
Abstract
Introduction:
There is a projected exponential increase in the number of hip fractures in the United States. Trends in patient demographics and the role of total hip arthroplasty (THA) and its associated outcomes following hip fractures surgery have not been well studied.
Methods:
Patients with proximal femur fractures between 1990 and 2007 were identified in the National Hospital Discharge Survey database. Demographics, comorbidities, perioperative complications, and discharge status for patients undergoing THA, hemiarthroplasty, or internal fixation were examined. Multivariable regression was performed to determine independent risk factors for perioperative complications.
Results:
Between 1990 and 2007, there was a statistically significant increase in patient age, adverse events, medical comorbidities, surgical complications, medical complications, and nonroutine discharge across all surgical treatment modalities. In the same time period, the utilization of THA for all fracture types decreased significantly.
Discussion:
Total hip arthroplasty was found to be an independent risk factor for perioperative complications. Orthopedic surgeons should be aware that the hip fracture population continues to get older, with more medical comorbidities and are at higher risk for perioperative complications.
Conclusion:
Total hip arthroplasty is associated with a higher rate of perioperative complications in the hip fracture population.
Keywords
Introduction
There is a projected exponential increase in the number of hip fractures in the United States over the next 30 years. 1 As this patient population continues to get older, with more medical comorbidities and at higher risk for complications, special attention must be paid to the indications for total hip arthroplasty (THA) and its associated complications. Several studies have reported on successful use of cemented and noncemented hemiarthroplasty (HA) and THA for proximal femur fractures. 2 –5 Although the American Academy of Orthopaedic Surgeons (AAOS) has published hip fracture guidelines, 6 to the best of the authors knowledge, there is no consensus regarding the indications for THA in the hip fracture population. Prior literature examining national surgical trends in utilization of THA for the treatment of hip fractures have also shown mixed results. 7,8 The purpose of this study is to examine national trends in the utilization of THA for hip fractures by orthopedic surgeons in the United States, as well as report national trends in patient demographics, comorbidities, and perioperative complications for those undergoing arthroplasty or internal fixation procedures. Surgical and nonsurgical factors associated with an increased risk in perioperative complications were also identified.
The treatment for displaced femoral neck fractures in the elderly population has been hotly contested. Several studies have shown superiority of HA in this population over internal fixation; however, there is no consensus regarding when THA versus HA is indicated. 5,9 –13 In general, THA has been recommended for younger, more active patients, whereas HA has been recommended for older, lower demand patients. 4,12,13 Sassoon et al 14 demonstrated that THA has the potential for improved function, less long-term postoperative pain, and lower reoperation rates. However, these potential benefits may be associated with a higher risk of perioperative complications and increased anesthesia time. It is also important to note that patients with hip fractures are at higher risk of complications and adverse outcomes as compared to patients undergoing elective THA for osteoarthritis. 15,16
Although femoral neck fractures constitute the large majority of arthroplasty procedures performed for hip fractures, previous studies have also demonstrated good results in the use of cemented HA and THA for comminuted 4-part intertrochanteric fractures in older patients with poor bone quality. In a multicenter prospective trial, Kumar Gn et al 17 reported patients who underwent cemented HA for 4-part intertrochanteric fracture had comparable peri- and postoperative complications to those who underwent internal fixation. The authors demonstrated improvements in functional outcomes with fewer mechanical failures in long-term follow-up for cemented HA relative to internal fixation. However, there are no studies examining epidemiologic trends in utilization, demographics, and outcomes of HA versus THA in patients with intertrochanteric and subtrochanteric fractures.
Epidemiologic data have shown that the hip fracture population is getting older and with more medical comorbidities over the last 20 years. 18 –20 The current patient population may be at greater risk of complications following surgery compared to prior years. Total hip arthroplasty has been shown to require longer surgical times, increased blood loss, higher transfusion rates, pulmonary embolism, and mortality as compared to HA and internal fixation but can provide better outcomes and lower cost in the long term for younger patients. 14 A better understanding of trends in overall health care, surgical management, and the risk factors associated with perioperative complications in this population is needed.
We hypothesized that due to the aging hip fracture population with more medical comorbidities, there is a national trend in performing fewer THA by US orthopedic surgeons and an increased rate of perioperative complications following hip fracture surgery.
