
Abstract
Background:
The purpose of the present study is to use a statewide, population-based data set to identify mortality rates at 30-day and 1-year postoperatively following total hip arthroplasty (THA) and hemiarthroplasty (HA) for displaced femoral neck fractures. The secondary aim of the study is to determine whether arthroplasty volume confers a protective effect on the mortality rate following femoral neck fracture treatment.
Methods:
New York’s Statewide Planning and Research Cooperative System was used to identify 45 749 patients older than 60 years of age with a discharge diagnosis of femoral neck fracture undergoing THA or HA from 2000 through 2010. Comorbidities were identified using the Charlson comorbidity index. Mortality risk was modeled using Cox proportional hazards models while controlling for demographic and comorbid characteristics. High-volume THA centers were defined as those in the top quartile of arthroplasty volume, while low-volume centers were defined as the bottom quartile.
Results:
Patients undergoing THA for femoral neck fracture rather than HA were younger (79 vs 83 years, P < .001), more likely to have rheumatoid disease, and less likely to have heart disease, dementia, cancer, or diabetes (all P < .05). Thirty-day mortality after HA was higher (8.4% vs 5.7%; P < .001) as was 1-year mortality (25.9% vs 17.8%; P < .001). After controlling for age, gender, ethnicity, and comorbidities, risk of mortality following THA was 21% lower (hazard ratio [HR] 0.79; P = .003) at 30 days and 22% lower (HR 0.78; P < .001) at 1 year than HA. Patients undergoing THA at high-volume arthroplasty centers had improved 1-year mortality when compared to those undergoing THA at low-volume hospitals (HR 0.55; P = .008).
Conclusions:
Based on this large, population-based study, there is no basis to assume THA carries a greater mortality risk after hip fracture than does standard HA, even when accounting for institutional volume of hip arthroplasty.
Keywords
Introduction
Femoral neck fractures represent an increasingly common diagnosis in the geriatric population associated with high morbidity and mortality. The worldwide incidence of hip fractures is expected to approach 6.26 million by 2050. 1 Furthermore, the 30-day mortality rate in the geriatric population after femoral neck fracture is reported as high as 9.6%, while the 1-year mortality rate increases to 33%. 2 Displaced femoral neck fractures in elderly patients are typically treated with hemiarthroplasty (HA) or total hip arthroplasty (THA). Hemiarthroplasty is the most common procedure performed in the geriatric population 3 ; however, rates of THA are increasing for femoral neck fractures in the active elderly patients. 4 The optimal treatment choice for displaced femoral neck fractures remains controversial.
Several randomized controlled trials have demonstrated improved functional outcome scores 5 –10 and decreased pain 5,11,12 for THA after femoral neck fracture when compared to HA. Despite purported benefits of THA, there are inherent risks associated with longer operative time and greater blood loss than HA. 9,10,13 The reported rates of postoperative dislocation are also greater when THA is used in the setting of femoral neck fracture when compared to HA. 13 –15
Decreased pain and increased function may matter little if the increased operative time and complications such as dislocation lead to increased patient mortality. Small differences in mortality may be missed by small, randomized controlled trials, which are often performed at specialty centers with high volumes of THA. As such, the importance of expertise with THA in contributing to any mortality benefit is critical in the decision to recommend THA or HA as first-line treatment for femoral neck fracture management. Population-based study of patient mortality allows critical evaluation of the role played by institutional surgical volume and experience with both THA in general and THA specifically for femoral neck fracture.
The purpose of the present study is to compare the outcomes of femoral neck fractures in patients ≥60 years of age treated with HA or THA using population-based data from the New York Statewide Planning and Research Cooperative System (SPARCS). The hospital demographic information obtained from this data set allows for a comparison between high and low-volume arthroplasty hospitals with respect to complications and mortality statistics. The author’s anecdotal experience has demonstrated an increased survivorship with THA for femoral neck fracture treatment, despite the increased technical demand over HA. We hypothesized a lower 30-day and 1-year mortality rate when patients are treated with THA versus HA and that this mortality benefit would remain significant after controlling for institutional volume of THA. In addition, we hypothesize that hospitals where THA is performed most commonly for femoral neck fracture will have lower mortality rates than centers with low-volume THA for fracture.
