
Abstract
Introduction
The timing of tranexamic acid (TXA) administration in fragility hip fracture patients is controversial. Prior studies have demonstrated reduction in transfusion requirements using the two-dose arthroplasty model. However, unlike arthroplasty patients whose bleeding starts at the time of surgical incision, hip fractures have an onset of bleeding at the time of the injury. The primary goal of this study was to evaluate the optimal timing of TXA administration and to determine its effect on red blood cell transfusions in fragility hip fracture patients.
Methods
All patients admitted to the fragility hip fracture service from April 1, 2019 to September 30, 2019 were prospectively screened for inclusion in the study. Eligible patients received 4 intravenous doses of TXA: Ineligible patients received no TXA. Patients with medical conditions precluding the use of TXA were deemed ineligible: allergy to TXA; creatinine clearance <30 mL/min; active malignancy; vascular event in the past year; anticoagulant use; fracture >48 hours prior to presentation. A subset of patients received only admission TXA dosing and a separate subset of patients received only incision and post op TXA dosing. Red blood cell transfusions, major adverse vascular events, and minor drug and infusion-related adverse events were recorded for all subgroups of patients.
Results
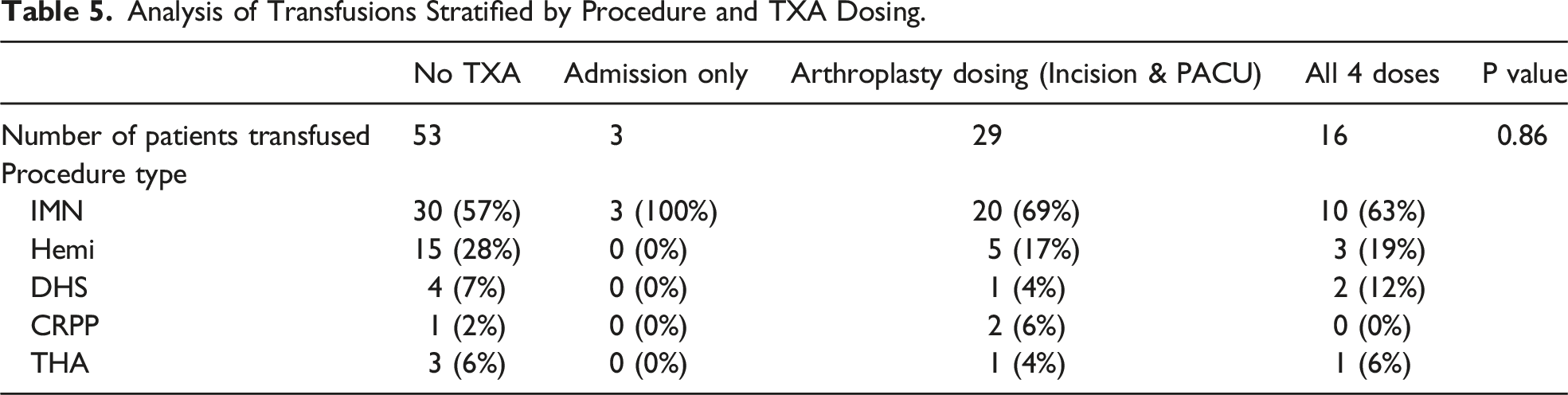
A total of 508 patients were eligible for analysis. In total, 180 patients received no TXA, 32 patients only received the admission doses of TXA, 112 patients received only the arthroplasty based (incision and post op) doses of TXA, and 183 patients received all 4 doses of TXA. The transfusion rate was significantly lower in patients who received all 4 doses of TXA (8.7%) and in those who only received one dose of TXA at admission (9.4%) compared to patients who received TXA at incision and recovery room (25.7%) or those patients who did not receive TXA prophylaxis (29.4%) (P = 0.001). Additionally, the transfusion rate for intramedullary nailing was higher compared to patients undergoing any other procedure (27% vs 13.8%, P < 0.001).
