
Abstract
Displaced femoral neck fractures are common injuries in the elderly individuals. There is controversy about the best treatment with regard to total hip arthroplasty (THA) versus hemiarthroplasty. This study uses the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) database to evaluate the preoperative risk factors associated with the decision to perform THA over hemiarthroplasty. We also evaluate the risk factors associated with postoperative complications after each procedure. Patients older than 50 years undergoing hemiarthroplasty or THA after fracture in the NSQIP database from 2007 to 2010 were compared to each other in terms of preoperative medical conditions, postoperative complications, and length of stay. Multivariate logistic regression models were used to adjust for preoperative risk factors for undergoing a THA versus a hemiarthroplasty and for complications after each procedure. In all, 783 patients underwent hemiarthroplasty and 419 underwent THA for fracture. Hemiarthroplasty patients had longer hospital stays. On multivariate logistic regression, the only significant predictor for having a THA after fracture over hemiarthroplasty was being aged 50 to 64 years. The patient characteristics/comorbidities that favored having a hemiarthroplasty were age >80 years, hemiplegia, being underweight, having a dependent functional status, being on dialysis, and having an early surgery. High body mass index, American Society of Anesthesiologists (ASA) class, gender, and other comorbidities were not predictors of having one procedure over another. Disseminated cancer and diabetes were predictive of complications after THA while being overweight, obese I, or a smoker were protective. High ASA class and do-not-resuscitate status were significant predictors of complications after a hemiarthroplasty. This study identified clinical factors influencing surgeons toward performing either THA or hemiarthroplasty for elderly patients after femoral neck fractures. Younger, healthier patients were more likely to receive THA. Patients particularly at higher risks of complications after hemiarthroplasty should be monitored closely.
Keywords
Introduction
Hip fractures are common orthopedic injuries in the elderly individuals. In 1996, approximately 340 000 hip fractures occurred in the United States, most often among women aged more than 65 years. 1 Caring for patients following a hip fracture presents an increasing burden not only on our health care system but also on the patients themselves as these injuries represent a life-changing event that has a 20% to 30% 1-year mortality rate. 2 –4 Additionally, the average lifetime cost incurred by sustaining a hip fracture is as high as US$81 300 of which US$19 937 is incurred at the initial hospitalization and the remainder from subsequent long-term care in nursing homes and lost wages and productivity of the patient’s family. 2,5 –7
Although the standard treatment algorithm for extracapsular, intertrochanteric hip fractures is well accepted, the treatment for intracapsular femoral neck fractures is more controversial. 8 Femoral neck fractures in elderly individuals are commonly classified according to the Garden classification. Nondisplaced fractures (Garden I and II) are usually treated with hip preservation, and displaced fractures (Garden III and IV) are generally treated with arthroplasty in elderly patients. 9
The primary indication for arthroplasty in patients with displaced femoral neck fractures is to avoid fracture nonunion and avascular necrosis in patients treated with internal fixation, which has been reported to be as high as 39%. 10,11 Many surgeons prefer to treat displaced femoral neck fractures with a hemiarthroplasty, particularly in very elderly patients. 8 However, numerous studies have been published demonstrating that functional outcomes, walking distance, self-reported pain scores, and hip disability indices are superior for patients treated with a total hip arthroplasty (THA) as compared to hemiarthroplasty. 11 –19 It has similarly been shown that although hemiarthroplasty is less expensive in the short term, total hip replacement is generally more cost effective in the long term due to the lower revision rates. 10,11,20 In contrast, the complexities of performing a total hip replacement for femoral neck fracture include an increased rate of dislocation, longer operative times, greater blood loss, and a more technically demanding operation. 8,11 –14,17 –19
As detailed earlier, there have been numerous studies evaluating the long-term outcomes following THA and hemiarthroplasty after a femoral neck fracture. However, one aspect that is missing from the literature is an evaluation of the preoperative factors that influence the choice to perform either a hemiarthroplasty or a total hip replacement.
