
Abstract
Introduction
Tranexamic acid can decrease blood loss related to surgery and trauma. The primary objective of this study is to examine if the use of a single dose of peri-operative TXA significantly decreases the rate of allogenic blood transfusions in the setting of operative care of hip fractures. Secondary objectives included examining if total blood loss was decreased by TXA in operative hip fractures as well as examining the safety of TXA by measuring the rates venous thromboembolism (VTE).
Methods
Retrospective chart review of 505 patients who were operatively treated for hip fractures at a single facility was performed. In a non-randomized fashion, 307 patients received TXA and 198 patients did not. Patients received 1 gram of TXA prior to incision. Blood transfusion was the primary end point. Blood loss was calculated using the hemoglobin balance method. Chart was reviewed for VTE events during hospitalization.
Results
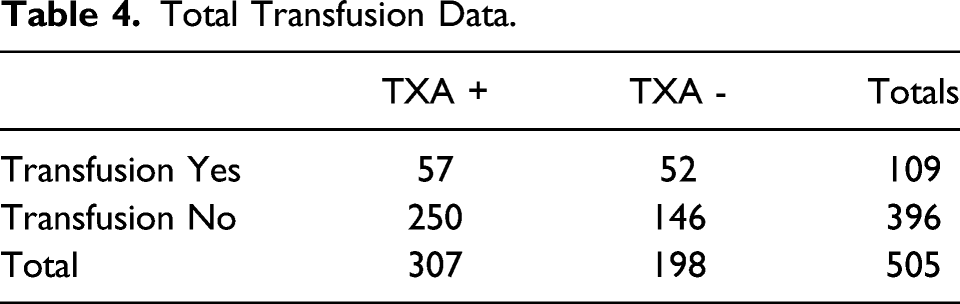
505 patients were analyzed. The use of single perioperative dose of TXA in the surgical management of hip fracture resulted in absolute risk reduction of transfusion of 7.7% and relative risk reduction of transfusion by 29%. This was statistically significant with P =.04. Patients who received TXA on average lost 235 ml less blood compared to those who did not receive TXA (P <.0001). No increase in VTE events were found in either group during hospitalization.
Conclusion
This study supports the use of TXA is decrease blood loss and transfusion rates in patients with hip fractures. TXA can be used routinely to decrease complications in this usually fragile population.
Introduction
Globally, 4.5 million people are disabled from hip fractures each year and hip fracture is among the top 10 causes of disability and the 3rd most expensive cost center for Center of Medicare Services (CMS) in the United States. 1 Hip fractures are associated with a number of complications, including blood loss anemia that requires allogenic blood transfusion. Blood transfusion in the setting of hip fracture care is not a benign process and through immunosuppression, is associated with increased rates of infection, delayed wound healing and fracture nonunion. 2 It would be ideal to have a strategy to decrease the chance of allogenic blood transfusion in any patient with an operative hip fracture.
In other surgical disciplines, tranexamic acid (TXA) has been shown to decrease blood transfusion rates in a wide variety of clinical scenarios, including primary hip arthroplasty. TXA is a synthetic reversible competitive inhibitor to the lysine receptor found on plasminogen. The binding of this receptor prevents plasmin from binding and stabilizes the fibrin matrix. 3 A systematic review from 2016, which included 7 studies and over 770 patients, concluded that intravenous (IV) TXA was associated with a 46% risk reduction in blood transfusion following hip fracture repair. 4 This level of risk reduction translates into a number of patients to treat to prevent one blood transfusion of about 1 in 8.
The primary objective of this study is to examine if the use of a single dose of peri-operative intravenous TXA significantly decreases the rate of allogenic blood transfusions in the setting of operative hip fractures. Secondary objectives include examining if total blood loss was decreased by TXA in operative hip fractures as well as examining the safety of TXA by measuring the rates venous thromboembolism (VTE) in the treated population.
Materials and Methods
This is a retrospective chart review of all hip fracture patients cared for at a single hospital by 2 orthopedic surgeons from May 1, 2016 through May 31, 2020. Institutional review board (IRB) approval was obtained prior to collecting the data. Billing information was used to identify the patient population.