Methods and Materials
A retrospective epidemiological study was performed using the National Hospital Discharge Survey (NHDS). The NHDS is a publicly available, government-sponsored survey, conducted annually in order to provide data of nonfederal, short stay hospitals to the public. The sample data are weighted to provide nationwide estimates of annual inpatient care. The NHDS includes up to 7 medical diagnoses and 4 procedural codes per case, categorized by the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes. Additional information obtained by the NHDS includes patient demographic information, length of stay, and discharge disposition. The diagnostic and procedural codes used for this study are presented in Appendix A. Due to the decrease in survey size and a doubled relative standard error of the NHDS in 2008, the end point of this study was selected to be 2007. As this database has been made publicly available, the current study was exempt from institutional review board approval.
A total of 5 616 844 patients admitted to US hospitals between 1990 and 2007 with a primary diagnosis of a femoral neck, inter/peritrochanteric, or subtrochanteric fracture were identified. All patients with the previously mentioned diagnoses with a primary procedural code for open reduction internal fixation, HA, THA, internal fixation without reduction, and closed reduction with internal fixation were then selected, resulting in the 4 732 165 surgically treated hip fractures analyzed in the present study.
Comorbidity burden was quantified using Elixhauser coding algorithms as previously described. The Elixhauser comorbidity measure is a model consisting of 31 conditions and has recently been identified as a better predictor of mortality in patients undergoing orthopedic procedures than the Charlson Comorbidity Index. 21 Dichotomous variables for each Elixhauser comorbidity were created and χ2 tests were utilized to assess for each comorbidity’s association with mortality. The weighted Elixhauser score for each statistically significant comorbidity was generated as previously described by van Walraven et al. 22 The Elixhauser comorbidity score was then calculated for each patient by summing the individual weights of all comorbidities.
Postoperative adverse events were determined using the complication screening package as previously described. 23 –25 All adverse events were classified into 3 categories: general medical complications, mechanical complication, or surgical complications. Nonroutine discharge was defined as discharge to a short- or long-stay inpatient facility.
The study period was divided into 3 equal time periods in order to more accurately assess variation in patient demographics and outcomes throughout the large study time frame. Group 1 was comprised of patients who underwent surgical management of hip fractures from 1990 to 1995, group 2 from 1996 to 2001, and group 3 from 2002 to 2007.
Categorical data were analyzed with χ2 analysis and continuous data were analyzed with the independent-sample t test and analysis of variance. Multivariable binary logistic regression analyses were performed to assess the contributions of individual comorbidities to mortality, adverse events, and nonroutine discharge. Elixhauser comorbidities with a P value less than .10 in bivariate analysis and present in at least 0.2% of the population were included in the logistic regression modeling as previously described. 21 Odds ratios (ORs) and confidence intervals were calculated to assess the association between comorbidities and the dichotomous variables. A P value of <.001 was used to define statistical significance. 26,27 Statistical analyses were performed using SPSS version 21 (Armonk, New York).
Results
Patient demographics and perioperative outcomes for all hip fractures included in the analysis are detailed in Table 1. The average age of patients undergoing surgery for hip fractures were 78.0 ± 13.0, 80.0 ± 12.0, and 72.0 ± 21.0 years for femoral neck, peri-/intertrochanteric fractures, and subtrochanteric fractures, respectively (P < .001). For surgical fixation of femoral neck fractures, HA was the most common surgical procedure performed (61.3%) with 32.6% of patients undergoing internal fixation and 6.1% of patients undergoing THA (P < .001). Although internal fixation with intramedullary or extramedullary device was the treatment of choice for peri-/intertrochanteric and subtrochanteric fractures, a nonnegligible percentage of patients underwent arthroplasty procedures: 3.8% and 2.7%, respectively (P < .001).
