
Abstract
Keywords
Introduction
Multilevel cervical spondylotic myelopathy (MCSM, involving three or more) is a cervical disease caused by joint degeneration and hypertrophy, ligamentum flavum calcification and hypertrophy, and spinal cord compression. The selection of surgical approach for MCSM is still controversial. The traditional views claim that posterior surgery is relative safe and has satisfactory outcome, but involves some complications such as axial pain, nerve root palsy, and poor recovery of cervical lordosis. Anterior cervical discectomy can directly remove the compression material and restore cervical lordosis; however, it is more likely to cause dysphagia and hoarseness due to long surgical time and retraction. 1 The use of the Zero-profile (Zero-p) interbody fusion cage can avoid the stimulation of the esophagus by the steel plate, reduce the traction of the esophagus and diminish the impact on adjacent segments, but it fails to improve the cervical lordosis and affects the postoperative clinical efficacy. 2 Moreover, the anterior decompression and hybrid reconstruction show promising safety and efficacy outcomes for the treatment of MCSM, with the advantages of short graft bone and segment plate.3,4 Therefore, we combined the advantages of the Zero-p self-locking fusion cage and the short-segment plate to develop anterior cervical discectomy and hybrid fusion (ACDHF). In this study, we enrolled patients with MCSM (three-level) admitted from January 2013 to June 2017 and treated them with ACDHF and traditional anterior cervical discectomy and fusion (ACDF) to compare the clinical efficacy on the treatment for MCSM.
Materials and methods
General information
Comparison of general information between two groups.

Note: a indicates that the number is X2 value; p < 0.05 indicates significance.
Surgical procedure
The surgery was performed by the same spine surgeons with more than 20 years of surgical experience. Multiple cervical spondylosis was treated with the same set of retractors and titanium alloy plate of the same thickness. Under general anesthesia through tracheal intubation, patients were placed in the supine position. A incision (4–5 cm) was made below the sternocleidomastoid muscle on the right side. The subcutaneous tissue was separated from platysma. After making a longitudinal incision of the platysma, the deep fascia tissue was loosened, and the visceral sheath was exposed. The anterior fascia and anterior fascia were cut to expose the surgical disc space, and then the disc space was enlarged with a Casper distractor through a fluoroscopic positioning needle to completely remove the annulus fibrosus and nucleus pulposus. The endplate cartilage was curetted until bleeding, and the posterior longitudinal ligament was removed by decompression using clenching forceps and curettes. In the hybrid group, a self-locking cage was placed in the most inferior disc space, and a cage filled with cancellous allograft bone was inserted in the disc space. Rongeurs were used to treat the hyperplasia of the anterior edge of the vertebral body. The cervical short-segment plate was fixed to the vertebral body against the side of the self-locking cage. After fixing the screw, the wound was washed and stanched, followed by suture, and tube drainage. In the control group, cages filled with allogenic cancellous bone were inserted into three prepared disc spaces and rongeurs were applied to remove the anterior vertebral hyperplasia. Anterior cervical long-segment plate were fixed on the vertebral body. After the position was confirmed by fluoroscopy, the screw was fixed and the wound was washed and stanched, followed by suture, and tube drainage (Figures 1 and 2). A 62-year-old male patient with MCSM. (A) Preoperative lateral X-ray indicated intervertebral space narrowing, osteophyte formation from C2-C6. (B) Preoperative MRI showed spinal cord compression of C3-6. (C) X-rays after 5 days of ACDHF showed good positioning of the self-locking retainer and the shorter segmental plate. (D) Postoperative MRI showed good decompression of spinal cord. Note: MRI: Magnetic resonance imaging. A 64-year-old male patient with MCSM. (A) Preoperative lateral X-ray indicated intervertebral space osteophyte formation from C3-C6. (B) Preoperative MRI showed spinal cord compression of C3∼6. (C) Postoperative X-ray at 1 week showed that cage and long segmental plate located well. (D) Postoperative MRI showed good decompression of spinal cord with strip edema. Note: MRI: Magnetic resonance imaging.

Postoperative treatment
With a tracheostomy kit prepared at the point-care site after the operation, patients were received antibiotics for 24 h and hormones and neurotrophic therapy. The drainage tube was removed 48 h after surgery, and walking exercise under neck collar was allowed after the drainage tube was removed. The patients were discharged 5–7 days after surgery, followed up regularly at 1, 3, 6, and 12 months after surgery, and reexamined in the outpatient clinic every year.
