
Abstract
Introduction:
The presence of a fragility fracture increases the risk of new fractures. The timely and prompt initiation of treatment for osteoporosis can reduce the incidence of new fractures, for which adherence to management is a determining factor. The main objective of the study was to characterize the secondary prevention program for fragility hip fractures in patients older than 65 years, determine adherence to treatment and its effect on the appearance of new fractures in the established follow-up period.
Materials and Methods:
A descriptive retrospective cohort study was carried out. Patients older than 65 years with a fragility hip fracture treated by an Orthogeriatric Clinical Care Center between May 2014 and April 2020 who completed a one-year follow-up were included.
Results:
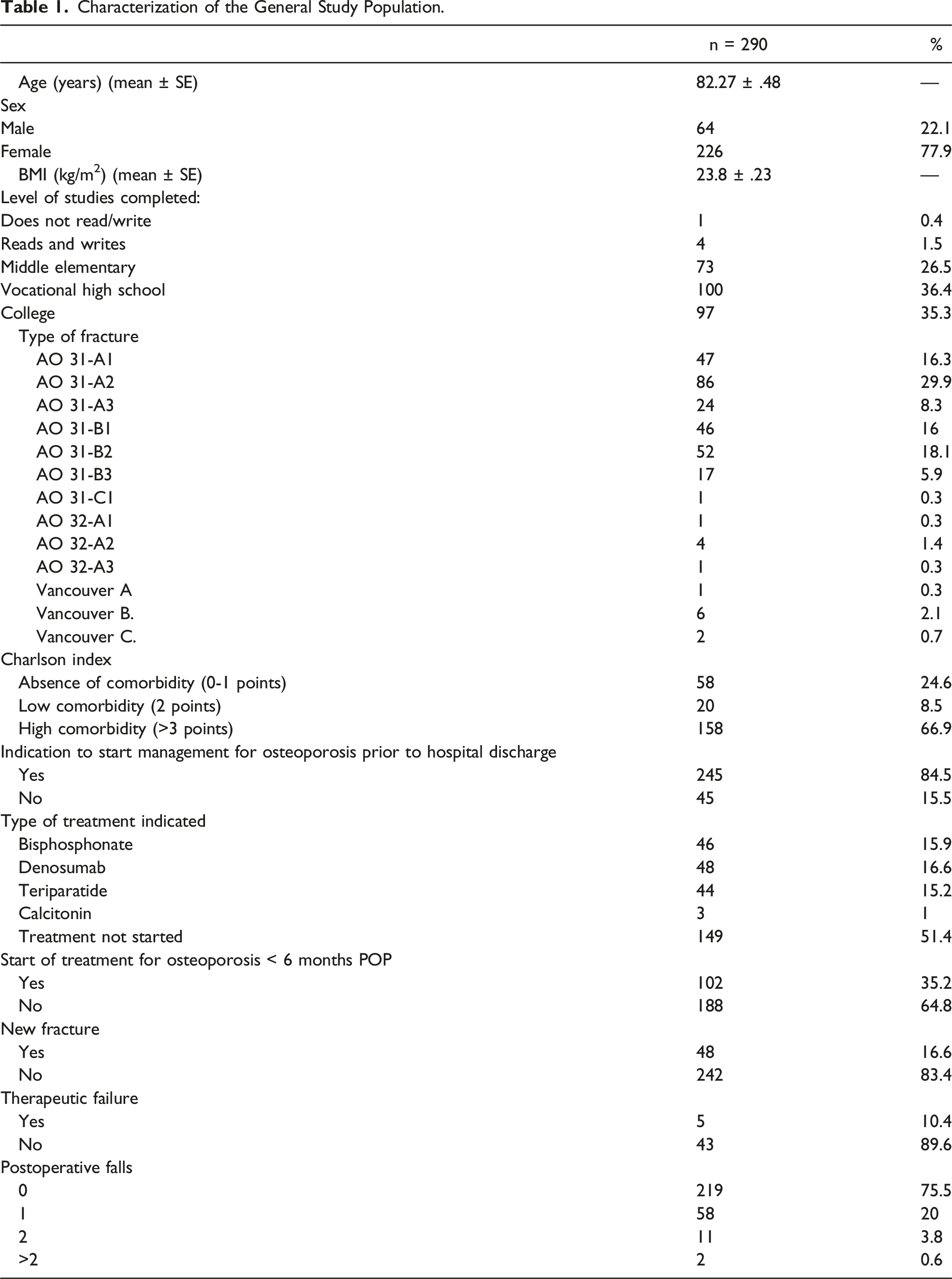
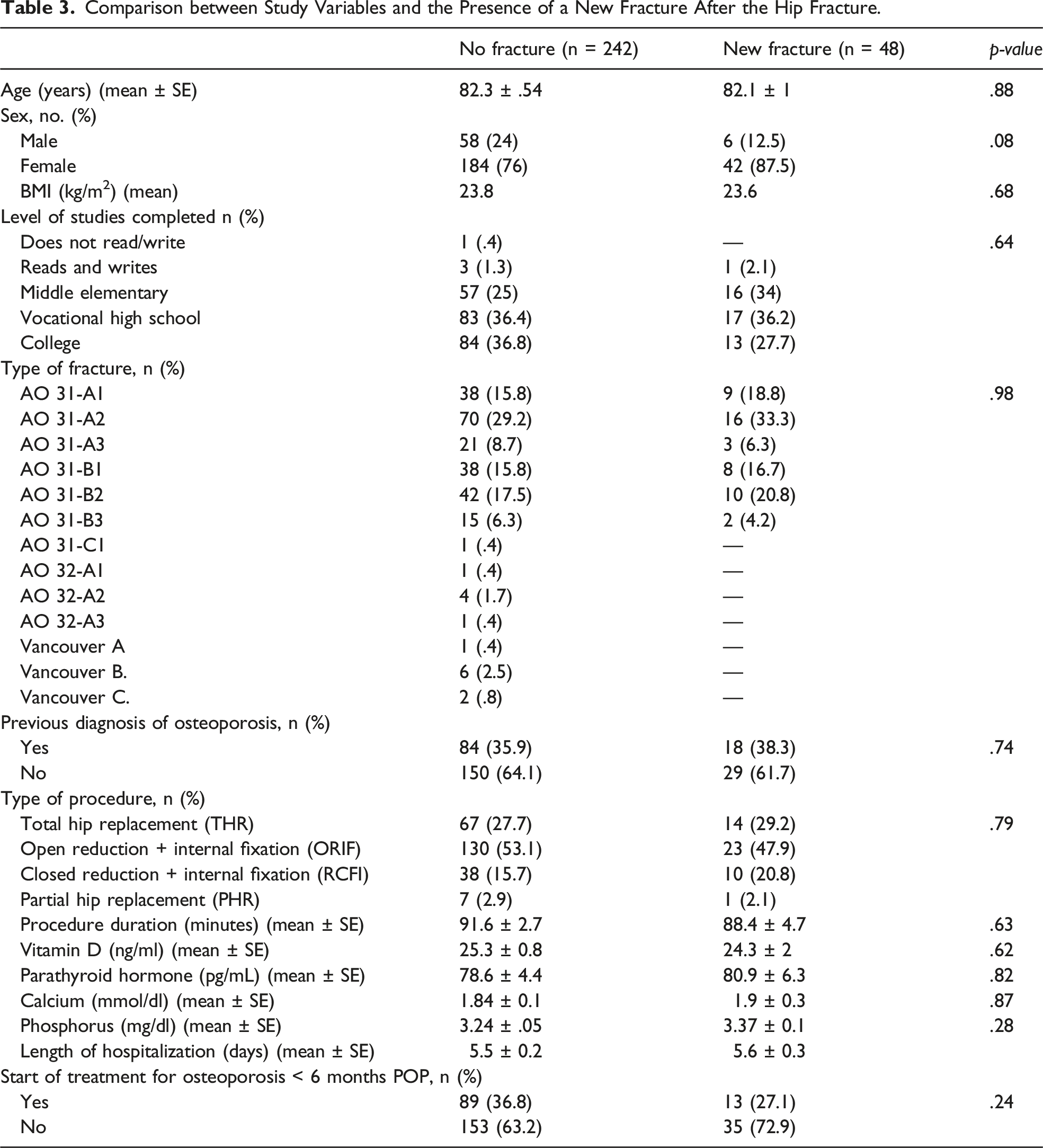
A final sample of 290 patients was obtained (226 women and 64 men) with an average age of 82.27 years. It was found that 84.5% of patients received indications to start osteoporotic management prior to hospital discharge and only 35.2% started the treatment in the first 6 postoperative months. 16.6% (n = 48) of patients presented a new fracture, with no significant difference between those who started their osteoporosis treatment in a timely manner. Out of the 48 patients, 5 patients (10.4%) met therapeutic failure criteria.