Demographics and Outcomes in Patients With Hip Fractures in the United States From 1990 to 2007.a
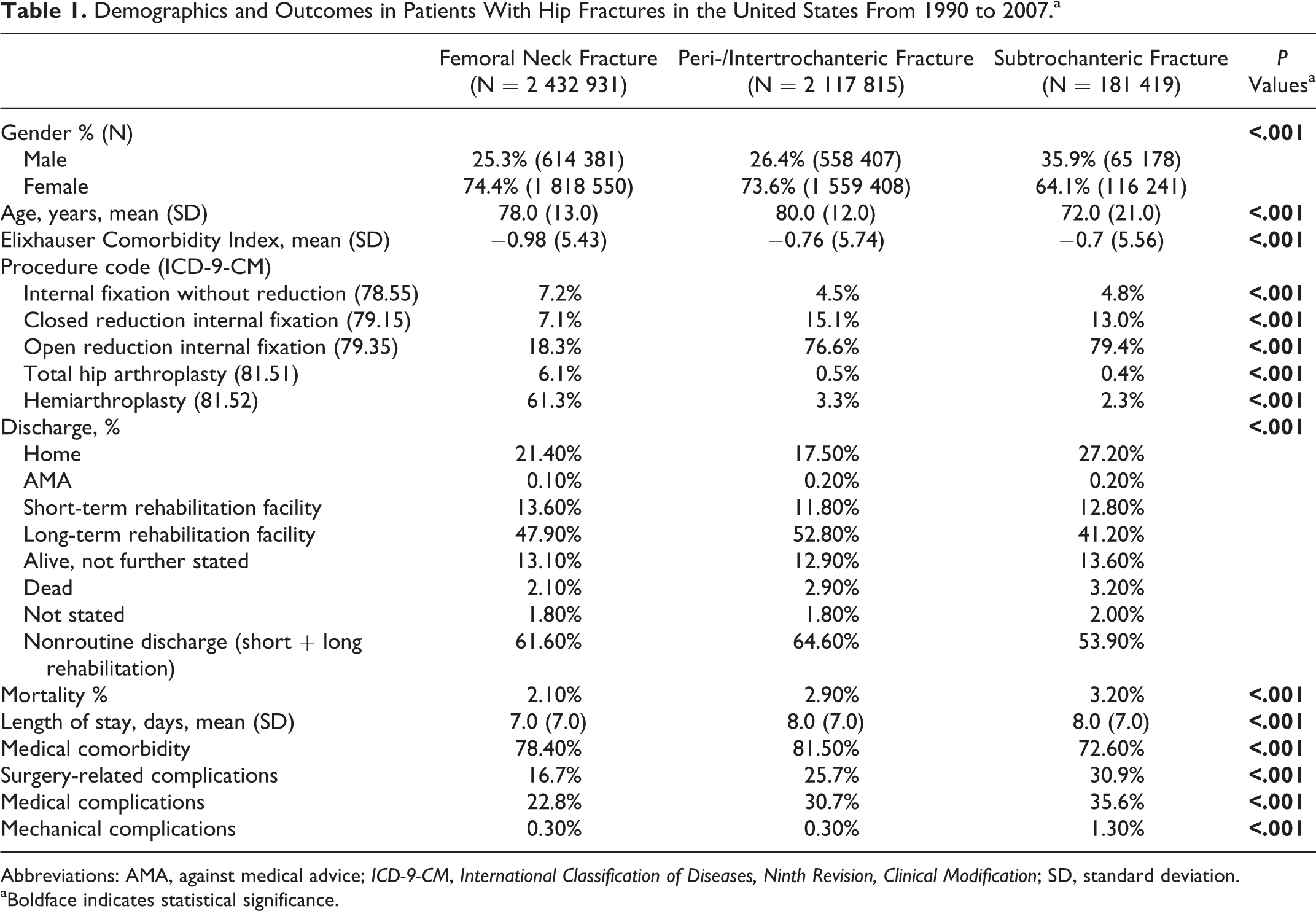
Abbreviations: AMA, against medical advice; ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification; SD, standard deviation.
aBoldface indicates statistical significance.
A higher percentage of patients with femoral neck (78.40%) and peri-/intertrochanteric (81.50%) fractures had an associated medical comorbidity as compared to patients with subtrochanteric fractures (72.6%; P < .001). Mortality (3.20%), surgical complications (30.9%), medical complications (35.6%), and mechanical complications (1.30%) were highest in the subtrochanteric fracture group (P < .001). Postoperatively, a higher percentage of patients with femoral neck or peri-/intertrochanteric fractures had nonroutine discharge, 61.6% and 64.4% respectively, as compared to 53.9% of patients with subtrochanteric fractures (P < .001; Table 1).
Table 2 details trends in patient demographics and outcomes for all patients surgically treated for hip fractures between 1990 and 2007. The percentage of patients older than 80 years have increased significantly between 1990 and 2007 with 55.5% in group 1 and 59.9% in group 3 (P < .001). The percentage of patients with a medical comorbidity increased from 73.2% in group 1 to 85.6% in group 3 (P < .001; Table 2, Figure 1). Medical complications mirrored the increase in medical comorbidities between 1990 and 2007 by increasing from 18.8% in group 1 to 35.6% in group 3 (P < .001; Table 2, Figure 1).

