
Abstract
Introduction:
This study aimed to investigate the prevalence of acute kidney injury (AKI) following hip fracture surgery in geriatric patients and to identify predictors for development of AKI with a focus on possible preventable risk factors.
Methods:
In this retrospective cohort study, we reviewed electronic medical records of all patients above 65 years of age who underwent hip fracture surgery at Copenhagen University Hospital, Bispebjerg, Denmark, in 2018. Acute kidney injury was assessed according to the Kidney Disease Improving Global Outcomes guidelines. Multivariate logistic regression analyses were used to identify independent risk factors for AKI.
Results:
Postoperative AKI developed in 28.4% of the included patients (85/299). Acute kidney injury was associated with increased length of admission (11.3 vs 8.7 days, P < .001) and 30-day mortality (18/85 vs 16/214, P = .001). In multivariable analysis, higher age (odds ratio [OR]: 1.05, 95% confidence interval [CI]: 1.01-1.08, P = .004), heart disease (OR: 1.78, 95% CI: 1.01-3.11, P = .045), and postoperative blood transfusion (OR: 1.84, 95% CI: 1.01-3.36, P = .048) were associated with AKI. Moreover, a higher postoperative C-reactive protein (199.0 ± 99.9 in patients with AKI, 161.3 ± 75.2 in patients without AKI) and lower postoperative diastolic blood pressure were observed in patients developing AKI.
Discussion and Conclusion:
Acute kidney injury was common following hip fracture surgery and associated with longer admissions and increased mortality. Patients developing AKI were older and showed several postoperative similarities, including higher C-reactive protein, lower postoperative diastolic pressure, and the need for blood transfusion.
Introduction
Hip fractures have grave consequences for frail older adults and are associated with reduced quality of life, increased morbidity, and mortality. 1 -3 A common postoperative complication is acute kidney injury (AKI) defined as an abrupt decrease in kidney function. 4 -10 Acute kidney injury is a comprehensive clinical syndrome with various etiologies comprising intrarenal and extrarenal pathology. Postoperative AKI is associated with longer hospital stays, increased hospital costs, and considerable morbidity and mortality—this even applies to mild and reversible AKI. 4,11 -15
Previous studies have found older age, preoperative lower glomerular filtration rate, emergent surgery, liver disease, obesity, high-risk surgery, and peripheral vascular occlusive disease to be preoperative predictors of AKI in noncardiac surgery. 4,7,16 Perioperative hypotension has also been demonstrated to be a risk factor for postoperative AKI and death, 17 -19 although there may be a difference between anesthesia-induced blood pressure lowering and hypotension due to intraoperative problems such as bleeding and hypovolemia. 20
Although several studies have examined risk factors for postoperative AKI, the literature on manageable risk factors for AKI in older adults undergoing hip fracture surgery is scarce. 21 The aims of this study were (1) to investigate the prevalence of AKI following hip fracture surgery in geriatric patients and (2) to identify predictors for development of AKI with a focus on possible preventable risk factors.
Methods
Study Design and Patient Population
The present study is a retrospective cohort study. The electronic medical records of all patients above 65 years of age admitted to Copenhagen University Hospital, Bispebjerg, Denmark, between January 1, 2018, and December 31, 2018, with a hip fracture were thoroughly reviewed retrospectively. Hip fracture was defined as International Classification of Diseases (ICD) code DS720 (fracture of femur neck), DS721 (pertrochanteric fracture), or DS722 (subtrochanteric fracture) present in the patient’s medical record. Exclusion criteria were (1) meeting the AKI criteria at admission (see below), (2) lack of postoperative serum creatinine measurement, (3) distal femur fracture, (4) fracture caused by in-hospital fall, and (5) permanent address outside the hospital’s catchment area (leading to lack of data if transferred to another hospital after surgery).
