
Abstract
Introduction:
The percentage of elderly population is increasing worldwide, with increasing incidence of femoral neck fractures. An increasing trend of arthroplasty for femoral neck fracture is observed. We aim to retrospectively analyze the preoperative factors that seem to influence the decision between hemiarthroplasty and total hip arthroplasty for managment of the same.
Materials and Methods:
Patients admitted with femoral neck fracture during January 2010 to March 2015 in our institute were included in the study. The preinjury independency status was assessed using Katz index scoring system. Based on the data obtained from case sheets, the patients were segregated into hemiarthroplasty group and total hip arthroplasty group. Variables that preferentially appeared in the individual group were identified.
Results:
A total of 206 hips of 199 patients were included in the study. The factors that seem to influence the decision between hemiarthroplasty and total hip arthroplasty with a statistical significance were age, Katz index score, and American Society of Anesthesiologists (ASA) grade. Higher ASA grades caused delay in surgery, increasing the length of hospital stay, and these patients more commonly underwent hemiarthroplasty.
Discussion:
Patients’ preinjury functional status influenced the decision between hemiarthroplasty and total hip arthroplasty, especially in the age between 65 and 80 years. Preoperative comorbidities did not prevent the patient from undergoing total hip replacement due to early optimization for surgery with the help of the dedicated orthogeriatric team.
Conclusion:
We conclude that preinjury functional independency of a patient is an important decisive factor in the choice between hemiarthroplasty and total hip arthroplasty. In addition to other factors including age and comorbidity pattern, scoring methods for preinjury functional status of patient could aid in decision-making. Early optimization, early surgery, and faster rehabilitation help the patients to achieve their preinjury functional status.
Keywords
Introduction
Hip fracture incidence is on the rise globally, with increase in aging population worldwide. Projected figures say the incidence of hip fracture will increase from 1.66 million in 1990 to 6.6 million by 2050. 1 Globally, North America and Sweden have the highest reported incidence of hip fractures. 2 India being the second most populous country in the world is projected to have a population of 82.2 million, who will be over 65 years of age by 2020. 3 Studies regarding the hip fracture incidence are still not available in India. 4 The projected figures 5 show that the current annual hip fracture incidence in India is 440 000 with a female to male ratio of about 3:1. It is expected to reach 600 000 by 2020 and more than 1 million in 2050. 5 There are well-established management protocols for hip fracture in adults, suggesting fracture fixation for extracapsular fractures and arthroplasty for displaced intracapsular fractures. 6 –8 Published literature show a rising trend in arthroplasty for femoral neck fracture and also elaborate on the advantages and risks involved. 9,10 There is ongoing debate regarding the method of replacement—hemiarthroplasty or total hip arthroplasty (THA)—best suited for management for intracapsular fractures. 10 –12 We aim to retrospectively analyze the preoperative factors that seem to influence the decision between hemiarthroplasty and THA in patients admitted to the trauma unit. Institutional review board approval for study was obtained, and informed consent obtained from the patients to use their clinical data.
Materials and Methods
Between January 2010 and March 2015, patients admitted in the trauma unit of our institution for femoral neck fractures were included in the study. All cases included in the study were displaced type 3 or 4 of Garden classification. The preinjury independency status of the patient was assessed using Katz index of independence in activities of daily living. 13 –15 This scoring system is based on the independency of the patient in performing daily activities such as bathing, dressing, toileting, transferring, continence, and feeding. Each of the above activities was scored 1 if performed without any assistance and 0 if required assistance. The maximum score of 6 indicated fully independent patient. A score of 4 indicates moderate impairment, and a score of 2 or less indicated full dependency. Case sheets were obtained from the medical records department and were analyzed for the variables presented in Table 1. Data were segregated into hip hemiarthroplasty (HHA) group and THA group. No matching done. Demographic data obtained is represented in Table 2. Variables that preferentially appeared in the individual group were identified. Statistical analysis was performed using SPSS software version 19.0 and Microsoft Excel version 2013.
Variables Retrospectively Analyzed From Patient Case Sheets.

