesting these patients remain high risk in the postoperative setting.
Factors independently associated with overall adverse outcomes in multivariate analysis included increased ASA status, hypertension, age, CCI, and operation time. These have been demonstrated to negatively impact orthopedic postoperative outcomes in previous NSQIP studies and are likely not specific for these fracture types. 13 Of note, male gender was found to be independently associated with incidence of SAE and mortality (Table 3). Both cohorts were overwhelming female, and it is unclear why male sex would predispose patients to mortality, although male sex has been seen to increase 1-year mortality for hip fractures. 22
This study was limited by several characteristics of the ACS NSQIP database including the availability of only short-term outcomes and a lack of data on perioperative characteristics relevant to orthopedic surgery. There is no information on patient satisfaction, detailed fracture pattern, pain, or postoperative weight-bearing status available. 15 Although the NSQIP database is a national data sample with detailed outcomes documented for patients included, the stringent inclusion criteria, and recent increasing use in orthopedics result in smaller sample sizes than those found in other national databases. 17,23 Furthermore, energy of mechanism of injury is unavailable in ACS NSQIP, a factor that may have helped parse out risk factors for adverse outcomes in this study. 24
Smoking and obesity were not found to impact rates of complications in this study. These findings may ease surgeon concerns for increased postoperative complications in these patients to some extent. Still previous studies finding an increased risk of infection for patients with these characteristics including those sustaining DF fractures treated with locking plates should not be discounted. 25 It has also been reported that obesity may impact long-term functional outcomes and union rates in DF fractures, a finding particularly relevant given the overall above average BMI for patients with DF fracture in this cohort. 26
This is the first study we are aware of to directly compare postoperative complications of DF and FN fractures treated operatively in the geriatric population on this scale. Despite limitations, the NSQIP database is a multicenter, nationwide database that presents a more representative sample of US surgical practice patterns than other databases. Although patient characteristics of geriatric patients with operatively treated DF and FN fractures are not entirely similar, the postoperative morbidity and mortality are comparable. These findings suggest the potential comanagement of these patients in similar comprehensive care institutions should be explored further. This information can also be taken into consideration when risk stratifying elderly patients with these injuries and can inform the physician–patient–family discussion with regard to prognosis and expected hospital course.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.