Outcome and Assessment of AKI
Acute kidney injury was diagnosed according to the Kidney Disease Improving Global Outcomes (KDIGO) guidelines 22 : (1) increase in serum creatinine ≥26.5 µmol/L within 48 hours or (2) increase in serum creatinine to ≥1.5 times baseline, which is known or presumed to have occurred within the prior 7 days. Due to lack of information on urine output in patient records, only serum creatinine was used to evaluate AKI. The most recent serum creatinine prior to admission was used as baseline creatinine.
Data Collection
Data retrieved for every patient in the electronic medical record included: Demographic and clinical characteristics: Age, sex, date of death as by July 2019, preoperative comorbidities compiled as an ICD code in the medical record for diabetes type 1 or 2, dementia, chronic kidney disease, hypertension, heart disease, and total number of chronic diagnoses. Characteristics of surgery: type of fracture, type of operation, length of operation, and blood loss during surgery. Characteristics of anesthesia: type of anesthesia, preoperative American Society of Anesthesiologist physical status classification score, and arterial cannula during operation. Geriatric characteristics: geriatric assessment by geriatrician during hospitalization, highest Barthel score during hospitalization, residence at admission and discharge, Confusion Assessment Method score, patient diagnosed with delirium by a physician, and prescription of haloperidol. Medication: Administration of any of the following drugs during hospitalization: angiotensin-converting enzyme (ACE) inhibitor, angiotensin II receptor blocker (ARB), β-blockers, calcium channel blockers (CCBs), bendroflumethiazide, spironolactone, furosemide, nephrotoxic antibiotics (cephalosporines, vancomycin, aminoglycosides), morphine, dexamethasone, nonsteroidal anti-inflammatory drug, metformin, anticoagulants, and antiplatelet drugs. Whether the patient received any of the following drugs prior to admission (as stated in admission note): ACE inhibitor, ARB, β-blockers, CCB, bendroflumethiazide, spironolactone, furosemide, metformin, anticoagulants, and antiplatelet drugs. Blood pressure values: first blood pressure measured after admission; morning blood pressure the first 3 days after surgery; highest and lowest systolic blood pressure (SBP) during anesthesia; highest and lowest diastolic blood pressure (DBP) during anesthesia; whether mean arterial pressure (MAP) at any point during anesthesia was ≤55 mm Hg; longest period where MAP was ≤55 mm Hg during anesthesia. Paraclinical parameters: electrocardiograms; most recent creatinine prior to admission; first and highest creatinine, C-reactive protein (CRP), and potassium during hospitalization; pre- and postoperative albumin, sodium and hemoglobin; pre-, peri-, and postoperative red blood cell transfusion.
Statistical Analysis
Patients were divided into 2 groups (a) meeting AKI criteria 1 and/or 2 and (b) non-AKI patients. For every variable retrieved from the medical records, univariate analysis was performed, using Student t test for parametric data and χ2 or Fisher exact test for nonparametric data. Variables with a 2-tailed P value of less than .05 were examined further in multivariate analysis with binary logistic regression with AKI (present or not) as the dependent variable. The multivariate analyses were made in 3 steps. Based on biological and clinical knowledge, we made conceptual frameworks to identify possible confounders. The first step is the crude analysis between various independent variables and the outcome of interest. In the second step, the association was adjusted for sex and age, and in the third step, additional adjustment for important confounders assessed by the conceptual frameworks was added. After evaluation of the initial findings, we explored more variables in the patients who were given postoperative blood transfusion. All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp, Armonk, New York).
Ethics
The study protocol was approved by the Danish Patient Safety Authority (Ref. no. 3-3013-2934/1), and data were handled according to The Danish Data Protection Agency (Ref. no. P-2019-164). Informed consent was by Danish legislation unnecessary and not obtained due to the observational and retrospective design of the study.
Results
A total of 322 electronic medical records were reviewed. Twenty-three patients were excluded, resulting in a study population of 299 patients (Figure 1).

Exclusion of patients.