Abbreviations: ASA, American Society of Anesthesiologists; ICU, intensive care unit.
Demographic Data.
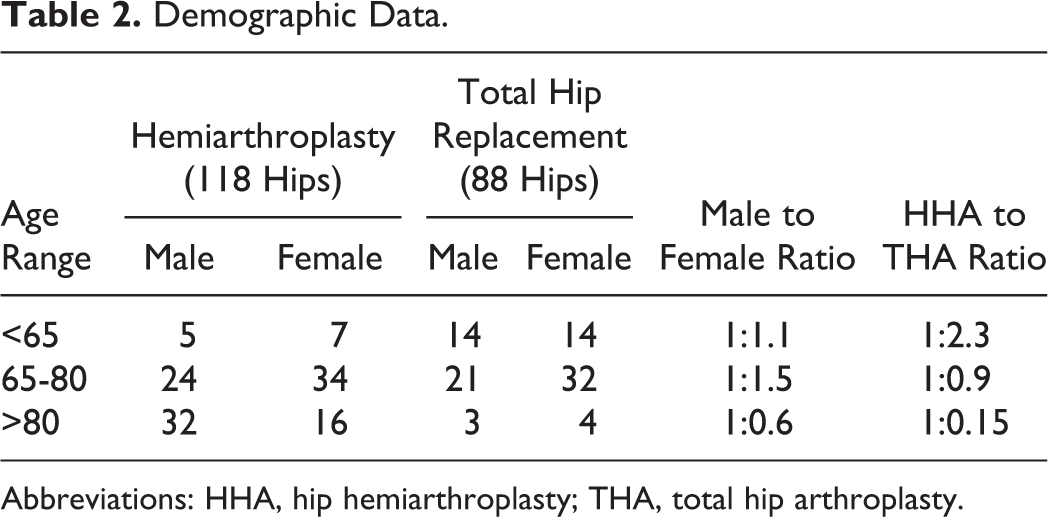
Abbreviations: HHA, hip hemiarthroplasty; THA, total hip arthroplasty.
Results
Of the 334 arthroplasty procedures performed during the abovementioned period, 227 were for femoral neck fractures, but 21 cases were excluded as they involved nonunion of femoral neck fractures. Remaining 206 hips of 199 patients that presented as acute trauma cases were included in the study. There was no case of simultaneous bilateral femoral neck fractures, though 7 patients who had already had femoral neck fracture on one side presented with fractures on the contralateral side, with time gap between the fractures. Of the two, HHA procedure was commonly used, constituting 57.28% of the total arthroplasty procedures. In this study group, the average age of the patient admitted for femoral neck fracture was 75 years for males and 72 years for females with an overall female preponderance. We found that fracture occurred more commonly on left side, with an incidence of 52.43% though statistically insignificant. Domestic fall was the most common reason for fracture, with an incidence of 88.35%. The other reasons for fracture included road traffic accident (9.71%), animal violence (1.46%), and assault (0.49%). In the HHA group, the average gap between injury and admission was 2.75 days in contrast to 1.67 days in the THA group, indicating that the HHA group presented late to hospital. The average gap between admission to surgery was 3.06 days in the HHA group and 2.48 days in the THA group, indicating patients who underwent HHA required more time for fitness optimization to undergo surgery. In this study, the average Katz index score of HHA group was 1.95 while that of THA group was 5.50. In HHA group, 15.53% patients needed preoperative blood transfusion for optimization compared to 9.22% patients in THA group, indicating that patients in the HHA group were more commonly anemic which was clinically significant but statistically insignificant. Other preexisting medical illness in both groups are summarized in Table 3, from which it is clearly evident that the patients in the HHA group had more comorbidities to deal with. We accepted American Society of Anesthesiologists (ASA) grading done by our anesthetists as an indicator for assessing comorbid conditions, as it is one of the globally accepted preoperative assessment methods. 16 –18 With regard to ASA grading, 77.97% of patients in the HHA group had a score of 3 to 4 compared to THA group (53.41%), indicating that THA group was relatively healthier than the other. On calculation of odds ratio for preoperative study variables which seemed to influence the decision between HHA and THA, the factors which were strongly associated with HHA were age >80 years, ASA grade of 3 or 4, and Katz index score of 1 to 4. Details are summarized in Table 4. The requirement of intraoperative blood transfusion was more among the THA group (8%) compared to the HHA group (3%), indicating relatively more blood loss and more theater time with this surgery. The decision regarding use of cement was based on the surgeon’s assessment of individual bone quality, which did not affect the decision between HHA and THA. The frequency of cement use is indicated in Figure 1. With a total 104 cemented procedures in both categories put together, there was no incidence of cement-associated complications. Following surgery, all patients were monitored in intensive care unit for 24 hours as this was the standard protocol in our institution and mobilized the next day unless required otherwise. Stay in intensive care unit for more than 24 hours was noted in 9.4% of HHA patients and 3.4% of THA patients. All patients were planned for mobilization the next day and discharged on eighth postoperative day unless the patient’s status did not permit so. All patients underwent standard physiotherapy protocol with the help of a dedicated physiotherapy team. All patients were discharged to their respective homes once they returned to their preinjury dependency status. The average length of stay in hospital for HHA patients was 13.57 days and for THA patients it was 12.58 days. Table 5 shows independent t test comparing the difference in mean values for selected criteria. Table 6 shows the χ2 test comparing the difference in proportion between the 2 groups. The preop factors that had a statistical significance were age, Katz index score, and ASA grade.
Incidence of Preoperative Comorbid Condition.