Comorbidity, complications, and mortality trends among patients surgically treated for hip fracture between 1990 and 2007.
Demographics and Outcomes in Patients With Hip Fractures Across Time Periods.a
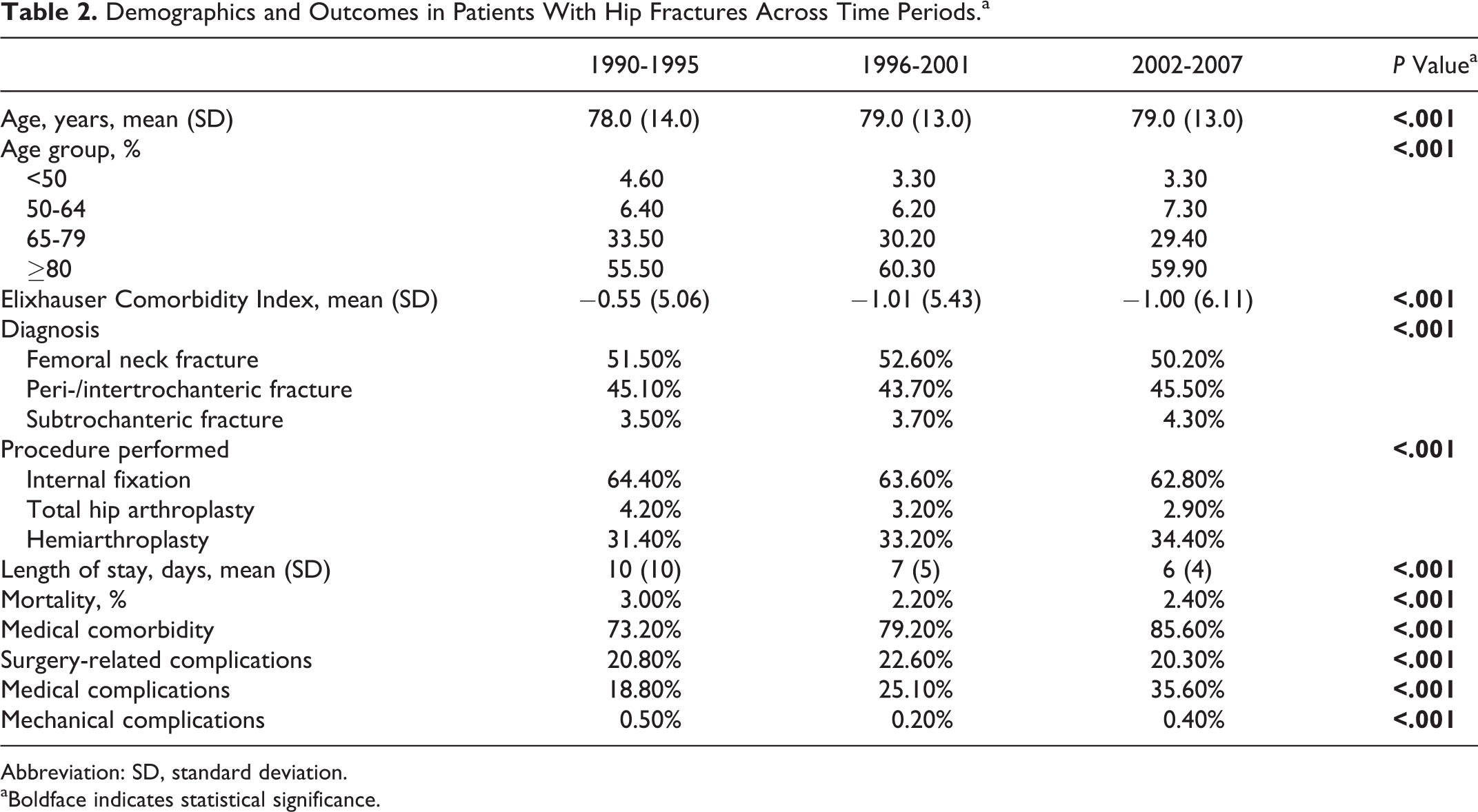
Abbreviation: SD, standard deviation.
aBoldface indicates statistical significance.
The utilization of THA for all hip fracture types between 1990 and 2007 decreased from 4.2% in group 1 to 2.9% in group 3 (P < .001; Table 2). During the same time periods, HA was increasingly utilized for all hip fractures (31.4%-34.4%) while the use of internal fixation utilization trended down (64.4%-62.8%; P < .001; Table 2). Figure 2 outlines trends in surgical fixation by fracture type between 1990 and 2007.