Discussion:
Most patients (84.5%) received indications for starting osteoporotic treatment before hospital discharge, nevertheless 35.2% started it during the first 6 postoperative months. 16.6% of patients presented a new fracture during follow up, of which only five met therapeutic failure criteria.
Conclusions:
No significant differences were found between the presence of new fractures and early initiation of osteoporotic management. However, literature shows that prompt and timely osteoporotic treatment reduces the incidence of new fractures, thus measures must be implemented to strengthen the adherence and surveillance of patients to the indicated treatment.
Introduction
Osteoporosis, according to the consensus of the National Institute of Health of the United States (NIH), is defined as a skeletal disorder characterized by deterioration in bone resistance, which predisposes patients to a greater risk of fractures. 1 Fragility fractures occur with low-impact trauma that result in a fracture, for example, a fall from one’s own height or a lower height. Among these, hip fractures in patients ≥65 years of age have a significant impact on quality of life, loss of independence, and mortality during the first year after the event. 2 The incidence of fragility fractures in the elderly has increased, with an annual mortality of 2 to 3 times in patients 80 years or older with hip fragility fractures. 3
In literature, fragility hip fracture 30-day mortality ranges between 8% to 10% and at 1 year from 20% to 28%. 4 The implementation of orthogeriatric clinical care centers for the treatment of patients with hip fractures has had a favorable impact in terms of reducing morbidity and mortality. Simunovic et al 5 found that after treatment at an orthogeriatric center, the annual mortality rate for hip fractures decreased from 23% to 9.1%. 5 This shows the importance of modifying the treatment approach of these patients.
Additionally, various observational and prospective studies have shown that the presence of a fragility fracture significantly increases the risk of new fractures.6,7 Given this, a wide range of available therapies have emerged to treat osteoporosis in these patients as a method of secondary prevention. Several of these management schemes have been shown to reduce the incidence of fractures by 30% to 50%, even among individuals who have suffered multiple prior fractures. There is also evidence showing that management of osteoporosis is associated with reduced mortality rate. 8
Studies show that in patients whose treatment includes antiresorptive therapy, a reduction in the risk of fracture can be observed after 6 months. In one study, the incidence of a second hip fracture was 4.2% in patients with adequate bisphosphonate intake for 1 year after the initial hip fracture compared with 10.9% in patients not following an antiresorptive therapy plan. 9 This demonstrates the importance of early initiation of osteoporotic management in patients who have already suffered a fracture and the significant impact that it can have 1 year after surgery.10,11 Despite existing evidence, initiation of this type of treatment plan for patients with prevalent fractures, including those with hip fractures, has been disappointingly low. 12
In the Fundación Santa Fe de Bogotá (FSFB), the Orthogeriatric Clinical Care Center (OCCC) was established in 2014 and was certified by the Joint Commission International (JCI) in 2018. The OCCC coordinates the co-management and postoperative follow-up of patients who are 65 years or older that suffer a fragility hip fracture between Orthopedics, Geriatrics and Anesthesiology. One of its main goals is to assure that the patient is operated in the best optimal conditions within 48 hours since the arrival at the Emergency Room. At our institution, the average time from admission to surgery is 28.71 hours. In the postoperative period, orthopedics and geriatrics continue the co-management, and emphasis is placed on the early start of mobility via physiotherapy sessions. Another objective of the center is early discharge, with discharge planning beginning at admission. This plan includes treatment for osteoporosis or a densitometric study before starting outpatient treatment. The evaluation, follow-up, and prescription of osteoporosis medication are all handled by the OCCC. In patients with severe vitamin D deficiency or conditions that prevent the start of immediate treatment, a densitometry test and tests for calcium and Vitamin D levels are conducted as soon as possible. Based on these results, a specific outpatient treatment plan is formulated. Therapeutic failure was considered when a patient who has been adhering to the prescribed management plan has two or more new fragility fractures during the first 12 months after starting treatment, or 1 or more new fragility fractures beyond those first 12 months. 13
The timely start and adherence to the established management are recorded in the follow up that each patient has after surgery. In those patients who cannot attend a consultation or receive a home visit, follow-up is done by telephone at 3, 6, and 12 months postoperatively.
This study analyzed the secondary prevention program for fragility fractures in patients 65 years or older with hip fracture who underwent surgical management to determine patient adherence to the secondary prevention program and the effect of the program regarding the appearance of new fractures after the start of pharmacological management for osteoporosis.
Methodology
Study and Population
This was a descriptive retrospective cohort study of patients over 65 years of age with a fragility hip fracture who required surgical management and were admitted to the Orthogeriatric Clinical Care Center of the FSFB between May 2014 and April 2020.