Methods
The New York Department of Health SPARCS provided data for this study. The SPARCS is an administrative database established in 1979 which collects patient-level data from all nonfederal acute care facilities in the State of New York and contains information on patient demographics, diagnoses, treatments, and charges for every hospital discharge, ambulatory surgical procedure, and emergency department admission. Estimated reporting completeness obtained from SPARCS annual reports from 2000 to 2010 ranged from 95% to 100% with an average of 98.7% completeness. 16 Mortality data were obtained through SPARCS linkage with the New York State Department of Health, Office of Vital Records, and New York City Department of Health and Mental Hygiene.
Using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis and ICD-9 procedural codes, we identified 45 919 records in patients ≥60 years of age with inpatient hospital admissions from 2000 through 2010 with a diagnosis code for femoral neck fracture (821.0-821.09) who underwent treatment with either THA (procedure code 81.51) or HA (procedure code 81.52). Follow-up cutoff date was December 31, 2011. The analysis included 212 hospitals in the State of New York where operative fixation of femoral neck fractures took place. One hundred and seventy records were excluded due to missing procedure dates for THA or HA. During the study period, there were 707 patients with multiple hospital admissions meeting inclusion criteria. These were treated as independent events, leaving 45 749 records in the study.
Comorbid conditions, using the method reported by Charlson et al, were assigned with use of a STATA interpretation of SAS software program obtained from the Boston College Department of Economics in its series Statistical Software Components. 17 –19
Study Comparison Groups
The 2 primary comparison groups in the study are THA for femoral neck fracture and HA for femoral neck fracture. Mortality rate analysis was conducted for these 2 groups at 30-day and 1-year postoperative time periods. This analysis was repeated after controlling for age, race, and comorbid conditions using the Charlson comorbidity index.
The data were also analyzed to investigate the relationship between mortality after femoral neck fracture and experience with THA performed for any indication (all-cause arthroplasty). The top and bottom quartile hospitals were identified based on the number of THA cases performed for any indication during the study period. The top quartile was defined as high volume, and the bottom quartile was defined as low volume. Several analyses were then performed: (1) mortality after THA for fracture was compared at hospitals within the top and bottom quartiles of all-cause arthroplasty (not just for fracture), (2) mortality after THA was compared to HA for femoral neck fractures within the top quartile of all-cause arthroplasty hospitals, and (3) mortality after THA was compared to HA for femoral neck fractures within the bottom quartile of all-cause arthroplasty hospitals.
A final analysis was designed to determine the relationship between mortality and hospital expertise at using THA exclusively for femoral fracture. The top and bottom quartile hospitals were identified by the number of THA cases for femoral neck fracture performed during the study period. Mortality after THA for femoral neck fractures at the top quartile hospitals was compared to mortality after THA for femoral neck fractures at the bottom quartile hospitals.
Statistical Methods
Univariate analyses on categorical and continuous parameters were performed using chi-square and Student t tests, respectively. Time to mortality was modeled using the Kaplan-Meier method, with the log-rank test. Proportional hazard regression was used to quantify 30-day and 1-year mortality risk with THA in comparison to HA, while adjusting for covariates that were significantly associated with mortality on univariate analysis (P < .05). All analyses were performed with use of a Stata statistical software (version 13.1 StataCorp, College Station, Texas).
Results
Patients with femoral neck fracture undergoing THA compared with HA were, on average, younger (79 vs 83 years, P < .001), more likely to be white (87% vs 85%, P < .001), and were less likely to have an acute myocardial infarction (7% vs 9%; P < .001), congestive heart failure (13% vs 16%; P < .001), dementia (4% vs 6%; P < .001), diabetes (15% vs 17%; P = .001), cancer (2% vs 3%; P = .001), and more likely to have rheumatoid arthritis (4% vs 3%; P < .001). Patients receiving THA had slightly fewer comorbid conditions (mean 0.9 vs 1.1, P < .001). There was no significant difference in gender or time to fixation between patients receiving THA and HA for femoral neck fracture (Table 1). Billed hospital costs were higher for THA than for HA (US$42 279 vs US$38 517; P < .001).