The American College of Surgeons National Surgical Quality Improvement Project (ACS NSQIP) database collects data from multiple centers about preoperative patient characteristics and short-term postoperative complications. Using this database, we sought to (1) evaluate the preoperative factors associated with the decision to treat patients with a total hip replacement or hemiarthroplasty and (2) compare which preoperative factors were associated with complications following these 2 surgeries.
Materials and Methods
Data Source
The ACS NSQIP is a prospective, risk-adjusted, multi-institutional outcomes program. The details of data collection strategies, inclusion criteria, sampling procedures, and outcomes measured in the ACS NSQIP have been reported. 21 –23 The ACS NSQIP collects data from 258 medium-to large-sized private hospitals in the entire United States in both the inpatient and the outpatient settings. Hospitals in the ACS NSQIP need to submit 1 680 cases per year and must hire at least 1 full-time surgical clinical reviewer to collect the data. The data collected consist of 135 HIPAA (Health Insurance Portability and Accountability Act)-compliant variables, including preoperative comorbidities, intraoperative variables, and 30-day postoperative morbidity, and mortality outcomes for patients undergoing major surgical procedures.
The ACS NSQIP data from 2007 to 2010 were utilized. Using Current Procedural Terminology (CPT) codes, we identified all patients who underwent hemiarthroplasty or THA. We then cross-referenced these CPT codes with the International Classification of Diseases, Ninth Revision, Clinical Modification diagnosis code listed for each patient to determine whether the procedure was performed in a setting of fracture. Patients with additional CPT codes were excluded from the analysis, indicating they underwent a second unrelated procedure (ie, humerus repair, arthroscopy of knee, vascular procedures, etc) under the same anesthetic period. We also excluded patients who had CPT codes indicating the hip arthroplasty procedure was secondary to removal of a bone tumor as well as patients who were <50 years of age, in a coma, pregnant, ventilator dependent, or who had missing data. Independent demographic variables include patient sex, age group (50-64, 65-79, and ≥80 years), race, and body mass index (BMI) divided into 6 categories based on the World Health Organization guidelines: underweight (<18.5 kg/m2), normal (18.5-24.9 kg/m2), overweight (25-29.9 kg/m2), obese I (30-34.9 kg/m2), obese II (35-39.9 kg/m2), and obese III (≥ 40kg/m2).
Independent process-of-care variables included type of anesthesia, whether the procedure was classified as emergent (occurring within 12 hours of admission), which we redefined as “early surgery,” and a variable for the greatest level of resident surgeon participating in the case. Independent clinical characteristics of patients included American Society of Anesthesiologists (ASA) classification, functional status prior to operation, and a medical history describing system-specific and general comorbidities.
Outcome Variables
The primary outcomes of interest were to identify the comorbidities and clinical characteristics of patients undergoing hemiarthroplasty versus those of patients undergoing THA after fracture. Other clinical outcomes of interest were as follows: 30-day postoperative complications, return to the operating room, and death. Complication variables were grouped into the following categories: wound (includes superficial, deep, organ/space surgical site infection, and wound disruption), septic (sepsis and septic shock), cardiac (cardiac arrest requiring cardiopulmonary resuscitation and myocardial infarction), respiratory (pneumonia, unplanned intubation, and failure to wean off ventilator), urinary (progressive renal insufficiency, acute renal failure, and urinary tract infections), and central nervous system (cerebrovascular accident/stroke with neurological deficit, coma >24 hours, and peripheral nerve injury). Other complication variables include pulmonary embolism, deep vein thrombosis/thrombophlebitis, graft/prosthesis/flap failure, receiving a blood transfusion either intraoperatively or postoperatively, and a one or more overall complication variable (includes all complications and death and excludes blood transfusions). The complications were treated as dichotomous variables (none vs ≥ 1). Length of stay (LOS) was treated as a continuous variable.