Operative trends in surgical fixation by fracture type between 1990 and 2007.
For femoral neck fractures, HA utilization has trended up uniformly (R 2 = .510), while THA (R 2 = .523) and internal fixation (R 2 = .264) have trended down. The use of arthroplasty procedure performed for subtrochanteric femur fractures has trended down (HA: R 2 = .011; THA: R 2 = .112), while internal fixation has trended up (R 2 = .122). The overall rate of THA utilization for all hip fractures trended down for all age groups with the largest decrease in patients older than 65 (65-79: R 2 = .249; ≥80: R 2 = .541; Figure 3). There was an increase in rate of HA in all age groups, except for patients ≤49 years old (≤49: R 2 = .116; Figure 3). For patients ≤49, there was a trend in increased utilization of internal fixation (R 2 = .144; Figure 3).
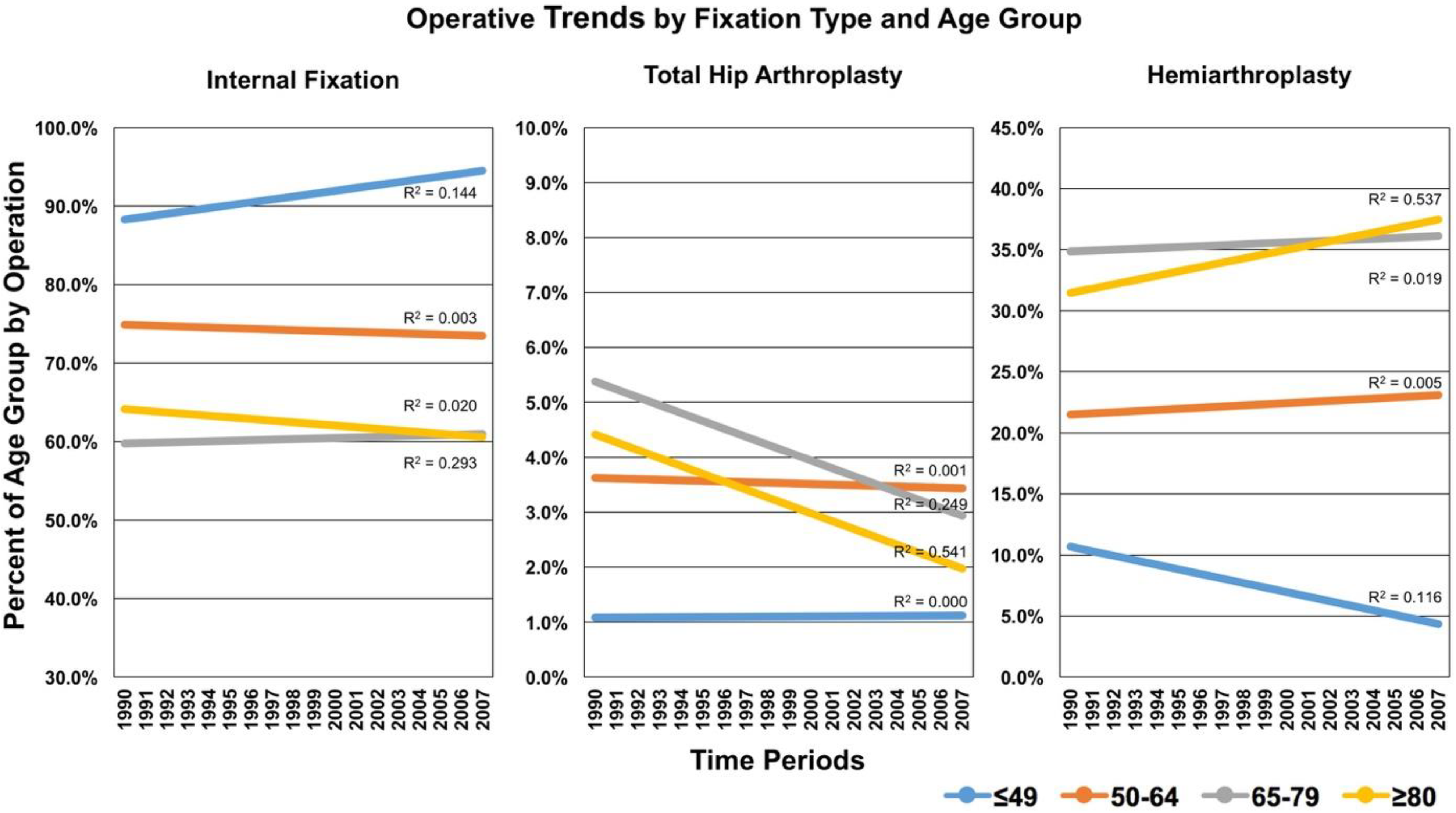
Operative trends by surgical fixation type and age group between 1990 and 2007.