Patient characteristics are presented in Tables 1 and 2. The incidence of AKI was 28.4% (85/299). Three patients received dialysis because of AKI and another 4 patients met criteria for dialysis but either refused or dialysis was thought to be futile due to the patients’ condition. The mean age for enrolled patients was 82.4 ± 8.8 years (range: 65-101 years), with significantly higher age in patients who developed AKI (84.7 ± 7.7 years) than in non-AKI patients (81.4 ± 9.1 years; odds ratio [OR]: 1.05, 95% confidence interval [CI]: 1.01-1.08, P = .004). Of this, 80 of 299 patients were male with no significant sex difference between the 2 groups.
Description of Cohort, Presented as Mean ± SD or No. (%) Univariate Analyses.

Abbreviations: AKI, acute kidney injury; SD, standard deviation.
a χ2 test.
b Student t test.
c Fisher test.
Clinical Characteristics, Presented as Mean ± SD or No. (%) Univariate Analyses.

Abbreviations: AKI, acute kidney injury; CRP, C-reactive protein; DBP, diastolic blood pressure; MAP, mean arterial pressure; SBP, systolic blood pressure; SD, standard deviation.
a Student t test.
b Fischer test.
c χ2 test.
Clinical Outcomes of AKI
At follow-up in July 2019, 29.1% of the included patients had died. Death during hospitalization, 30-day mortality, and overall mortality were more frequent in patients developing postoperative AKI, and length of hospital stay was significantly longer for these patients. These associations remained significant when adjusting for sex and age (Table 3).
Risk of Death After AKI—Multivariate Analysis.

Abbreviations: AKI, acute kidney injury; CI, confidence interval; OR, odds ratio.
Nonmodifiable Risk Factors for AKI
As presented in Table 4, several comorbidities were associated with AKI. When adjusting for sex and age, heart disease and chronic kidney disease increased the risk of AKI. In the fully adjusted model, only heart disease (OR: 1.78, 95% CI: 1.01-3.11) was associated with postoperative AKI. No significant association between the number of chronic diagnoses and AKI was found.
Comorbidity and Risk of AKI.

Abbreviations: AKI, acute kidney injury; CI, confidence interval; CKD, chronic kidney disease; OR, odds ratio.
a Adjusted for sex, age, heart disease, hypertension, diabetes type 1 and 2, and chronic kidney disease, respectively.
Possible Modifiable Risk Factors for AKI
Longer surgeries, blood loss during surgery and presence of postoperative blood transfusion were associated with development of postoperative AKI in the univariate analysis. In the fully adjusted model, the association between blood loss during surgery and AKI was no longer significant (Table 5). However, when mutually adjusted, postoperative blood transfusion remained significantly associated with development of AKI. The association between blood loss and AKI was not explained by the type of fracture neither by the type of operation (data not shown).
Blood Loss, Blood Transfusion, and AKI.
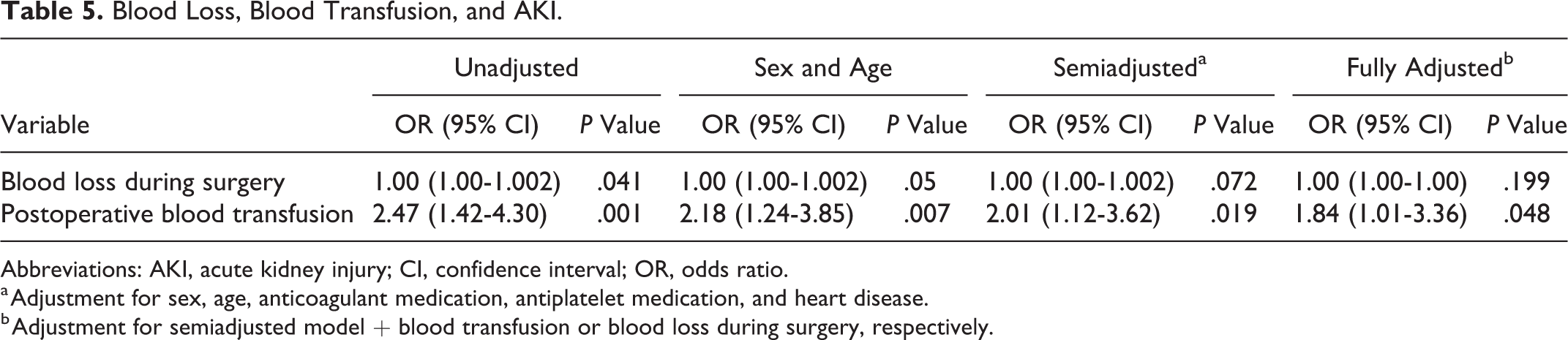
Abbreviations: AKI, acute kidney injury; CI, confidence interval; OR, odds ratio.