Statistical Analysis
A univariate analysis of the independent variables by our outcomes of interest was performed by chi-square statistical analysis for categorical variables. An independent samples t-test was used to compare the mean hospital LOS of patients undergoing THA versus hemiarthroplasty. Multivariate logistic regression models were used to adjust for independent variables for type of hip surgical procedure, for having an overall complication after THA, and for having an overall complication after hemiarthroplasty. Preoperative predictor variables used in the multivariable analysis included patient demographics, clinical characteristics, and preoperative risk factors. The preoperative variables that were included into the regression models had a P ≤ .20 on univariate associations. A backward stepwise approach was used for the multivariable analysis, using a P value of ≤.05 for entry and a P value of ≥.10 for removal from models. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. Data analysis and management were performed using SPSS version 19.0 (Chicago, Illinois). All tests were 2-sided, with statistical significance set at a P value of ≤.05. This study was deemed exempt from institutional review board approval at our institution because ACS NSQIP is a public database with no personal identifying information.
Results
A total of 783 patients underwent hemiarthroplasty and 419 patients underwent THA for fracture. Differences in patient demographic and clinical characteristics and comorbidities by arthroplasty procedure are shown in Tables 1 and 2, respectively. Compared to the hemiarthroplasty patients, patients undergoing THA were more likely to be men, younger (age 50-64 years), functionally independent in their activities of daily living, have a higher BMI (overweight or obese class I-III), and have a lower ASA class but less likely to have early surgery (all P < .05). The THA patients were more likely to smoke, drink alcohol, and be on chronic corticosteroids but less likely than hemiarthroplasty patients to be on dialysis, have had a stroke with neurological deficits, be hemiplegic, or have an open wound/wound infection, bleeding disorder, impaired sensorium, or DNR status (all P < .05).
Demographic and Clinical Characteristics of Patients Undergoing Hemiarthroplasty Versus Total Hip Arthroplasty for Fracture.a,b,c

Abbreviations: BMI, body mass index = bodyweight (kg)/height2 (m)2; ASA, American Society of Anesthesiologists; PGY, post-graduate year; MAC, monitored anesthetic care.
a N = 1202.
b Percentages have been rounded and may not add to 100.
c The P values reported in the table in the grey boxes indicate the results from the chi-square analysis for that variable overall. Individual comparisons are not made between each subheading.
Comorbidities of Patients Undergoing Hemiarthroplasty Versus Total Hip Arthroplasty for Fracture.a,b

Abbreviations: PCI, percutaneous coronary intervention; HTN, hypertension; COPD, chronic obstructive pulmonary disease; CNS, central nervous system; preop, perioperatively; DNR, do-not-resuscitate.
a N = 1202.
b Percentages have been rounded and might not sum to 100.
Unadjusted Outcomes
Compared to the patient group who underwent hemiarthroplasty, the patients who underwent THA for fracture were more likely to have received a blood transfusion (14.4% vs 22.7%, P < .01) but less likely to have had one or more complication (excluding blood transfusion) overall (18.9% vs 13.6%, P < .05) as shown in Table 3.
Complications of Patients Undergoing Hemiarthroplasty Versus Total Hip Arthroplasty for Fracture.a,b

Abbreviations: CNS, central nervous system; DVT, deep vein thrombosis; OR, odds ratio; intraop, intraoperatively; postop, postoperatively.
a N = 1202.
b Percentages have been rounded and might not sum to 100.
Patients undergoing THA had on average shorter lengths of hospitalization compared to hemiarthroplasty patients (mean LOS = 5.48 days vs 7.03 days, respectively; mean LOS difference 1.55 days (95% CI: 1.001-2.101 days); P < .001.
Adjusted Outcomes
On a multivariable logistic regression (Figure 1), the only patient characteristic/comorbidity that was a predictor for having a THA after fracture was being of age 50 to 64 years. The patient characteristics/comorbidities that were predictors that favor hemiarthroplasty were age ≥80 years, being underweight, having a dependent functional status, being on dialysis, hemiplegia, and having an early surgery. The following were not predictors of having one procedure over another: high BMI (includes overweight and obese I-III classes), ASA class, gender, chronic corticosteroid use, or having a wound infection, history of stroke with neurological deficit, history of TIA, impaired sensorium, history of peripheral vascular disease, hypertension, previous cardiac surgery, DNR status, alcohol use, or being a smoker (data not illustrated).