Patient Sample Demographics.a,b

Abbreviations: HA, hemiarthroplasty; THA, total hip arthroplasty; MI, myocardial Infarction; CHF, congestive heart failure; PVD, peripheral vascular disease; COPD, chronic obstructive pulmonary disease.
aSignificant P values appear in bold (P ≤ .001).
bPatients were significantly younger and healthier as determined by Charlson comorbidity index in the total hip arthroplasty cohort. There was a significantly lower mortality rate at 30 days and 1 year in the total hip arthroplasty cohort as compared to hemiarthroplasty.
Without controlling for comorbid conditions, THA had reduced 30-day mortality (5.7% vs 8.4%; P < .001) and reduced 1-year mortality (17.8% vs 25.9%; P < .001). After controlling for age, gender, and comorbid conditions, there was a 21% reduced mortality risk at 30 days postoperatively (hazard ratio [HR] 0.79; P = .003) which persisted at 1 year (HR 0.78; P < .001; Figure 1). The mortality benefit from THA compared with HA, as demonstrated on Kaplan-Meier survival curve, began early and remained favorable throughout the first postoperative year (Figure 2).

Graphical representation of hazard ratios of factors influencing risk of 1-year mortality after femoral neck fracture with 95% confidence intervals.
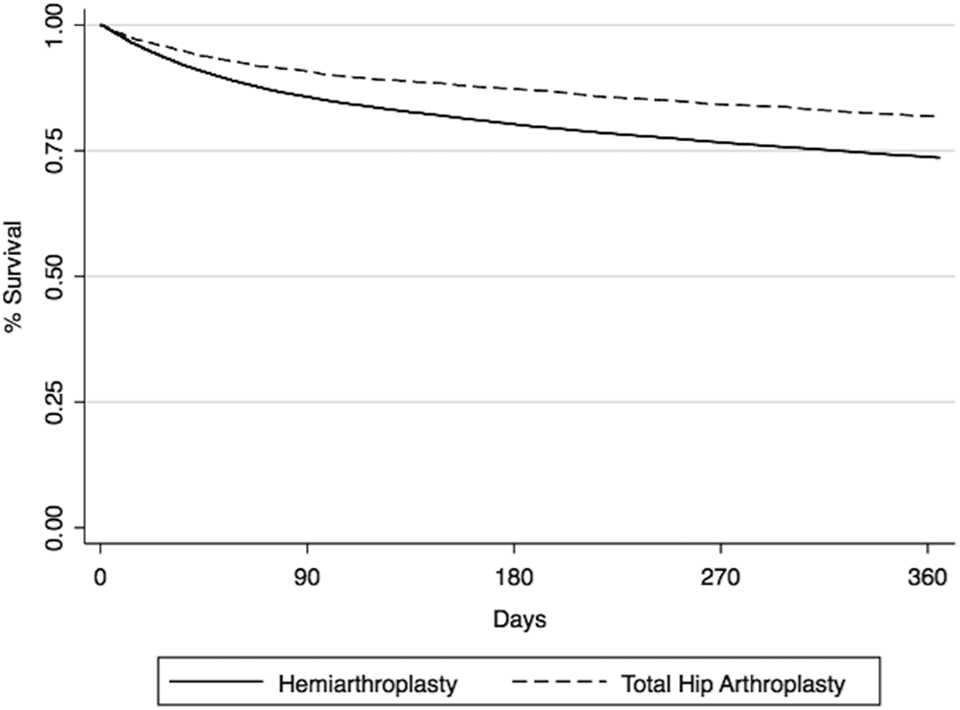
Survival after total hip arthroplasty and hemiarthroplasty for femoral neck fracture.
Does the All-Cause Arthroplasty Volume at a Hospital Affect Mortality Outcomes?
Hospital experience with the THA procedure done for any reason (all-cause arthroplasty) may affect mortality outcomes. To test the association between hospital experience with THA done for any reason and mortality, hospitals were stratified by volume of all-cause arthroplasty. high-volume all-cause arthroplasty hospitals (top quartile) were compared to those with the least experience (bottom quartile). In this analysis, THA was associated with decreased mortality when performed at high-volume all-cause THA hospitals compared with low-volume arthroplasty hospitals (HR 0.55; P = .008; Table 2).
Comparison of Hospital Volume and Femoral Neck Fracture Mortality.a,b

Abbreviations: CI, confidence interval; HA, hemiarthroplasty; THA, total hip arthroplasty.
aSignificant P values appear in bold (P ≤ .001).
bHazard ratios presented at 95% confidence level.