Inclusion Criteria
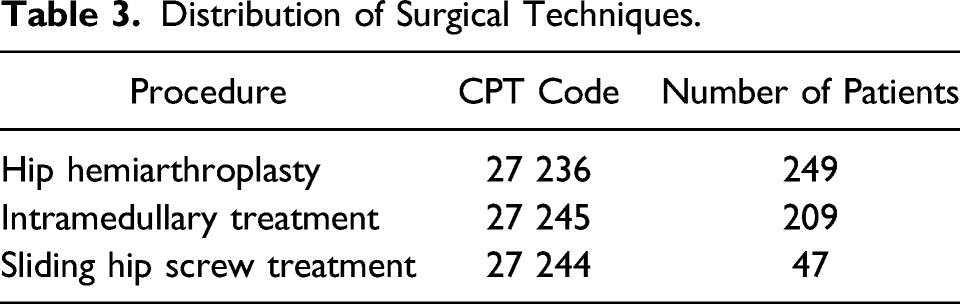
• Patients who underwent operative hip fracture repair, with either hemiarthroplasty, intramedullary nail treatment, or sliding hip screw treatment. • Age of 60 years or greater. • Patients were included independent of use of anticoagulant medication at the time of injury.
Exclusion Criteria
• Patients with active metastatic adenocarcinoma. • Age of 59 years or younger. • Patient with previous hip arthroplasty or periprosthetic proximal femur fracture • Patient who required a pre-operative blood transfusion due to symptomatic anemia
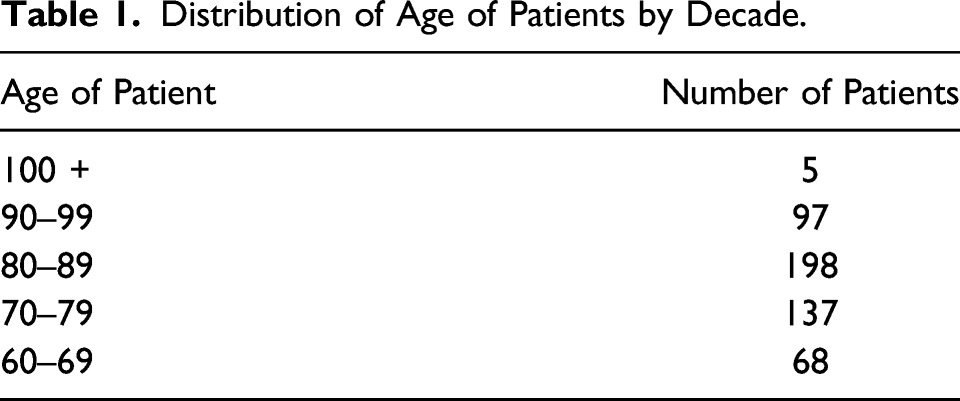
Distribution of Age of Patients by Decade.
Demographic of (+) TXA vs (−) TXA.

All patients were admitted to a geriatric co-management program, with inpatient hospitalist service as primary admission team with consultation from the orthopedic team. Patients were optimized with the goal to be in surgery within 24–36 hours if possible. Patients typically received general anesthesia with or without a peri-operative nerve block. Nerve block utilization was at the discretion of the surgeon in consultation with the anesthesiologist. Intraoperative blood transfusions were not utilized. Fluid management was at the discretion of the anesthesiologist during surgery. Chemical VTE prophylaxis was most commonly enoxaparin 40 mg subcutaneous (SQ) daily starting on post-operative day 1 and continued for 21 days. If the patient was already on coumadin or a DOAC, then the baseline medication was resumed on post-operative day 1. The decision for blood transfusion was at the discretion of the hospitalist service. Typically, hemoglobin (Hgb) less than 7 was indicated for transfusion. If Hgb was 8 or less and the patient had persistent symptoms, such as lightheadedness, orthostatic hypotension or tachycardia, then transfusion was heavily considered.
Distribution of Surgical Techniques.
For statistical analysis, rates of blood transfusion were calculated for those patients who received TXA and those who did not, which are the control event rate and experimental event rate. The absolute risk reduction was then calculated and then converted to a number needed to treat (NNT). From this data, the relative risk reduction was calculated. As the blood transfusion results data is dichotomous or non-continuous, so a 95% Confidence Interval for the difference between 2 independent proportions was calculated. Additionally, a 2x2 Chi Square analysis was performed with significance set to P <.05. The calculated blood loss, using the hemoglobin balance method, for each patient was recorded. The mean blood loss and standard deviation for each group was calculated. Using this information, the 95% CI for single samples was calculated using the Z statistic. Since these data were continuous, an unpaired 2 tailed t-test was utilized. Significant was set to P <.05. Microsoft Excel was used for some calculations. Online statistical calculators were used for other tests. The 95% Confidence Interval for the difference between 2 independent proportions was accessed at http://vassarstats.net/prop2_ind.html. Chi square analysis calculator was accessed at https://www.socscistatistics.com/tests/chisquare/default2.aspx. The Z statistic calculator was accessed at https://www.socscistatistics.com/confidenceinterval/default3.aspx. The unpaired 2 tailed t-test calculator was accessed at https://www.graphpad.com/quickcalcs/ttest2/.