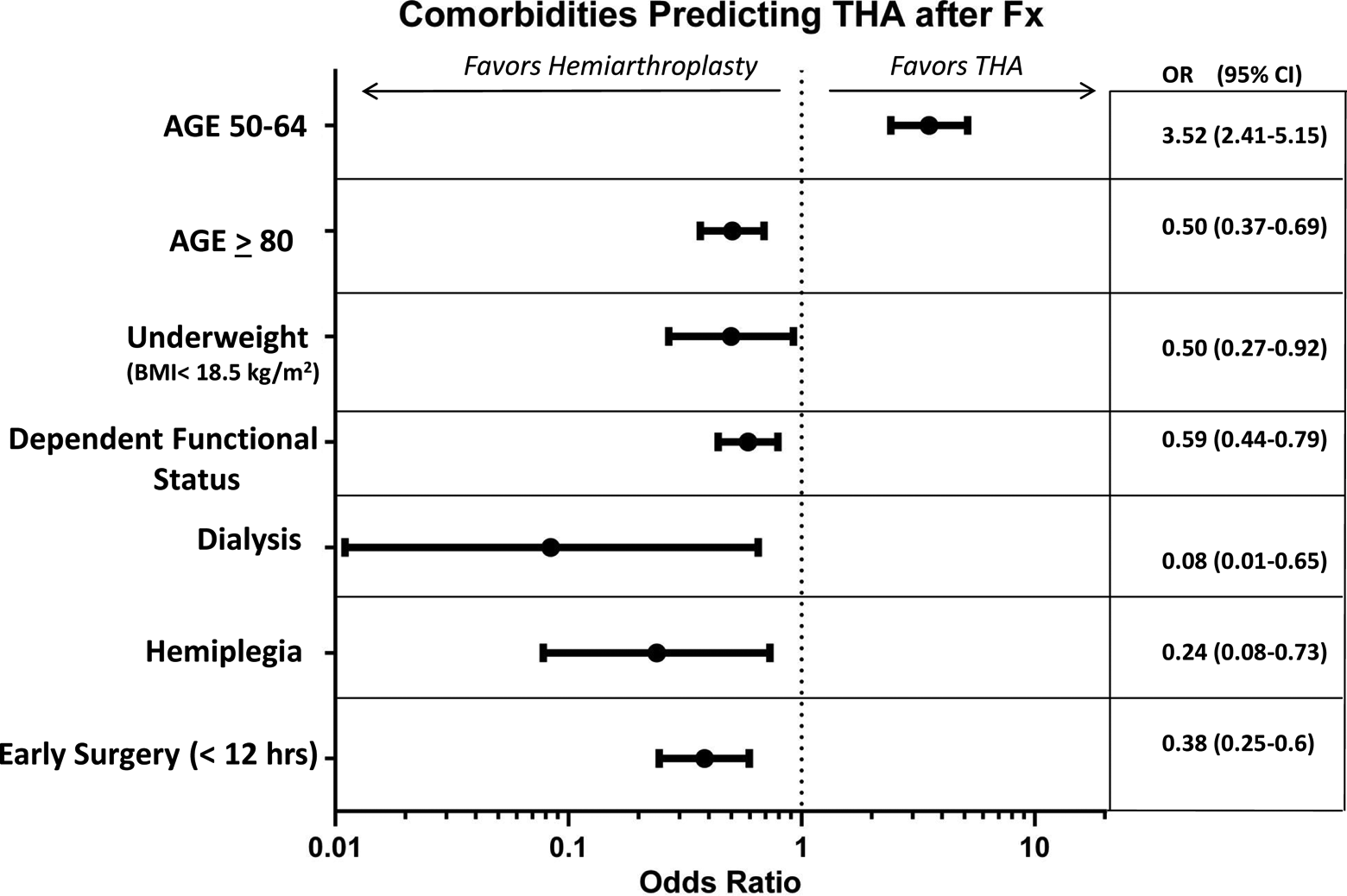
Multivariate regression for significant comorbidities predicting having a THA over a hemiarthroplasty after femoral neck fracture. The reference value (OR = 1) refers to having a THA. Ranges above OR = 1 favor THA. Ranges below OR = 1 favor hemiarthroplasty. OR indicates odds ratio.
