
Abstract
Introduction
Total hip arthroplasty (THA) performed for femoral neck fractures (FNFs) is becoming a more frequent treatment in the active elderly population. Since there is limited research available presenting clinical outcomes after THA using the anterior-based muscle sparing (ABMS) approach, the aim of this study was to compare this surgical approach to the direct lateral (DL) approach in patients treated by THA for FNFs.
Materials and Methods
We retrospectively reviewed the data prospectively collected as a part of our “Hip Fracture Unit” and included 163 patients who underwent THA from January 2016 to January 2019 for acute displaced FNFs.
Results
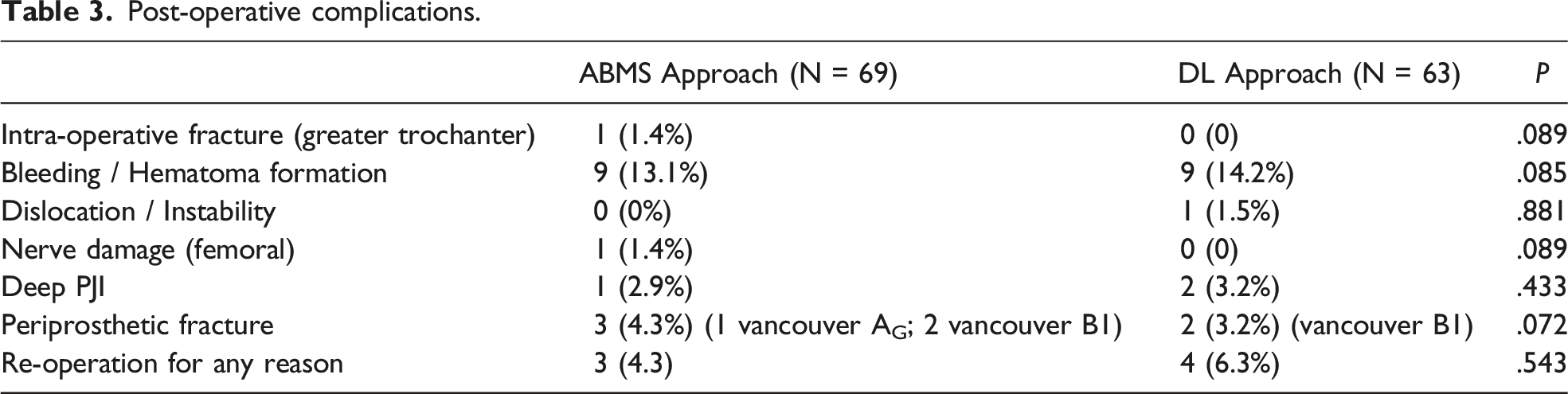
A total of 132 patients who completed a minimum 2-years follow up (69 in the ABMS group and 63 in DL group) were included. The ABMS group demonstrated significantly shorter time to reach milestone for hospital discharge (1.5 Days vs 2.1 days, P = .018), while no statistically significant differences were detected in peri-operative complications. At 3 months, the timed up and go test, the Harris Hip Score (HHS) and the Oxford ip Score (OHS) were significantly better (P = .024, .032 and .034, respectively) in the ABMS group compared to the DL group. No differences were found in functional outcomes (HHS and OHS) nor in complication rate at 6, 12 and 24 months.
Discussion
This is one of the first studies to analyze functional results of THA performed for FNFs through an ABMS approach. Results are in line with those already present in the Literature.
Conclusion
ABMS approach allows earlier mobilization and better early functional outcomes, compared to DL approach, in patients undergoing THA for acute displaced FNF. No differences are found after 6 months in functional results and complications rate.