a Adjustment for sex, age, anticoagulant medication, antiplatelet medication, and heart disease.
b Adjustment for semiadjusted model + blood transfusion or blood loss during surgery, respectively.
A past medical history of hypertension and AKI was not significantly correlated. In the univariate analysis, however, wide pulse pressure and high SBP at admission were associated with AKI. This association did not remain significant when adjusting for sex and age (Table 6). During surgery, many patients experienced low blood pressure values. Seventy-one percent (71%) of the patients had at least one episode where MAP was 55 mm Hg or less during surgery. We did not find significant differences in blood pressure measurements or duration of hypotension during surgery between patients with and without AKI. Neither did the percentage difference between admission blood pressure and lowest SBP during surgery differ between the 2 groups. Patients developing postoperative AKI had significantly lower DBP the first 2 days after surgery, and AKI patients were more often administered β-blockers and diuretics during hospitalization. There was no association between AKI and preadmission antihypertensive medication or administration of other kinds of antihypertensive medication during hospitalization apart from β-blockers (21/85 vs 27/214, P = .01) and diuretics (48/85 vs 61/214, P < .001).
Pulse Pressure.
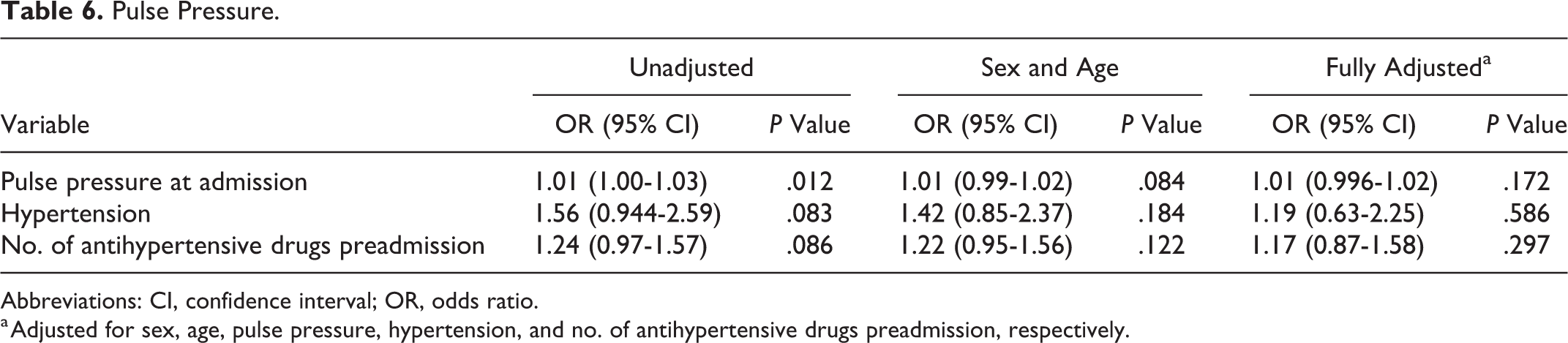
Abbreviations: CI, confidence interval; OR, odds ratio.
a Adjusted for sex, age, pulse pressure, hypertension, and no. of antihypertensive drugs preadmission, respectively.