Does the Mortality Difference Between THA and HA for Femoral Neck Fracture Depend on All-Cause Arthroplasty Volume?
To assess whether differences in mortality between THA and HA were related to hospital experience with THA, we compared mortality after each procedure in high and low-volume centers. At hospitals in the top quartile of all-cause arthroplasty experience, patients whose fracture was treated with THA had half the mortality of patients treated with HA even after controlling for demographics and comorbid conditions (HR 0.50; P = .001). Strikingly, low-volume all-cause arthroplasty centers also have significantly reduced mortality for THA as compared to HA, although the benefit is slightly muted (HR 0.76; P < .001; Table 2).
Does Hospital Experience With THA for Fracture Affect Mortality Rate?
Finally, we attempted to compare the mortality in hospitals where THA is often performed, specifically for femoral neck fracture to those where this procedure is rare. When hospitals were divided into quartiles based on the number of times THA was employed specifically for femoral neck fracture, no significant association with mortality could be found. Hospitals performing high volumes of THA for femoral neck fracture compared with low volumes of THA for femoral neck fractures had similar mortality outcomes (HR 1.02; P = .87; Table 2).
Discussion
The present study demonstrates a significantly reduced mortality rate for patients greater than 60 years of age undergoing THA as compared to HA for femoral neck fractures. These findings are supported by recent meta-analyses and systematic reviews of the literature demonstrating no increased mortality risk when THA is utilized for femoral neck fracture. 12,14,15 The present study builds upon these prior results while addressing the mortality risk with population level data. A similar study conducted by Soohoo et al using the data set provided by California’s Office of Statewide Health Planning and Development reported no significant difference in mortality at 90 days when comparing THA and HA. 20 The present study, using the SPARCS data set, marks the first instance of population level evidence, indicating a lower mortality rate with THA for femoral neck fractures as compared to HA.
These results do not indicate that treating a femoral neck fracture with a THA imparts a life-sustaining benefit on the patient. Lower mortality rate at both 30 days and 1-year postoperatively for THA compared to HA is likely due to a selection bias toward healthier individuals in the THA group. In the present study, we were able to control for medical comorbidities; however, we surmise that differences in patient health still exist between the groups. Use of the database allows for identification of comorbidities but does not indicate their severity. For example, there is a vast difference between a patient in remission from lung cancer and a patient who has diffuse metastases, yet both will carry an equally weighted diagnosis of cancer. We suspect that the decreased mortality in the THA cohort is the result of careful and appropriate avoidance of THA in unhealthy patients with femoral neck fracture.
The issue of mortality rate has also been addressed in current randomized, controlled trials evaluating THA and HA for femoral neck fractures. Avery et al reported 100-month follow-up on a total of 81 patients randomized to either THA or HA and noted a significantly greater mortality in the HA group. 11 Further randomized, controlled trials have noted no significant difference in 1-year mortality between THA and HA despite the inherent increased operative time and blood loss with THA. 8,10 Although the above studies are well designed, the small sample size limits their generalizability.
A further weakness of current randomized controlled trials comparing THA to HA is that the surgeries are presumably performed by high-volume surgeons, often arthroplasty fellowship trained at high-volume arthroplasty centers. Many instances in the orthopedic literature have highlighted the importance of surgeon and institution experience in the use of arthroplasty procedures. 21 –27 Primary hip arthroplasty literature has demonstrated reduced 6-month revision rates, 23 postoperative mortality, 21 and reduced hip dislocation when surgery is performed at high-volume centers. 24,25 In turn, clinical studies evaluating complications of arthroplasty for femoral neck fractures indicated higher primary and recurrent hip dislocation rates following THA as compared to HA. 28,29 This finding is likely due to the increased technical demands of THA, and any detrimental effects of procedural inexperience might be mitigated by high-volume arthroplasty hospitals.