Conclusions
Patients with fragility hip fractures who received IV TXA at hospital admission have significantly lower transfusion rates compared to those who received no tranexamic acid or those who received two dose-TXA (at the operative incision and in the post-operative recovery room). These findings suggest that isolated dosing of TXA at hospital admission may be more effective at reducing post-operative bleeding than the traditional arthroplasty dosing (incision and post-op doses) and is equally as effective as the 4-dose TXA protocol in hip fracture patients undergoing surgery.
Introduction
The efficacy and safety profile of perioperative tranexamic acid (TXA) administration has been well established in trauma and elective total hip and knee arthroplasty.1-8 In these patients, prior studies have demonstrated a reduction in red blood cell transfusion requirements with perioperative TXA administration, independent of dosing, timing, type of anesthesia, and pre-operative hemoglobin levels.1-3,7,9 As allogenic blood transfusions have been associated with increased risks of transfusion reactions, length of hospital stay, infection transmission, and costs, recent clinical recommendations have endorsed the use of TXA in other areas orthopaedic surgery.1-3,9
In fragility hip fracture patients, the use of TXA to reduce blood loss and transfusion requirements has become an emerging area of research. Zhang et al. systematically reviewed 8 randomized controlled trials and reported an overall reduction in blood loss and transfusions without an increase in vascular thrombotic events (VTE) compared to controls undergoing hip fracture surgery. 10 Porter et al. showed that use of TXA was not associated with an increased risk of complications in high-risk patients undergoing arthroplasty for hip fracture. 11 Most of the current studies within the literature have utilized the TXA arthroplasty protocol for these patients, which typically involves one TXA dose at the time of surgical incision and a subsequent dose post-operatively.10,12 However, unlike arthroplasty patients whose bleeding starts at the time of surgical incision, hip fractures patients likely have differences in bleeding at the time of the injury. 13 As such, more clinical data is needed to examine early TXA administration and its effect on transfusion rates in patients with fragility hip fractures.
Currently, few studies have investigated TXA administration upon hospital admission for fragility hip fractures.1,13 Drawing from both the arthroplasty and trauma literature, a recent study conducted at our institution showed that a novel standardized hybrid TXA protocol of 4 doses, starting at the time of admission and continuing through the post-operative time period, significantly decreased transfusion rates in patients undergoing surgery for hip fragility fractures without an increase in the rate of adverse events. 1 However, the independent timing of these doses within the established hybrid model and its effect on decreasing transfusion rates has not been established.
The primary goal of this study was to evaluate the optimal timing of TXA administration and to determine its effect on red blood cell transfusions in fragility hip fracture patients. Due to the insidious onset of bleeding at the time of injury, we hypothesized that hip fracture patients who received TXA at hospital admission would have significantly lower blood transfusions rates compared to those who did not receive an initial TXA dose at admission. Such data has important clinical implications and can better define TXA guidelines for patients undergoing surgery for fragility hip fractures.
Materials and Methods
This study was considered to be a quality improvement project and therefore exempt from Institutional Review Board approval by Yale University and Yale New Haven Hospital guidelines. All patients admitted to the fragility hip fracture service from April 1, 2019 to July 31, 2020 were prospectively screened for inclusion in the study. Inclusion criteria included any fragility hip fracture admitted to the Yale New Haven Hospital St. Raphael Campus, the centralized campus of our fragility hip fracture service. The four intravenous (IV) doses of TXA regimen included: 1-gram over 10 minutes followed by infusion of 1 g over 8 hours upon admission to the inpatient unit, typically within 1 hour; 1 g administered at surgical incision followed by 1 g 3 hours later. Ineligible patients received no TXA. Exclusion criteria were determined by TXA contraindications in drug information literature. 1 In addition to patients with an allergy to TXA and impaired renal function, patients at highest risk of venous or arterial thrombotic disease were excluded. This category includes patients with a history of a vascular event within the last year or active malignancy. Patients on long term anticoagulation therapy were also considered to be in the high thrombosis risk category. Given these criteria, the following patients were excluded: allergy to TXA; creatinine clearance <30 mL/min.; active malignancy; vascular event in the past year (myocardial infarction, coronary stenting, stroke, peripheral vascular stenting, venous thromboembolism); anticoagulant use; and fracture >48 hours prior to presentation.