Keywords
Introduction
Surgical management of femoral neck fractures (FNFs) with total hip arthroplasty (THA) is becoming more popular in the active elderly population compared to internal fixation or hip hemiarthroplasty (HHA).1-3 The reasons for the increased use of THA are thought to be related to the improvement of patients’ satisfaction and quality of life, and possible economic advantages compared to alternative options. 4 Nevertheless, complications and related failures are still frequent, and multiple studies have demonstrated a higher incidence of complications, hospital readmissions and re-operations following THA for FNFs compared to THA for osteoarthritis (OA).5,6 Many factors have been demonstrated to influence the frequency and nature of these complications. Among modifiable factors, the choice of surgical approach is one of the most relevant.4,7
Historically, the two most used approaches for THA after FNFs are the postero-lateral (PL) approach described by Moore 8 and the direct lateral (DL) approach described by Hardinge. 9 In recent years, there has been growing interest in tissue-sparing approaches. The soft-tissue-preserving nature of the direct anterior (DA) approach, which uses the interval between sartorius and tensor fasciae latae (TFL) muscles, has generated a great interest even in the treatment of femoral neck fracture. 10 The rationale of its use in FNFs are the reduced risk of dislocation, decreased postoperative pain and faster rehabilitation which may be particularly favorable in an old and frail patient population, and it has been reported to have improved early rehabilitation when compared with alternate approaches.11,12
However, there is another anterior approach to the hip which is less popular than the DA approach: the anterior-based muscle sparing (ABMS) approach 13 or, as also named in the literature, antero-lateral minimal invasive (ALMI) approach, or similar. 14
This approach is based on a modification of the standard antero-lateral Watson-Jones interval, 15 and the dissection of the hip is performed using the intermuscular plane between the TFL and the gluteus medius (GMe) without any detachment of the abductor muscles. The ABMS approach is anterior to the GMe and to the greater trochanter, and thus, it is similar and shares the advantage of the DA approach of being a muscle sparing approach. 15 The results of the ABMS approach used in THA for OA has been widely described in literature,16,17 but there is a paucity of report about the use of the ABMS approach in THA performed for FNFs.
The purpose of the study was to find evidence whether there are advantages of using an ABMS approach compared to a conventional DL approach to perform THA for the treatment of FNFs in the elderly active population.
Materials and Methods
Participants
We retrospectively reviewed the data prospectively collected as a part of the “Hip Fracture Unit” project that prospectively documents the treatment and outcomes of all patients with a fragility hip fracture admitted to our “Hip Fracture Unit”, that annually treats more than 600 patients with proximal femur fracture and is a multidisciplinary project designed to improve the care for these patients at our hospital.18-20
All patients who had undergone THA for acute displaced FNFs (Garden type III and IV) between January 2016 and January 2019 were considered for inclusion in this study. The other inclusion criterium was the use of either the ABMS or the DL approach to perform the procedure. We excluded patients with bilateral fractures, pathological fractures, previous ipsilateral hip or femoral surgery, patients unable to walk before the fracture occurred, and patients with medical contraindications, medical illness or cognitive disorders precluding participation to follow-up examinations and unwillingness to participate.
Following the inclusion and exclusion criteria, 163 patients with FNFs operated on from January 2016 to January 2019 were included into the study. According to the surgical approach used, the patients were divided into 2 groups. Eighty-four patients were operated on through the ABMS approach, while 79 patients through the DL approach. Institutional Review Board approval was obtained prior to initiation of the hip fracture project and the study has been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. All patients had provided informed consent to the treatment plan, the operation plan, and the rehabilitation and follow-up process. Also, all patients gave their informed consent to data collection and their anonymous use for scientific purposes.
Surgical Treatment and Peri-Operative Care
All surgical procedures were performed with the patient in supine position and both legs draped into the surgical field to assess rotation and leg-length intra-operatively. Intravenous antibiotic prophylaxis was administered following our hospital protocol for orthopedic prosthetic procedure (Cefazolin 2 g + Vancomycin 15 mg/kg pre-operatively and every 8 and 12 hours post-operatively for 48 hours, respectively).
In the ABMS approach, as previously described, 13 the interval plane between TFL and GMe was used, without any detachment of the abductor muscles. In the DL approach, the GMe was incised along the fiber course to a maximum length of 3 cm to protect the inferior branch of the superior gluteal nerve. The anterior third of the GMe was detached together with the underlying gluteus minimus ventrally to expose the joint capsule. Lengthening of the incision into the vastus lateralis was strictly avoided.
Implants used were both cemented and press-fit. In every patient, an uncemented cup was implanted (Regenerex Ringlock Acetabular system or G7 acetabular system, Zimmer Biomet Orthopedics Inc, Warsaw, IN, USA; and Dynasty system, Microport Orthopedics Inc, Arlington, TN, USA) while the stem was cemented (Profemur Gladiator Cemented Modular Stem, Microport Orthopedics Inc) or press-fit (Taperloc Complete Hip System, Zimmer Biomet Orthopedics Inc). Choice of the femoral stem (cemented/press-fit) was based on age of patients and the canal-fill ratio. In all cases, a highly cross-linked polyethylene liner (both neutral or high-wall) was adopted and was coupled with a ceramic or Cobalt-Chromium head, 32 or 36 mm in diameter, from same manufacturers, depending on the size of the cup.