Regarding complications after THA, only having disseminated cancer and diabetes were predictive of having a complication, whereas being overweight or obese I had a protective effect against having a complication as shown in Figure 2. Following hemiarthroplasty, only DNR status and being ASA classes 3 and 4 were predictive of having a complication as shown in Figure 3. Other variables such as gender, age, dependent functional status, dyspnea, preoperative sepsis, current pneumonia, preoperative blood transfusion, bleeding disorder, >10% weight loss in the last 6 months, or renal failure were not predictive of having a complication after either a hemiarthroplasty or a THA (data not illustrated).

Adjusted 30-day postoperative complications for patients undergoing THA (the x-axis is in logarithmic scale).
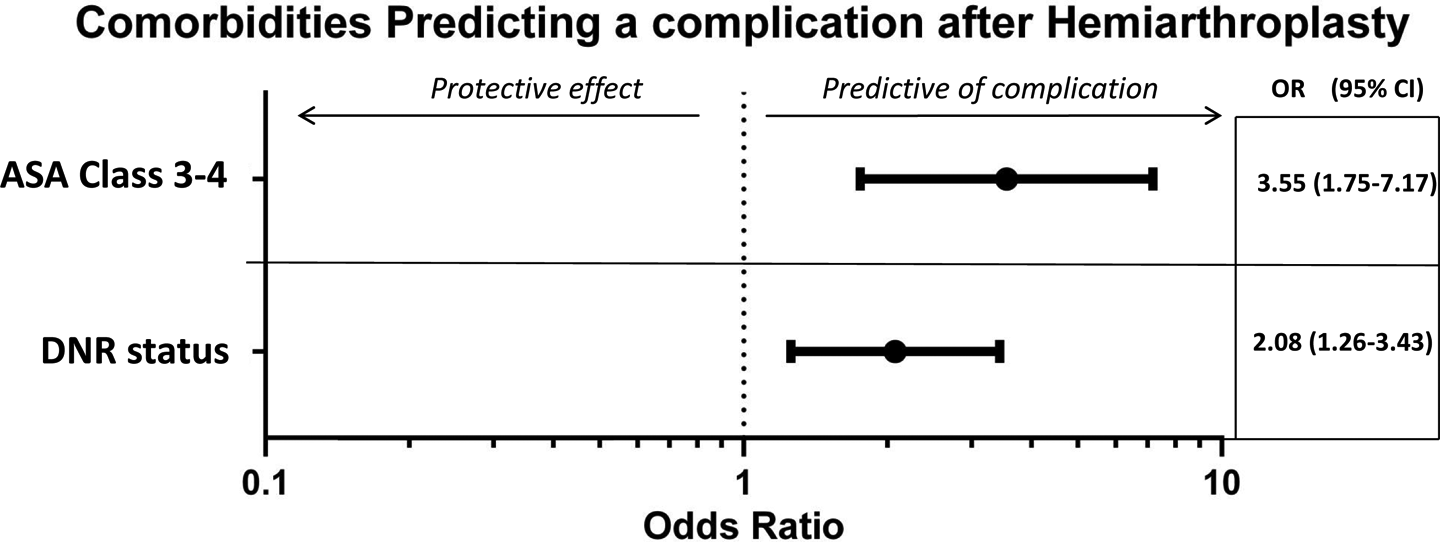
Adjusted 30-day postoperative complications for patients undergoing hemiarthroplasty.