All care teams on the fragility hip fracture service were advised to administer the 4-dose TXA regimen to all eligible patients at our institution. However, it is important to note that while the majority of care teams at our institution followed this recommended TXA protocol, there were a few care teams that deviated from or were not consistent with the 4-dose TXA recommendation and administered TXA to patients at their own discretion. These deviations are inherent when implementing novel protocols into large departments and such variability replicates a clinical scenario and may improve the generalizability of our findings.
If medically cleared, all patients were taken to the operating room within 24 hours of admission. 1 For patients that were eligible for the 4-dose regimen but had not received the initial admission TXA doses, due to either protocol deviations, misunderstandings by different care teams, or random errors, all these patients were still given 1-g of TXA at the time of surgical incision followed by 1 g 3 hours later. Similarly, there were patients that were deemed ineligible for the 4-dose TXA protocol due to the aforementioned contraindicated comorbidities, but some respective care teams proceeded with an abbreviated two-dose TXA of 1-gram of TXA at the time of surgical incision followed by 1 g 3 hours later for these patients. Additionally, some eligible patients for the 4-dose TXA regimen only received the admission doses of TXA, and the remaining two doses were not given due to protocol deviations, misunderstandings by different care teams, or random errors. All patients were eventually stratified into 4 respective groups: no TXA, admission only doses of TXA, two-dose TXA arthroplasty based (incision and post-operative doses), and the complete 4-dose TXA regimen.
There were 527 total patients admitted to the fragility hip fracture service from April 1, 2019 to September 30, 2019. Of those 527 patients, 19 had insufficient documentation and were removed from analysis, leaving a total 508 patients for analysis. Of the 508 patients, 180 received no TXA, as they were ineligible for the 4 dose TXA protocol due to contraindicated comorbidities. Of the remaining 328 patients, 183 received the complete 4-dose TXA protocol. A subset of patients (n = 32) that were eligible for the complete 4 dose TXA protocol only received the admission and infusion doses. An additional subset of patients (n = 113) did not receive the admission and infusion doses, and only received our abbreviated two dose protocol of incisional and post-operative TXA doses (arthroplasty-based TXA protocol). Again, the formation of these sub-groups were a result of protocol deviations, misunderstandings by different care teams, and/or random errors by the care team. Subgroup analysis of these two groups of patients were performed and compared to the greater cohort of patients who received no TXA or the complete 4 doses of TXA. A multivariate linear regression analysis and intention-to-treat analysis was performed for analysis of nonrandomized intervention study designs. 14
The primary outcome of this study was the rate of allogenic blood transfusion. Demographic data, hemoglobin values, transfusions given, timing of transfusion were recorded. Reasons for ineligibility were also tracked. Transfusion threshold was <7 g/dL as determined by our service’s established blood management protocol, in coordination with a dedicated hip fracture hospitalist. Major adverse events, including cerebrovascular event, myocardial infarction and venous thromboembolic disease were tracked in-hospital and for 90 days post-discharge. Minor adverse events associated with TXA, such as headache, abdominal pain, nasal symptoms, nausea, vomiting, and diarrhea, were tracked in hospital.
Statistical Analysis
Statistical analysis using chi-squared, fisher exact, t-tests, ANOVA, and multivariate analysis was performed to compare patient factors, TXA administration, and transfusion requirements. A multivariate linear regression analysis and intention-to-treat analysis was performed for analysis of nonrandomized intervention study designs. 14 Units transfused was used as the dependent variable, and initial TXA protocol eligibility, surgery >48 hours after injury, admission hemoglobin level, anticoagulation status, malignancy history, renal comorbidities, and vascular comorbidities were included as dependent variables to predict need for transfusion.
To address the selection bias associated with the TXA protocol eligibility criteria, we performed a matched sub-analysis of patients who presented with an admission hemoglobin less than 11.5 g/dL. This group of patients had no significant difference in admission hemoglobin. This was used to control the impact of low hemoglobin on transfusion rates. All statistical analyses were performed using Stata 13.1 (StataCorp, College Station, TX) and SPSS Statistics 28 (IBM Corp. 2021. IBM SPSS Statistics for Windows, Version 28.0. Armonk, NY). Statistical significance was set as P < 0.05, two sided.
Results
Patient Demographics.