After the surgical procedure, all patients were hospitalized in our multidisciplinary ortho-geriatric unit, where they underwent the same post-operative protocol regardless of the surgical approach used. Twelve hours after surgery, patients were placed in the sitting position, and 24 hours after surgery they were verticalized and mobilized with full weight bearing under physiotherapeutic (PT) assistance. Peri-operative antithromboembolic prophylaxis with low molecular weight heparin was admistered to all patients. In patients already under oral anticoagulants prior to surgery, the drug was discontinued at admission and reintroduced 36-48 hours after surgery.
Clinical Assessment: Primary and Secondary Outcomes
During post-operative hospitalization, days to reach PT milestones for hospital discharge was registered. At our Institution, to meet PT discharge criteria patients must be able to: (1) transfer in and out of bed and chair independently, (2) independently (even if with crutches or an axillary walker) ambulate approximately 50 meters, and (3) ascend and descend at least 4 steps of stairs.
At the 3-months follow up outpatient visit, the “timed up and go” (TUG) test was registered. This test was introduced in 1991 as a modification of the “get-up and go” test, 21 and it is a simple, easy, and thus widespread clinical tool for measuring the lower limbs’ functionality and mobility of patients. Also, the Harris Hip Score (HHS) and the Oxford Hip Score (OHS) were assessed at 3, 6, 12 and 24 months after surgery. The HHS is a clinician-based outcome measure, while the OHS is a short 12-item patient-reported outcome measure; the cross-culturally adapted and validated Italian versions of both scores were used.22,23
Secondary outcomes were surgical and peri-operative complication rate, and re-operation rate. Surgical and peri-operative complication rates were recorded accordingly to the adverse events standardized list, developed by the American Hip Society, including post-operative bleeding/haematoma formation, implant failure, implant dislocation, periprosthetic fractures, superficial wound infection, deep periprosthetic joint infection (PJI), nerve damage, and more. 24 Re-operation rate was recorded as need for re-intervention for any reason at last follow up.
Statistical Analysis
Statistical analysis was performed using the Chi-square test or Fisher’s exact test to compare categorical variables between groups, while the Student’s t test or Mann-Whitney U test were used to compare continuous variables. The significance level was set at P < .05; p was reported as not significant (n.s.) in text and with exact values in Tables. All data were elaborated with SPSS® statistics software (IBM®, Armonk, New York, NY, USA).
Results
Comparison of Demographic and General Clinical Characteristics for Each Group of Patients.

Primary Outcomes
Main functional outcomes.

Results presented as mean (range); statistically significant results in
Secondary Outcomes
Post-operative complications.
Discussion
THA is the preferred treatment for displaced FNFs in active, cognitively intact, and independently mobile patients. However, complications and related failures are still frequent and include: dislocation, periprosthetic fractures, PJIs, nerve damage, aseptic loosening, and others; the choice of the surgical approach is crucial to influence the nature and frequency of these complications. 4 Two conventional approaches for arthroplasty after FNFs have been described since the 20th century with only slight modifications over time, the PL and DL approach; they have been extensively studied in the literature and advantages and disadvantages have been clarified. 26 The DL approach allows for an excellent exposure of both the femur and the acetabulum but requires partial release of the anterior third of the GMe; therefore, the functional outcome could be complicated by a disfunction of the abductor muscles that may lead to limp-walking or Trendelenburg gait and pain at the level of the greater trochanter. THA for FNFs performed through a PL approach result in less pain, with better patient satisfaction and better quality of life. 7 However, PL approach has an increased risk of dislocation and reoperation due to instability. As a consequence of that, the DL approach is associated with a lower risk for revision than the PL approach, regardless of the cause. 27
With the effort of combining the advantages of the 2 approaches, in the recent years, newer approaches have been utilized in THA for FNFs, and mainly the DA approach. Nowadays, it is estimated that about 10% of the hip surgeons use this approach as the standard approach for THA after FNF, 4 and results has already been extensively reported in literature. In the first systematic review and meta-analysis of the DA approach for FNFs, 10 9 eligible studies published between 2012 and 2016 were included in the study. Data demonstrated that DA approach provided superior early functional mobility compared to other surgical approaches in 4 studies, and no other study favored another approach over the DA. Subgroup analysis demonstrated significantly fewer dislocations among DA (1.1%) vs PL approach (7.8%). No other significant differences between the DA and other approaches regarding the overall complications, perioperative fractures, infections, re-operation rates, and mortality were found. Other studies have shown similar results. Bucs et al carried out a study to evaluate the efficacy of the DA approach in HHA for FNFs compared to the DL approach. In their study, patients operated through the DA approach showed significantly less post-operative pain, allowing them to an earlier mobilization. 28 Nogler et al demonstrate that patients treated with anterior approaches had less post-operative pain, less blood loss, and reduced hospital stay than those treated with PL or DL approaches. 29