Trends in comorbidities and outcomes by fracture type and procedure performed were analyzed. The percentage of patients with a medical comorbidity increased for all surgical methods and across all time periods, but the greatest increase was seen in the THA group (73.1%-87.5%; P < .001; Table 3). The length of stay decreased uniformly across all surgical methods (Table 3). However, routine discharge to home decreased and discharge to long-term rehabilitation facilities increased across all treatment modalities (Table 3).
Demographics and Outcomes in Patients With Hip Fractures Across Time Periods by Procedure.a

Abbreviations: SD, standard deviation.
aBoldface indicates statistical significance.
Table 4 lists the prevalence of complications for all patients undergoing surgical intervention for hip fractures and by surgical fixation type. Postoperative anemia (20.40%; P < .001) and transfusion (18.60%; P < .001) were the most common complications following all hip fracture surgeries. Total hip arthroplasty had a higher rate of postoperative anemia (20.00% vs 19.70%; P < .001), transfusion (19.30% vs 17.70%; P < .001), and acute pulmonary embolism (0.70% vs 0.60%; P < .001) compared to HA (Table 4). Patients undergoing THA had the highest rate of experiencing any adverse event across all time periods as compared to those undergoing HA (Table 3). The percentage of patients experiencing any adverse event postoperatively also increased across all time periods and by all procedure types (Table 3).
Prevalence of Adverse Events by Procedure Performed and in Total in Patients With Hip Fractures Between 1997 and 2007.a

Abbreviations: CRIF, closed reduction internal fixation; HA, hemiarthroplasty; IFnoRed, internal fixation no reduction; MI, Myocardial Infarction; ORIF, open reduction internal fixation; THA, total hip arthroplasty.
aBoldface indicates statistical significance.
Multivariable logistic regression analysis demonstrated that increasing age, male gender, and diagnosis of subtrochanteric fracture were the strongest predictors of mortality in patients with hip fractures (Table 5). Hemiarthroplasty was the procedure that was the strongest predictor of postoperative mortality (OR: 1.792; range: 1.731-1.856; P < .001). Total hip arthroplasty was the procedure that was the greatest predictor for experiencing any adverse events postoperatively (OR: 3.206; range: 3.162-3.251; P < .001; Table 6). With regard to nonroutine discharge, increasing age was the strongest independent risk factor for discharge to a short or long-term rehabilitation facility (OR: 2.322, 6.283, 10.980: P < .001; Table 7).
Logistic Regression for Predictors of Mortality Among Patients With Hip Fractures.a

Abbreviations: CI, confidence interval; OR, odds ratio.
aBoldface indicates statistical significance.
bAge groups relative to age 0 to 49 years cohort.
cDiagnosis relative to femoral neck fractures.
dProcedure relative to internal fixation without reduction.