Results
Total Transfusion Data.
Blood Loss in mL as Calculated by the Hemoglobin Balance Method for All Patients.

In terms of safety, no VTE events, ischemic CVA, or myocardial infarction events were noted for any patient in this study during their admission for care of a hip fracture during hospitalization in both groups.
Discussion
In this study a single intravenous perioperative dose of TXA significantly decreased the risk of blood transfusion in the setting of operative management of patients with hip fractures. The hypothesis that TXA could decrease transfusion risk is supported. In addition, the use of TXA demonstrated a significant decrease in blood loss without a measurable increase in adverse effects, such as VTE, stroke, or MI. This paper adds support to the body of literature regarding the positive effects of the use of TXA for hip fracture surgery.
TXA has been using in a variety of surgical disciplines to decrease blood loss. In hip fracture care, a review of 7 studies and 770 patients estimated the decreased risk of transfusion by approximately 46% and the NNT of 8. 4 One of the challenges in studying TXA use in hip fractures is that different dosing regimens are used. Our study showed a NNT of 13, which is slightly higher than found in the review and could represent sampling error. Another possibility is that this group of patients could be more frail than those patients in other studies. It is not known if age has an independent effect on the utility of TXA. Also, the single dose protocol may also have been suboptimal for some patients compared to a weight-based protocol or multiple dose protocol. This study compares favorably to an RCT by Zuffery et al 6 in which the relative risk reduction was 30% for perioperative blood transfusion in a population of all types of hip fractures using IV TXA.
Strengths of this study include the relatively large sample of patients treated at a single facility with a simple protocol for the use of TXA. A variety of hip fractures were treated with appropriate surgical management. This would suggest TXA is helpful for the whole variety of hip fracture seen in a typical community practice environment. Data collected from the chart were objective and straight forward to find. For example, if a patient received a blood transfusion, this was easy to find in the medical record. Also, no adverse effects were identified.
Weaknesses of this study include the retrospective chart review nature of the study which comes with those well-known biases. Patients were not randomized. Blood loss was estimated using the hemoglobin balancing method which does rely upon using equations that estimate blood volume for patients.
At our institution, a single dose of 1 gram of TXA costs $4.97. The average cost of blood transfusion is approximately $1500. With a NNT of 13, TXA is a cost-effective treatment at our institution. The decreased transfusion rate from just transfusion costs alone provides significant savings to our hospital. It is also possible that other savings could be realized in terms of decreased complication rates and readmission rates, but that was beyond the scope of this study.
In terms of safety in this study, no increase was observed in VTE events occurred during hospitalization. Recent meta-analysis of 216 studies including 125 550 patients demonstrated no increase in VTE or myocardial infarction or cerebral infarction events over patients who did not receive TXA. 7 Another recent paper showed no increase in MI or VTE events in approximately 26 000 patients with history of coronary artery disease undergoing elective hip and knee arthroplasty procedures. 8 TXA appears to be a safe medication in terms of causing blood clots or other coagulation complications. This is consistent with the mechanism of action of TXA, which stabilizes existing clots and so works at active sites of bleeding.
Our study included both intracapsular and extracapsular hip fractures. It has been shown that extracapsular patterns have increased pre-operative average blood loss compared to intracapsular patterns. 9 The average pre-operative blood loss was .6 gm/dl for intracapsular fracture patterns and was 1.1 gm/dl for extracapsular hip fracture patterns. Extracapsular hip fractures have a potentially much larger space to bleed into pre-operatively. Given that TXA appears to be safe, a next possible step of the use of TXA to consider would be to dose TXA in the emergency department at the time of admission as well as in the perioperative period. This could further decrease blood loss and therefore blood transfusion risk, especially in extracapsular patterns.
Conclusion
In summary, the perioperative use of a single dose of 1 gram of TXA during the operative management of fractures demonstrated significant decrease in blood transfusion rate post-operatively and significantly decreased blood loss as measured by the hemoglobin balance method without any measurable increase in adverse effects. This study supports the routine use of TXA in the operative treatment of hip fractures. The use of TXA represents another tool in the orthopedic surgeon’s arsenal to decrease complications in this usually frail population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.