Observation indicators
Data collected were postoperative drainage, blood loss, operation time and hospital stay. The 1956 Japanese Orthopaedic Association (JOA) score was used to assess the status of spinal cord nerve function and the visual analogue scale (VAS) was conducted to evaluate the improvement of postoperative neck and shoulder pain. The intersection of the perpendicular lines of the C2 and C7 extension lines was taken to determine the cervical curvature. The bone graft fusion was evaluated based on the Koller method. 5 Dynamic X-ray indicated no movement between the fusion spinous processes, no translucent line at the interface, and bridging bone at the bone graft site. Three-dimensional reconstruction of the cervical spine was performed when necessary to fuse the vertebral endplates or between the grafted areas. The condition of postoperative dysphagia was evaluated using the Bazaz scoring. 6 We also observed the complications such as hoarseness and cerebrospinal fluid leakage.
Evaluation of curative effect
We evaluated neck, shoulder, and limb pain preoperatively, at 5 days, 3 months, and 6 months postoperatively, as well as neurological status at last follow-up using the pain VAS. The JOA score was applied to evaluate the neurological status preoperatively, at 5 days, 3 months, 6 months, and last follow-up postoperatively. The physiological curvature of the cervical spine was also measured. Moreover, the Bazaz score was used to evaluate the degree of postoperative dysphagia.
Statistical analysis
Data were analyzed using the SPSS 21.0 software. All continuous data meet the normal distribution were presented as mean ± SD. For continuous data, difference between groups was analyzed by independent t test (2 groups) or repeated- measures analysis of variance (RM-ANOVA). The analysis of count data was performed by χ2 test. p < 0.05 refers to significant difference.
Results
The basic situation of the operation
Basic information of patients in the two groups during perioperative period (Mean ± SD).

Clinical efficacy
Comparison of the JOA, VAS and Curvature of the cervical spine in hybrid group and control group (Mean ± SD).

Imaging evaluation
During the follow-up period of all patients, X-rays confirmed the safety and effectiveness of the that internal fixation of plates. Long-segment plate fixation of the intervertebral space reached the fusion standard 6 months after the operation in 28 cases of control group, and the other 2 cases reached the standard 12 months after the operation. In the hybrid group, the self-locking fusion cage was partially sunk without displacement 3 months after the operation in 2 cases, and the rest of the intervertebral space was in good position. All cases achieved bone fusion within 6 months, without internal fixation-related complications such as internal fixation plate fracture or screw loosening. Still, the difference in the curvature of the cervical spine between two groups was less significant (p = 0.549, Table 3).
Postoperative complications
Comparison of the dysphagia in hybrid group and control group after surgery (n).
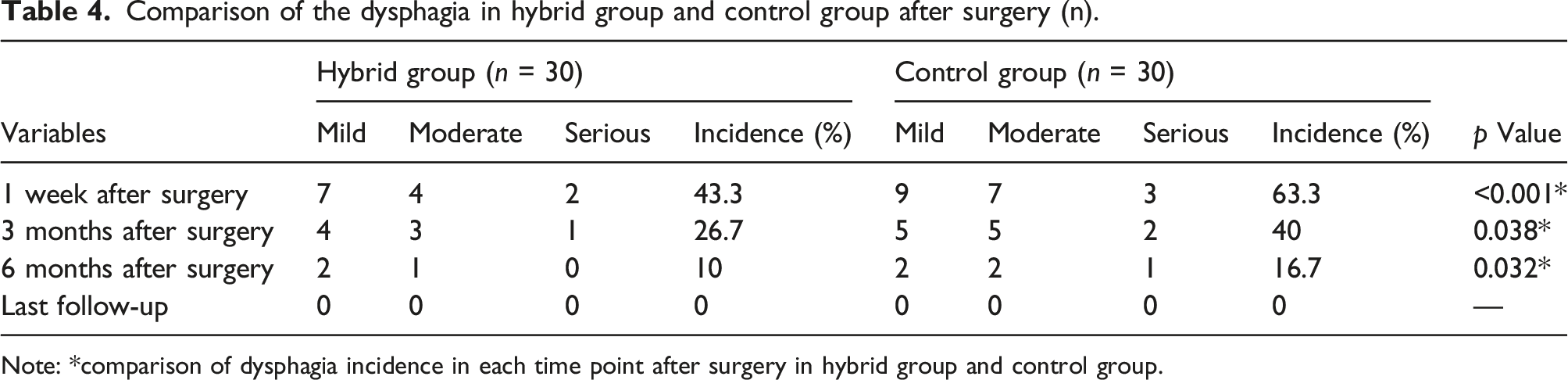
Note: *comparison of dysphagia incidence in each time point after surgery in hybrid group and control group.