Other Clinical Differences
Patients with AKI had significantly higher postoperative CRP than non-AKI patients. This finding remained significant after adjustment for the length of operation (based on the theory that longer operations are associated with greater trauma causing higher CRP). The first blood tests after surgery showed significant lower levels of albumin and hemoglobin in AKI patients, whereas there was no significant preoperative difference. The use of arterial cannula during surgery was significantly more frequent in AKI patients but did not remain significant after adjustment for sex, age, and comorbidities. No association was found between AKI and nephrotoxic medication during admission (data not shown). The average postoperative hemoglobin in patients given postoperative blood transfusion was 8.5 g/dl (standard deviation [SD]: 1.4) as compared to 10.8 g/dl (SD: 1.6) for patients not given postoperative blood transfusion. No other clinically significant differences were observed between patients given or not given postoperative blood transfusion.
Discussion
In this observational, retrospective study of hip fractures in older adults, we found an incidence of AKI of 28.4% according to the KDIGO criteria. Acute kidney injury was associated with longer admissions and patients with AKI often died during admission or within 30 days after surgery, even when the AKI was relatively mild and did not require dialysis. This finding is consistent with other studies where the 30-day mortality rate after AKI has been reported as high as 15% to 19% 4,21 and where even small changes in creatinine double the risk of short-term death. 15 These high mortality rates stress the probable importance of early diagnosis and prevention of AKI to improve the outcome after hip fracture surgery in older adults.
We found that heart disease and preexisting renal disease were nonmodifiable risk factors of AKI, consistent with earlier studies. 8,20,21 However, only heart disease was an independent risk factor. Our finding of a wide pulse pressure and high SBP at admission may also be considered as a proxy for atherosclerotic disease and heart disease. 23 Our findings are consistent with the literature and suggest that atherosclerosis and heart disease are important predictors for AKI after hip fracture surgery, and special attention to these patients during the hospital admission may be prudent.
Importantly, we also found postoperative blood transfusion to be associated with increased risk of AKI, even after adjustment for blood loss during surgery, heart disease, and anticoagulant medication. Blood transfusion has been reported to substantially increase mortality and infections in orthopedic patients. 24,25 An association between blood transfusion and AKI has also been seen after percutaneous coronary intervention 26 and cardiac surgery. 27 In our study, 43% of patients receiving postoperative blood transfusion also had AKI during the admission. In Denmark, red blood cell transfusion is recommended when hemoglobin is <6.9 g/dL (<7.6 g/dL for patients with chronic heart disease) or when the patient experiences symptoms of anemia. In our cohort, most patients were given blood transfusions at higher levels than 7.6 g/dL because of symptoms. Liberal blood transfusions have been reported to increase the risk of transfusion-related acute lung injury and heart failure 28 possibly due to immunological reactions to blood affecting these organs. 29 However, it should be stressed that the blood transfusions usually are a consequence of acute illness in the perioperative period: In everyday practice, clinicians often give blood to patients with signs of hypoperfusion and physiological stress due to infections and hypovolemia. This may also explain the lower DBP the first 2 days after surgery in the AKI group. In our study, the link between blood transfusion and AKI is probably an expression of acute illness in the patients more than an explanation of AKI caused by the blood transfusion itself.