Reasons patients did not meet TXA protocol on initial screening.

Transfusion Rate Stratified by TXA Dosing.

Analysis of Transfusions Stratified by Procedure.

Analysis of Transfusions Stratified by Procedure and TXA Dosing.
Multivariable linear regression of variables that predict need for transfusion.

This table shows a multivariable linear regression analysis with an intention-to-treat analysis that predicts need for transfusion. Only TXA administration and admission hemoglobin were significant factors to predict need for transfusion, as well as hemiarthroplasty and CRPP compared to IMN.
Transfusion rate in patients with and without TXA administration in patients with admission Hgb <11.5.

Demonstrates a subgroup analysis of transfusion rates with and without TXA administration in patients with an admission hemoglobin less than 11.5 g/dL.
Abb1: Hgb, hemoglobin; TXA, tranexemic acid.
Adverse Reactions.

Table 4 shows the number patients with reported major adverse events, which included deep vein thrombosis, pulmonary embolus, heart attack, or stroke.
Discussion
This study is an extension of our ongoing experience with a standardized hybrid TXA protocol of 4 doses, starting at the time of admission and continuing through the post-operative intervention, which previously showed that a 4-dose TXA regimen significantly decreases transfusion rates in patients undergoing surgery for hip fragility fractures. 1 In the current study, we found that early administration of IV TXA, 1-gram over 10 minutes followed by an infusion of 1 g over 8 hours at the time of hospital admission to the inpatient unit, can significantly decrease red blood cell transfusion rates in fragility hip fracture patients compared to those who received no TXA. Moreover, fragility hip fracture patients who received the admission dosing of TXA had significantly lower transfusion rates (9.4%) compared to those who received the traditional arthroplasty two-dose TXA protocol (25.7%), given at the time of incision and in the post-operative recovery room. We also found that transfusion rates did not significantly differ in patients who received the admission dosing of TXA compared to those who received the expanded 4-doses of TXA. Therefore, these findings confirmed our primary hypothesis regarding the importance of an early TXA dose relative to the timing of other TXA doses. Early administration of TXA and how it compares to various other TXA dosing schedules has not been investigated in the current literature. These findings have important clinical implications and can better define TXA guidelines for patients undergoing surgery for fragility hip fractures.
In the current study, the authors believed further research was warranted to compare different TXA dosing regimens (ie, no TXA vs only TXA dosing at admission vs two-dose arthroplasty-based protocol, vs 4-dose TXA regimen) to determine which particular dose(s) within the 4-dose TXA regimen were most effective at decreasing transfusion rates in hip fracture patients. While previous studies have reported significant decreases in post-operative transfusions with the use of a singular TXA admission dose in hip fractures, the comparison groups in these studies received no TXA treatment.1,13 Therefore, it is unclear how the admission dosing of TXA compares to other regimens of TXA dosing in patients with fragility hip fractures While the clinical practice guidelines noted by the American Association of Hip and Knee Surgery report that there are no differences in single vs multiple doses of TXA in arthroplasty patients, such recommendations are unavailable for patients with hip fractures undergoing surgery.1,15 In the current study, patients who received isolated TXA admission doses had significantly lower rates of transfusion rates compared to those patients who received the two-dose based arthroplasty TXA protocol (at the time of operative incision and in the PACU). Additionally, there was no difference in transfusion rates between patients who received only the TXA admission dose vs the complete 4-dose TXA protocol. These findings suggest that isolated doses of TXA at hospital admission may be more effective at reducing post-operative bleeding and transfusions than the two-dose based arthroplasty TXA protocol (incision and post-op doses) and is equally effective as the complete 4-dose TXA dosing in hip fracture patients undergoing surgery. These findings highlight the importance of early TXA administration in hip fractures and may be explained by the temporal differences in the onset of bleeding between elective arthroplasty (at the time of incision) and traumatic hip fracture patients (at the time of fracture).13,16,17 These findings may be the first step for developing more defined TXA guidelines and scheduling for hip fracture patients.