Discussion
Our study found that both approaches significantly improved the JOA scores, VASNP scores and the cervical lordosis (p < 0.05), with no significant difference between the two approaches (p > 0.05). ACDHF could achieve similar clinical effects as ACDF. The key to achieve satisfactory clinical results is that the precise surgical technique during surgery can ensure the complete removal of osteophytes of the endplate cartilage, adequate preparation of the endplate bone graft bed at both ends, and appropriate selection of cages that meet the shape of the upper and lower endplates. Also, the application of self-locking independent fusion cage can ensure the decompression and fixation effect. 7 The common causes of dysphagia in anterior cervical surgery are varied, but generally can be divided into two categories 8 : (1) Patient factors: age, gender, and weight; (2) Physician factors: surgical section, operation time, steel plate length and thickness, use of zero-profile hybrid fusion, and use of special retractors. Moreover. Since cervical lordosis maintenance is related to various factors such as implant size, location, contact area, and intraoperative distraction height. More clinical observations are needed to assess the effectiveness of two methods for maintaining postoperative cervical lordosis.
The rate of dysphagia in the hybrid group within 6 months after surgery was significantly lower than that of the control group (p < 0.05). In spite of no significant difference in dysphagia and other complications at the last follow-up (p > 0.05), early dysphagia may be related to the short segmental plate and self- locking stand-alone cages. These applications do not treat all prevertebral osteophytes, and the insertion of a plate can save time for pulling the surrounding tissue. Besides, when multiple cervical spondylosis involves the 6–7 intervertebral spaces of the cervical spine, the application of self-locking stand-alone cages can avoid the difficulty of pre-bending the plate, shorten the operation time, reduce the time of pulling esophagus, postoperative bleeding and esophageal adhesions. Moreover, late dysphagia may be related to plate thickness. We observed resolution of dysphagia at the last follow-up in both groups, which was related to the selection of the plate with the same thickness in our study.
We also found that compared with ACDF, ACDHF obtained a shorter operation time, less intraoperative blood loss and postoperative drainage. This is because (1) the application of ACDHF with short segmental plate does not need to deal with the prevertebral osteophytes too much in the intervertebral space where the self-locking stand-alone cages is located; (2) it is easier to fix the short segmental plate; (3) the application of self-locking stand-alone cages can avoid the difficulty of pre-bending the plate, shorten the operation time, reduce intraoperative bleeding and postoperative drainage. Moreover, in the same field of view, the use of short segmental plate in ACDHF can be close to the self-locking stand-alone cages and far away from the upper intervertebral disc, which can avoid the stimulation of the proximal and distal intervertebral discs, especially the stimulation that is more likely to occur in the upper intervertebral space. 9 Further, the use of short segmental plate can reduce the angle between the plate and the sagittal line of the cervical spine, so that the plate can be fixed more firmly. 10 The use of long segmental plates in ACDF is difficult to take into account both upper and lower non-surgical intervertebral discs at the same time 11 and difficult to ensure that both ends of the steel plate are more than 5 mm away from the intervertebral disc.
This study has several limitations. First, this study contains limited sample size, which may affect the results of the study due to individual differences in cases; Second, postoperative complications like fusion rate may be underestimated due to technical problems; Third, the Bazaz score of dysphagia in the selected cases in this study mainly obtained by subjective perception, which may cause error due to inaccurate case description; Fourth, the follow-up time is not long enough in this study, which is needed to clarify the therapeutic effect of the ACDHF technique.
In conclusion, our research demonstrates that both ACDHF and ACDF can achieve satisfactory clinical results, but the ACDHF can reduce intraoperative injuries and postoperative dysphagia, making it as an optional approach for the treatment of MSCM.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:This study was supported by the Public welfare application research project of Huzhou science and Technology Bureau (No. 2017GY35).