Abbreviations: THA, total hip arthroplasty; CABG, coronary artery bypass grafting; COPD, chronic obstructive pulmonary disease.
Calculation of Odds Ratio for Hemiarthroplasty Versus THA.a

Abbreviations: ASA, American Society of Anesthesiologists; THA, total hip arthroplasty.
aThe reference value of OR 1 refers to having a hemiarthroplasty. Ranges above OR 1 favor hemiarthroplasty. Ranges below OR 1 favor THA.

Frequency of cementation.
Independent t Test Comparing the Difference in Mean Values.

Abbreviations: HHA, hip hemiarthroplasty; THA, total hip arthroplasty; S, statistically significant; NS, statistically insignificant; ICU, intensive care unit.
Chi-Square Tests Comparing the Difference in Proportions in 2 Types of Surgeries.

Abbreviations: ASA, American Society of Anesthesiologists; GA, general anesthesia; HHA, hip hemiarthroplasty; THA, total hip arthroplasty; S, statistically significant; NS, statistically insignificant; RTA, renal tubular acidosis.
Discussion
The life expectancy of an Indian citizen increased from 53.875 years during 1980 to 68.014 years during 2014. 19 This may soon translate into increase in health-care cost of the aging population in India. The treatment algorithm for efficient management of hip fractures is well established in Western literature. 6 –8 Few studies elicit the problem of hip fractures in India, highlighting the clinical and socioeconomic challenges in the management of hip fractures. 20,21 On admission, the prime target would be to optimize the patient for surgery, needing the care of an orthogeriatric team, as rightly highlighted by Lau et al, Jain et al, and Rocca et al. 20,22,23 Identifying the key elements in this orthogeriatic assessment is of vital importance to provide a targeted approach for individual patient, as highlighted by popular established guidelines. 6 –8,24 Our search of literature showed that controversy exists in deciding between HHA and THA when considering patient’s age, with evidence supporting both. 11,12,25,26 Although age is an important criterion, we concur with authors who stress on the patient’s preinjury functional status to decide between HHA and THA, especially in the age between 65 and 80 years. 27 Preoperative comorbidities of hypertension, diabetes mellitus, cardiac illness, hypothyroidism, and vitamin D deficiency could be very well managed with a dedicated physician team and optimize the patient for surgery, and hence these factors did not prevent the patient from undergoing THA, which is usually considered more demanding. Our results concurred with that of Yeoh and Fazal, who concluded that higher ASA grades caused delay in surgery, increasing the length of hospital stay. 28 We found that patients with higher ASA grades more commonly underwent HHA, as also reported by Miller et al. 29 The main drawback in our study was being a retrospective single-center study involving small number of patients without any randomization or matching. Other factors that were not included in our study, such as body mass index, abbreviated mental test score for individual patient, smoking, and alcohol consumption, have a bearing in the decision between HHA and THA, as noted by Miller et al. 29 Another drawback of this study is that the patient’s socioeconomic status was not included, which could have been an important factor in deciding between HHA and THA since most of the patients in the study group paid for their health expenses and were not covered by health insurance.
Conclusion
It is concluded that our study concurs with the idea that young, active, functionally independent patient may be offered THA in preference to HHA. Future randomized multicenter studies in India would help bring out evidence about functional outcome in patients undergoing THA or HHA. Scoring methods for preinjury functional status of patient could aid in the decision-making in addition to other factors, including comorbidity pattern. Early optimization by a dedicated orthogeriatric team and adhering to standard physiotherapy protocol would provide good results in patients undergoing the procedure. Early surgery and faster rehabilitation help the patient to achieve the preinjury functional status.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.