There are limited studies that have examined the efficacy of early IV TXA administration to further decrease the hidden blood loss in fragility hip fractures. Baskaran et al performed a meta-analysis of 8 studies (6 randomized controlled trials and 2 cohort studies) examining TXA use in patients undergoing hip fracture surgery and only one study reported results from an admission dose of TXA. 18 While this study reported a significant decrease in transfusions, it was limited to only 43 patients who underwent surgery for intertrochanteric fixation. 18 Similarly, Ma et al. conducted a prospective randomized controlled trial and reported that early (within 6 hours of admission) treatment with 1g IV TXA at hospital admission reduced pre-operative transfusion rates and post-traumatic hidden blood loss in elderly patients with intertrochanter fractures, without increasing the risk of venous thrombosis. 13 However, these studies used only a control group that received no TXA treatment, did not compare the efficacy of admission TXA dose(s) to other TXA dosing regimens, and were confined to only intertrochanteric fractures.13,16,17 The findings in the current study are in agreement with those reported by Baskaran and Ma.13,18 However, it is important to note that our cohort of patients were not confined to only intertrochanteric fractures, and included all types of hip fractures which may increase the generalizability of our reported findings to better define TXA guidelines.
The safety profile of TXA administration (compared to no TXA treatment) in fragility hip fracture patients is well reported and has not been associated with an increased risk of mortality, deep vein thrombosis, pulmonary embolism, myocardial infarction, or stroke.1,7,10,11,13,19 Additionally, the 4-dose TXA model used at our institution has been shown to have no increase in vascular thrombotic events in hip fracture patients compared to those who received no TXA treatment. Although the number of patients in the current study receiving only the admission dose of TXA was small (n = 32), there was no significant difference in adverse events between patients who received TXA doses only at hospital admission compared to those who received the 4-dose TXA protocol (n = 183). While administering 4 doses compared to the admission dose of TXA will most likely not increase the risk for vascular thrombotic events, the benefits of utilizing a single admission TXA dose over the 4-dose protocol may aid in decreasing health care costs and improve medication schedule management for the providing healthcare team.
This study has inherent limitations. With the exclusion criteria employed, we included healthier patients into our TXA cohort. However, we sought to obviate this limitation by using multivariate analysis, which did not demonstrate that renal, vascular, or oncologic disease contributed to transfusion rates. Patients on therapeutic anticoagulation at admission were considered high risk for vascular events and excluded from the TXA protocol. These patients would be expected to have higher rates of blood loss and transfusions; however, multivariate analysis again showed that preoperative anticoagulant was not an independent contributor to transfusion rates. Further, the varying fracture pattern within this cohort also likely influences the rate of transfusion and other outcomes, and we were able to demonstrate that patients treated with IMN required higher rates of transfusion. This is likely due to the ongoing bleeding at the fracture site of intertrochanteric fractures, whereas femoral neck fractures are typically intracapsular with a contained area of bleeding. In addition, we did not perform a sub-analysis of outcomes between patients treated with long vs short intramedullary devices due to limited numbers. While blood loss has been shown to greater in patients treated with long IMNs compared to short, 20 the focus of this study was directed at the type of procedure (eg, hemi vs nail). In our study, the rate of transfusion was higher in patients with an intramedullary nail (27%) vs other procedures (13.8%). While this outcome could be influenced by the number of long vs short nails, our data still suggests that TXA is helpful in decreasing the risk of transfusion risk with IMN procedures. Larger number of patients should be studied to better understand how our TXA dosing can impact transfusion rates in short vs long nail procedures. Lastly, multivariable analysis also shows that both TXA protocol and admission hemoglobin were significant predictors for needing transfusion, though the study is underpowered to exclude the possibility of contributions from other factors such as use of anticoagulation, which may have resulted in a type II statistical error during analysis. Further analysis in a truly randomized fashion is needed to validate these observations. 1
Conclusions
Patients with fragility hip fractures who received IV TXA at hospital admission have significantly lower transfusion rates compared to those who received no TXA or those who received two dose-TXA (at the operative incision and in the post-operative recovery room). These findings suggest that isolated dosing of TXA at hospital admission may be more effective at reducing post-operative bleeding than the traditional arthroplasty dosing (incision and post-op doses) and is equally as effective as the 4-dose TXA protocol in hip fracture patients undergoing surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.