Discussion
Hip fractures are common problems that are already challenging the medical system as the population ages. 1 –4,24 These fractures come in many varieties and levels of complexity but one of the most common types is a displaced femoral neck fracture. Recently, a number of studies have shown that THA has improved outcomes over hemiarthroplasty.11 –19 The goal of this study was not to demonstrate the superiority of total hip replacement but to identify which preoperative factors may be associated with the decision to perform THA versus hemiarthroplasty and to compare the complications associated with each.
Using the multivariate model, we identified 6 factors associated with the decision to perform THA or a hemiarthroplasty including age, BMI, functional status, dialysis, hemiplegia, and early surgery (Figure 1). These comorbidities reflect a more medically complex patient pool. A large number of patients who have a femoral neck fracture are elderly patients with significant comorbidities who are not physically active. As such, a hemiarthroplasty will likely work well and the proposed increase in function associated with a THA may not be realized by many of these patients. Also of consideration when deciding between hemiarthroplasty and THA is the high mortality rate within 1 year of hip fracture, the increased rates of dislocation after a total hip, and the cost of the prostheses. 2 –4,8,11 –14,17 –19 In patients who are at high risk of subsequent falls, a hemiarthroplasty may be the superior choice as it is more reproducibly stable and easier to perform by most orthopedic surgeons.
Lowe et al 25 published a review of the literature on the treatment of hip fractures and they make a strong case for treating patients based on “physiologic age.” They reason that physiologically younger patients are more fit and have a better expectation to return to their prefracture activities than older, more debilitated patients. As such, a total hip replacement would be an ideal treatment for younger, healthier patients. This concept is reflected in our data as well since it seems clear that the surgeons in this study were preferentially choosing patients who were younger and healthier to receive total hip replacements. (Figure 1)
With regard to complications, we did not find any significant difference in the rates of thromboembolic complications, respiratory complications, and infections as shown in Table 3 (P > .05 for all). Also, there were no significant differences between the 30-day mortality rates (5.6% vs 3.1%) for THA versus hemiarthroplasty, respectively (P = .063). There was increased utilization of blood transfusion in patients who had a total hip replacement, 22.7%, versus 14.4% for hemiarthroplasty. This likely represents increased blood loss associated with preparing the acetabulum during THA.
Although the blood transfusion requirements were higher in the THA cohort, a secondary analysis of our data did not demonstrate an increased risk of postoperative infection. This was in contrast to the higher rates of infection that has been documented in the literature for patients who receive a blood transfusion. 26 In our study, the rate of postoperative septic complications in the group of patients who received blood was 2.5% (22 of 994 total nontransfused patients) compared to 3.8% (8 of 208 total transfused patients; P = .523).
Since there was no significant increase in complications resulting from blood transfusions, we elected to exclude blood transfusions from the final analysis when grouping all complications together. However, we certainly acknowledge that there are well-documented risks of blood transfusions other than infection, such as transfusion-related reactions, fluid overload, and prolonged hospitalizations. 26 We believe that all measures should be taken to decrease the need for blood transfusion.
When all complications are considered together, excluding blood transfusion, we found that patients who received a hemiarthroplasty had an 18.9% chance of having one or more complications compared to 13.6% for patients receiving THA (P = .020). This represents an aggregate of all possible recorded complications ranging from postoperative mortality, pneumonia, infections, mortality, renal failure, and so on (Table 3) Since older, sicker patients preferentially underwent hemiarthroplasty, it follows that these same patients would be at higher risk of postoperative complications. It has been shown previously that patients with higher ASA scores and with advanced age and greater comorbidities have higher rates of early postoperative complications following orthopedic surgery. 27 –29 Furthermore, our study showed that hemiarthroplasty patients stayed, on average 1.55 days, longer in the hospital than THA patients, which is also consistent with THA patients being healthier and having less complications perioperatively.
The current study describes the preoperative patient factors associated with receiving a hemiarthroplasty versus a THA after a femoral neck fracture as well as the 30-day complication rates after these procedures. We identified a number of conditions that were significantly associated with decision to perform total hip replacement versus hemiarthroplasty. In general, patients who have more medical comorbidities and are less functionally independent are being treated with hemiarthroplasty. However, it is likely that a large number of patients who would be good candidates for THA are not being treated as such. As shown in Table 1, there was a substantial number of patients between the age of 50 and 64 (8% of hemiarthroplasty patients) as well as a large number of healthy patients as judged by their ASA score (17.2% with ASA score of 1 or 2) who underwent hemiarthroplasty instead of THA.