Logistic Regression for Predictors of Any Adverse Event Among Patients With Hip Fractures.a
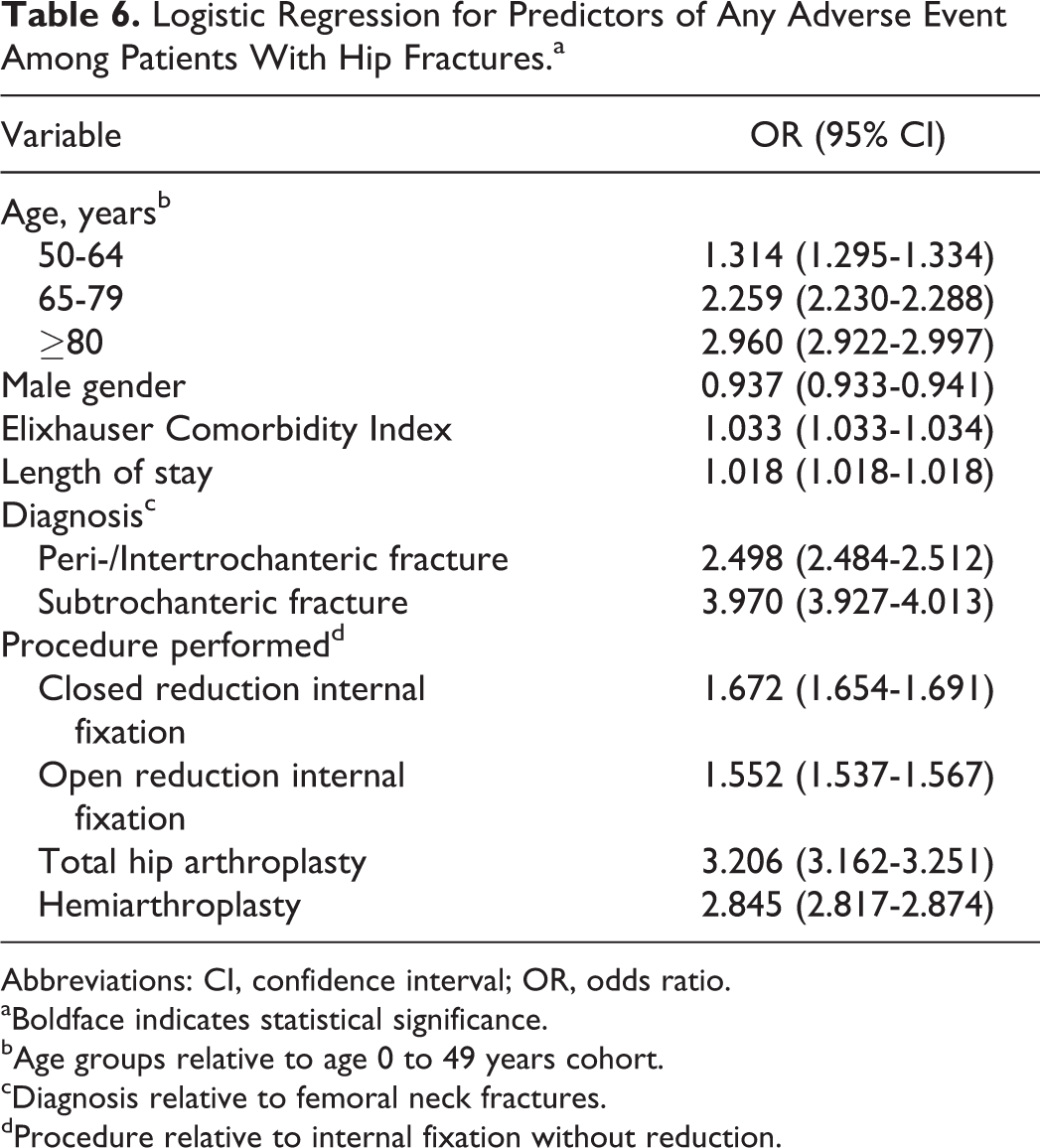
Abbreviations: CI, confidence interval; OR, odds ratio.
aBoldface indicates statistical significance.
bAge groups relative to age 0 to 49 years cohort.
cDiagnosis relative to femoral neck fractures.
dProcedure relative to internal fixation without reduction.
Logistic Regression for Predictors of Nonroutine Discharge (to a Short- or Long-Term Rehabilitation Facility) Among Patients With Hip Fractures.a

Abbreviations: CI, confidence interval; OR, odds ratio.
aBoldface indicates statistical significance.
bAge groups relative to age 0 to 49 years cohort.
cDiagnosis relative to femoral neck fractures.
dProcedure relative to internal fixation without reduction.
Discussion
The limitations of our study are those inherent with a retrospective database review. One of the possible errors introduced into the data set are errors and variation in coding of procedures performed, medical comorbidities, and outcome measures. The risk of variation among coding strategies was minimized with the use of a large population from a well-established national database with a large population of different surgeons contributing their data. An important limitation is that our data only contains information for a single hospital stay; therefore, long-term clinical outcomes, readmissions, and return to the OR could not be analyzed. Additionally, the information analyzed is limited to the comorbidities, outcome measures, and organization of subgroups gathered by the NHDS. Therefore, clinical outcome scores, costs by procedure, and the effects of readmissions on functional outcomes are underrepresented by the data of the current study.