High-volume geriatric fracture hospitals that utilize an orthopedics and internal medicine comanagement model have reported improved outcomes in elderly patients with femoral neck fractures. Data from these geriatric fracture specialty centers indicate shorter times to surgery and discharge, fewer cardiopulmonary complications, and reduced mortality rates. 30,31 With streamlined care and reduced medical complications, the organized fracture care model also represents an US$18 000 per patient savings as compared to US government reports. 32 Clearly, institutional expertise with both procedure and diagnosis could represent a confounding variable when comparing 2 surgical treatments. The benefit of population level data, as in the case of the SPARCS database, is that individual hospital volumes of surgery and femoral neck fracture care can be isolated and controlled, reducing the institutional bias.
In the present study, we hypothesized that improved mortality rates for THA rather than HA after femoral neck fracture would be independent of hospital arthroplasty experience; therefore, outcomes at high-volume and low-volume institutions were compared. We ranked hospitals based on their total annual volume of THA for all indications (fracture, degenerative joint disease, neoplasm, etc). The hospitals were then separated into top and bottom quartiles based on this ranking. At top quartile all-cause arthroplasty hospitals, THA for femoral neck fracture results in lower mortality risk as compared to the same procedure performed at bottom quartile all-cause arthroplasty hospitals. In a separate study using a similar SPARCS data set model, we demonstrated that increased hospital volume of THA for degenerative joint disease exerts a protective effect on mortality after THA for femoral neck fracture. 33 Both of these results indicate that procedural expertise is an important variable that needs to be controlled for when comparing mortality outcomes for femoral neck fracture treatment with THA or HA.
When THA was performed for a displaced femoral neck fracture at a high-volume all-cause arthroplasty center, there was a 50% reduction in mortality as compared to HA in the same hospitals. This result remained significant when mortality following THA and HA for displaced femoral neck fractures was compared at low-volume all-cause arthroplasty hospitals. This supports our hypothesis such that, regardless of hospital experience in arthroplasty, performing a total hip replacement for femoral neck fractures in the geriatric population does not incur increased mortality risk compared with HA. Inferring from the above analyses, THA for femoral neck fracture appears to be safe in both low-volume and high-volume centers but, with regard to mortality rate, is best performed at a center with extensive arthroplasty experience.
Considering the specific use of THA for the treatment of femoral neck fracture, the volume of such procedures performed did not make a significant difference in mortality between hospitals. Total hip arthroplasty for femoral neck fracture performed at a hospital with a high volume of such procedures conferred no mortality benefit over the same procedure performed at low-volume centers. This may indicate that the experience with THA for femoral neck fracture is not the most important factor, per se in determining post-operative mortality. Indeed, it appears as if experience with THA for any cause is more important than specific experience with THA for femoral neck fracture in determining mortality at any given hospital.
This study suffers from the limitations of a retrospective administrative data set. There may be inaccurate coding or failure to include all comorbidities present for a given patient. However, hospital coders are likely to include the comorbidities that would most likely increase acuity indices. Also, it is unclear exactly how the THA procedure itself confers a mortality benefit; anecdotal evidence indicates that THA is preferentially selected for high functioning patients. Therefore a bias toward healthier patients in the THA group could occur despite controlling for medical comorbidities. The nature of the data set does not include the ability to accurately determine prehospital functional status.
Mortality in the database is only recorded within the borders of New York State, which may potentially skew the results with patients who receive surgery inside and then expire outside the state. However, the large total patient population in the present study would likely make any effect negligible.
The results of this study demonstrate significantly improved 30-day and 1-year mortality rates when geriatric femoral neck fractures are treated with THA when compared to traditional HA. The reduced mortality risk in the THA cohort remains constant even when controlling for age, race, and comorbid conditions. Furthermore, there was a significantly improved 1-year mortality for patients undergoing THA rather than HA, regardless of hospital experience with arthroplasty. However, THA for femoral neck fracture resulted in fewer mortality events when performed at high-volume arthroplasty hospitals—those hospitals where the procedure is performed more often for any cause. In addition, we noted a reduced mortality rate when THA for femoral neck fracture is performed at hospitals with the greatest average volume of THA for all causes as compared to low-volume THA hospitals. Further research could elucidate whether other common complications of THA such as infection and hip dislocation are also affected by hospital arthroplasty volume. Based on this large, population level study, there is no basis to assume THA carries a greater mortality risk after hip fracture than standard HA, even when accounting for the volume of arthroplasty performed at an institution. Moreover, careful patient selection is paramount to maintaining a low mortality rate following THA for femoral neck fracture.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.