The above-mentioned factors suggest that some patients who might benefit from a THA are not receiving one. There are a number of factors beyond what is presented in this study such as surgeon availability that undoubtedly affect clinical decision making, but it is interesting to note that only 7.2% of patients had a THA performed within 12 hours of admission as compared to 21.6% of patients who underwent a hemiarthroplasty (P < .001, Table 1). This was statistically significant in our multivariate analysis as patients undergoing early surgery were less likely to have a THA (OR [95% CI]: 0.38 [0.25-0.6]). These data could be explained if surgeons identify patients who would benefit from THA and delaying the surgery so that the patient can either be transferred to the care of a surgeon who regularly performs THA or postponed to a time when the primary surgeon is better prepared for a more complex surgery.
Some of the clinically applicable results from this study are the risk factors identified for complications after THA and hemiarthroplasty (Figures 2 and 3). Identifying high-risk patients allows for early aggressive management directed toward preventing adverse outcomes. Following THA, patients with diabetes or disseminated cancer are at a higher risk of having a complication. Similarly, after hemiarthroplasty, patients with high ASA scores (ASA 3 and 4) or who are deemed DNR preoperatively are at high risk of developing complications. Therefore, physicians can identify these patients early in their clinical course and take care to carefully monitor and manage these delicate patients with multiple systemic comorbidities.
An interesting finding noted in our study is that overweight and obesity class I patients are relatively protected against early complications after THA. These findings are contributory to the recent findings in the literature which have shown that there appears to be a lower all-cause mortality for patients who are overweight and that obesity class I (BMI 30-34.9) may not associated with higher all-cause mortality compared to normal weight patients. 30
There are a number of limitations to this study. Most obvious is that it is a review based on data from a national patient database. We did not have additional records to review nor could we speak with patients to determine what complications they might have had beyond 30 days after surgery. Other limitations of our study are that the ACS NSQIP does not report on surgeon volume, academic status of hospitals, insurance type of patients, income group of patients, total in-hospital costs, or hospital readmissions. The ACS NSQIP data set also does not capture disease- and operation-specific variables; therefore, we could not evaluate other hip arthroplasty-specific complications such as dislocation, fracture, and early revision, among others. The advantage of ACS NSQIP is that it provides detailed clinical information on many patients and encompasses academic and nonacademic hospitals, thus allowing for analysis of a broad cross-section of the population.
This study supports the notion that patients who are younger, healthier, and functionally independent are best served by receiving a THA in favor of a hemiarthroplasty, even if this means delaying treatment in order to transfer care to a time when or to a surgeon who can perform the necessary procedure safely. As mentioned earlier, the data point to the fact that there are likely a number of patients who should be receiving a THA who are not being given the opportunity. In the appropriately chosen patient, THA is a safe and effective surgery that is not associated with increased postoperative complications. We identified 2 comorbid conditions (diabetes and disseminated cancer) as having a higher risk of developing a postoperative complication following THA. Similarly following hemiarthroplasty, patients with high ASA class and DNR status had increased rates of complications. These therefore are conditions that if present could be potential targets for aggressive perioperative management in order to decrease the risk of poor outcomes.
In summary, we have presented data evaluating how patients’ preoperative conditions are associated with management of femoral neck fractures as well as factors associated with morbidity after the surgery. One avenue that is currently being explored to decrease the morbidity is utilizing a medical comanagement system to help care for patients with medically complex hip fracture. This has been reported to dramatically reduce costs and improve outcomes for these patients. 31 We hope that the results from the current study will help further improve outcomes for these increasingly complex patients.
Footnotes
Authors’ Note
The article was prepared for submission to the Geriatric Orthopaedic Surgery & Rehabilitation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.