More recently, other Authors reported similar excellent clinical results and a low rate of complications.11,12 From these results one may argue that the DA should be the approach of choice in arthroplasties (both THA and HHA) for FNFs. However, it has to be considered these are selected studies that are exposed to bias in patients’ selection, surgeon’s skill and experience. Studies on patients with OA indicated that an anterior approach is technically more demanding, with more complications and a steep learning curve with respect to PL or DL approaches. 30 From these considerations, the ABMS approach could combine the advantages of a DA approach without the drawback of such a more demanding approach. It has been clearly demonstrated that the ABMS approach shares the advantages of the DA of being muscle sparing by not violating the abductor muscles. The ABMS approach has been typically performed with the patient in the lateral decubitus or in the supine position with the use of a fracture table or any other dedicated table, but it can be easily performed in a supine position on a standard table, is both lower limbs are prepped. Moreover, compared to the DA, the ABMS approach has no limitations in femoral component design, and it has a shorter learning curve. 13 Despite these considerations that create a strong rationale for its use in THA for acute FNFs, there are just few reports in the literature about the results of ABMS approach in such a pathology. De Jong et al found that the AMLI (or ABMS) was a safe alternative to the traditional AL approach with improved operation time, smaller incision and less surrounding tissue damage. 31 Similar results were reported by Tsailas et al when comparing the outcomes of the ALMI approach to traditional PL approach for the management of FNFs in the elderly. They found limited complication rate, similar to that observed with the PL, strongly suggesting that ALMI is a safe and valid technique for elderly patients with FNFs requiring joint replacement (THA or HHA). 32
To our knowledge, the present study is one of the first in which results of the ABMS approach in THA for FNFs have been analyzed in detail. The principal finding of this study is that the ABMS approach presents better clinical results in terms of immediate and early functional outcomes as well as better patient-reported outcomes, in comparison with the DL approach, but just within the first 3 months after surgery. Actually, the AMBS group recovered faster during hospitalization and reached earlier the PT milestones for hospital discharge, suggesting that the muscle-sparing nature of this approach is potentially beneficial for both in-hospital mobility and early return to the activities of daily living. In our opinion, the statistical significance of both earlier hospital discharge and 3 months TUG test can play a critical role for this specific population of elderly patients with FNFs. As already extensively reported in the literature,33-36 patients have a very high early mortality rate independent from clinical scores (HHS and OHS, in particular), therefore an early hospital discharge and a faster TUG test recovery could potentially be better indicators of the clinical status of the patients more than clinical scores by themselves. However, critical benefits for such a population of elderly patients with FNFs did not last more than 3 months after surgery, meaning that neither the OHS nor HHS differences reached a significant minimal clinically important difference. Despite the early favorable effects were not reached at the cost of increased peri-operative complications (similar to the DL approach, which is traditionally considered one of the safest approaches in hip arthroplasty), our current data did not show a clear advantage of the ABMS approach via the clinical outcomes.
Limitations are present in this study. First, due to its retrospective nature, the current study suffers from the inherent limitations and weaknesses of this type of studies. Randomization was not performed, and surgeons decided the surgical approach according to their own preferences. On the other hand, every surgery was performed by the same team of highly specialized surgeons, who regularly perform THA with both surgical approaches both for OA and FNFs, so limiting eventual bias linked to surgeon’s skill and experience. Another limitation of this study is the relatively short-term follow up, even if it must be considered that the first 2 post-operative years results are the most important in this specific population, since surgical complications are mainly encountered early. Third, the number of patients included in the study might be considered insufficient to achieve sufficient statistical power to find differences between groups in the main outcome variables.
Conclusions
The ABMS approach in THA for the treatment of FNFs allows for earlier mobilization, and better early functional outcome compared to the DL approach, but no functional advantage remained thenceforth. The ABMS approach is a proven and reliable choice to perform THA for FNFs, offering good outcome and faster recovery, similarly to total hip arthroplasties for degenerative arthritis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.