Our results support recent epidemiological studies that have shown that the hip fracture population has gotten older and with more medical comorbidities. 28 –30 The advent of bisphosphonate therapy and their impact on decreasing fragility fractures along with increased life expectancy in US patients’ likely account for hip fractures occurring in older individuals in recent years. 31 Between 1990 and 2007, the percentage of patients with hip fractures older than 80 years rose by more than 7%. In the same time period, we found that the percentage of patients with a medical comorbidity rose by nearly 28%. Consistent with previous studies which have demonstrated that age and medical comorbidities are associated with poor outcomes following hip fracture surgery, these changes in patient demographics suggest that the hip fracture population is at higher risk of perioperative complications now than in years past. 32,33
Although mortality has decreased from 1990 to 2007 by nearly 20%, medical complications, surgical complications, and adverse events perioperatively have increased significantly in this population. Our findings suggest that although physicians may be better at treating perioperative complications and preventing mortality, an older, more sick patient population is the likely culprit for a higher rate of adverse events following hip fracture surgery. Multi-organ disease and decreased physiological reserve put these patients at greater risk of postoperative complications.
Although HA was the procedure of choice for femoral neck fractures, approximately 6% of patients in our study underwent THA. Our results support those of Jain et al 34 in that we found a decrease in utilization of THA in patients with all types of hips fractures in recent decades. This validated our hypothesis as we anticipated that with an aging population with a higher rate of medical comorbidities, fewer patients would be candidates for THA. Our results differ from those of Miller et al 7 who found an increase in utilization of THA. However, the previously analyzed data are from case logs of newly graduated orthopedic surgeons and may not accurately represent overall trends in the country for all surgeons. The authors reported that a lower percentage of new graduates are treating hip fractures and a higher percentage of those who are performing THA. Subspecialization trends in orthopedics and recent literature suggesting superiority of THA versus HA may explain why some recent graduates are more commonly performing THA for hip fractures. 7
A small percentage of patients with intertrochanteric/peritrochanteric fractures underwent arthroplasty procedures. One of the limitations of our study is that due to ICD-9 coding limitations we are unable to determine the degree of displacement or comminution of these fractures in which arthroplasty procedures were performed or whether or not cementing of the prosthesis was performed. There are reports in the literature which show that cemented arthroplasty is an attractive treatment option in older patients with poor bone quality following 4-part proximal femur fractures. 2,3 Although our data suggests that THA is associated with a higher rate of perioperative complications as compared to HA, future studies are needed to compare outcomes in patients undergoing cemented/uncemented THA and HA for comminuted proximal femur fractures.
Age, HA, male gender, and subtrochanteric fracture were the strongest predictors of mortality. Although our regression model accounted for medical comorbidities, our data does not directly factor for patient’s functional status. In general, the literature recommends that patients who are older and with lower functional demand should be offered HA over THA. Previous studies have shown that poor preoperative walking capacity and poor activities of daily living are strong predictors of postoperative mortality. 35 Undergoing HA therefore may serve as a surrogate marker for functional status. Our results are also consistent with prior studies which have shown that increasing age is predictor of postoperative mortality. 32 The association with subtrochanteric fracture and male gender with higher energy trauma, polytrauma, and mortality may also explain our findings that this fracture type is a risk factor for mortality. 33,35
An adverse event was defined as either a mechanical, medical, and surgical complication in the perioperative period throughout the inpatient stay. Our regression analysis which accounted for age, fracture type, procedure, and medical comorbidities showed that THA was an independent risk factor for any adverse events in the perioperative period when compared to either internal fixation or HA. Total hip arthroplasty had similar ORs predicting adverse events as carrying the diagnosis of CHF or atrial fibrillation in patients with hip fractures treated surgically. Consistent with prior studies, patients undergoing THA also had a significantly higher rate of PE and requirement of blood transfusions as compared to patients undergoing HA. These findings are not unexpected given the higher complexity of surgery, increased OR time, and reaming of the acetabulum in THA. However, these explanations are only hypothetical because neither the study design nor the variables examined allow us to make such conclusions. Although THA is a relatively safe procedure, the hip fracture population is at higher risk of complications than the primary elective THA population. Orthopedic surgeons should be aware that national trends demonstrate the hip fracture population is getting older and with more medical comorbidities and at higher risk of complications than in years past. Moreover, although THA has been reported to show better functional outcomes and lower reoperation rates, it is also an independent risk factor for adverse events in the perioperative period such as anemia, transfusion, and PE when compared to HA. National trends in decreased utilization for THA may be an indicator that fewer patients are candidates for THA compared to HA. Special care must be taken when deciding which patients with hip fractures are candidates for THA.
Footnotes
Appendix A
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.