Low blood pressure during hip surgery is common. It has been argued that low blood pressure could lead to impaired renal perfusion and thereby risk of AKI. 19 However, in our study, perioperative blood pressure values and MAP did not differ between the groups with and without AKI. There are inconsistencies in the literature regarding this association. A few studies have found an association between intraoperative hypotension and AKI, 17,19 suggesting hypotension to reduce renal blood flow and thereby causing renal damage, 19 although even longer duration of hypotension has been shown to be unrelated to AKI. 18,20 Intraoperative hemodynamic optimization has also been reported to be effective in reducing postoperative acute renal injury. 9,30 In our study, AKI patients had larger bleedings during surgery but did not experience lower perioperative blood pressures than non-AKI patients. Patients with advanced age, atherosclerosis, hypertension, and chronic kidney disease often have impaired autoregulation of blood pressure, which can cause kidney function to deteriorate even when patients have blood pressure values within normal values. 31 Our data did not strengthen the widespread hypothesis that perioperative hypotension is the main cause of AKI after hip fractures.
A few differences were found between the 2 groups when comparing paraclinical findings. Most notably, postoperative CRP was found to be significantly higher in patients with AKI even after adjustment for duration of surgery and type of surgery and fracture. The peak in CRP after hip surgery is partly related to the trauma but could also be related to infections and inflammation. More specific data on infections were not available in the current study, but AKI related to systemic infections seems to be a plausible explanation for this association.
In the present study, AKI was evaluated according to the KDIGO criteria and a relatively high prevalence of AKI (28%) was observed. The definition of AKI has been subject to debate, which was why the KDIGO criteria were made based on the formerly used Risk, Injury, Failure, Loss of kidney function and End-stage kidney disease (RIFLE) classification and the Acute Kidney Injury Network criteria. 22 If we instead had used the RIFLE classification (defining AKI as present when serum creatinine was >1.5 of baseline [KDIGO criterium 2]) in the present study, the prevalence of AKI was 17.4% (n = 46, missing baseline creatinine on 34 patients). All univariate analyses were also performed across these 2 groups, leading only to slight changes in data (data not shown).
Strength and Limitations
The present study is a single-center study where all patients admitted during 1 year were included. In Denmark, only public hospitals admit acute patients, and our study therefore includes a complete cohort of all patients in Central and Northern Copenhagen with acute hip fractures in 2018. This is an important strength of the study, eliminating most of the risk of selection bias. Further, we had complete data sets from almost all patients. The study is observational and retrospective, and data were initially collected as part of routine clinical work without consideration of our study, which also reduces the risk of bias. However, some limitations are present. The sample size is relatively small, and we examined many potential predictors. Therefore, data may have been overfitted by including many explanatory variables, and our findings might not all be reproducible. Hence, the study should mainly be considered as explorative and hypothesis generating. All data were collected from the patients’ electronic medical records, and we therefore had to rely on the correctness of other doctors’ registration. Because baseline levels of serum creatinine often are unknown in acutely admitted patient, the most recent serum creatinine in the medical records prior to admission was used as an estimate of baseline creatinine levels. However, these creatinine levels often originate from earlier admissions and may be affected of other diseases at that time. Other variables of high interest to the research questions were unfortunately not readily available from the hospital records, including administration of fluids, volume of blood transfusion, continuous measurements of hemoglobin, 32 urine output, and clinical data on infections. Confounding by indication is an important concern in observational studies as ours. We have adjusted for the most probable confounding factors but acknowledge that an interventional study would be the ideal design to study the relation between postoperative blood transfusions and AKI.
Conclusions
Acute kidney injury was common following hip fracture surgery and associated with longer admissions and increased mortality. Higher age and heart disease were nonmodifiable and independent risk factors of postoperative AKI. Special attention to high-risk patients during hospital admission, and the clinical individualization of the need for blood transfusion is prudent.
Footnotes
Authors’ Note
The data files are stored by Bispebjerg and Frederiksberg Hospital, Copenhagen, Denmark, on a server dedicated to research and with security according to Danish national rules. The data are available on request by the author, but restrictions apply to the availability of these data according to Danish law and are therefore not publicly available.
Acknowledgments
The authors thank Mette Brimnes Damholt for helpful discussion and sharing of insights on kidney patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.