Inclusion Criteria
Patients of the clinical care center of the FSFB who completed at least 1 year of follow-up in the FSFB and who could be contacted by telephone and/or attend a follow-up consultation were included.
Exclusion Criteria
Patients that did not provide information on osteoporosis treatment or did not have any knowledge about their treatment were excluded.
Sample Size and Statistical Analysis
The sample size consisted of a census of patients older than 65 years of age with a diagnosis of hip fracture who received surgical management at the FSFB from May 2014 to April 2020, and who did not present exclusion criteria.
The sample size was calculated for proportions with an alpha level of significance of .05, a power of 80%, and an estimated sampling error of 6%. The sample size estimate was 252 patients.
For statistical analysis, the Chi-square test and Fisher’s exact test were performed to determine the association between discrete variables and new fractures. The Shapiro-Wilk test was used to establish whether the continuous variables had a normal distribution. T and Mann-Whitney tests were performed to determine the relationship between continuous variables and new fractures. All analyses were performed using the Real Statistics resource pack (version 7.8 July 2021) and SPSS V27.
Ethical Considerations
All patients were asked to sign an informed consent in which they agreed to be managed by the orthogeriatric clinical care center and to be part of the database. The study was approved by the corporate research ethics committee of Fundación Santa Fe de Bogota, which is governed by the Declaration of Helsinki of the World Medical Association (WMA) “as a declaration of ethical principles for medical research with human beings, including research on identifiable human material and data” (WMA, 1964/2018).
Results
Characterization of the General Study Population.
Types of Fragility Fracture After Initial Hip Fracture.

Comparison between Study Variables and the Presence of a New Fracture After the Hip Fracture.
Discussion
Hip fracture is the most severe consequence of osteoporosis due to the significant impact it has on functionality, comorbidity, and mortality. 10 Studies have shown that having one fracture significantly increases the risk of having additional fractures, which carry with them an increased risk of mortality, hospitalizations, disability, and admission to long-term care facilities and nursing homes.9,11,14
Because of these risks, the National Osteoporosis Foundation’s Physician’s Guide to the Prevention and Treatment of Osteoporosis states that people over 50 years of age with a hip fracture should institute a risk assessment and preventive measures for the appropriate treatment for osteoporosis, as indicated. 15 However, it has been seen that medications for the treatment of osteoporosis have been underused in clinical practice, with studies showing that a considerable proportion of patients do not receive any type of osteoporotic management after a fracture. 12 Associated with this, patient adherence to these treatments has become a challenge, with studies showing figures of 15% of patients following their treatment plan following 1 year after any osteoporotic fracture and 21% adhering to treatment after a hip fracture. 16
In the present study, it was found that before hospital discharge, 84.5% of patients with hip fracture received indications associated with the start of treatment for osteoporosis (eg a bone densitometry order to determine management or the prescription of a specific drug), and 35.2% started the treatment ordered during the following 6 months, which despite being a low figure, compares positively with what was found in studies such as the one by Solomon et al (2014), in which 24% of patients used some medication for osteoporosis in the 12 months post hip fracture. 14 Due to the retrospective quality of the study, it was difficult to identify and quantify the exact reasons why the patients did not start treatment on time; nonetheless, it was observed that impediments associated with medical insurance, non-attendance at follow-up consultations, and patients not undergoing follow-up additional laboratory tests to determine the optimal drug to use contributed to non-compliance with osteoporotic management.
Of the total sample, 16.6% of the patients presented a new fracture during follow-up, among which the most common were those of the hip (contralateral followed by the previously fractured), pelvis, and distal radius. Of these, only five patients met therapeutic failure criteria. A higher incidence of new fractures was observed in the group of patients who did not start treatment for osteoporosis on time compared to those who did, although the difference between the two groups was not statistically significant.
Conclusion
Early initiation of pharmacological treatment for osteoporosis is of significant importance to prevent further fractures in patients who have sustained a fragility fracture of the hip. In the present study, it is observed that most of the patients treated by the Orthogeriatric Clinical Care Center were advised to begin early osteoporotic management; however, it is important to determine what the main reasons were that led many of them to not comply with the recommended treatment. Also, strategies should be established that encourage adherence to the recommendations of the medical team.
Limitations
The main limitation of this study was the loss of information due to the retrospective nature of the study and the follow-up time of the patients. Also, the loss of follow-up of some patients due to personal and administrative reasons.
Footnotes
Acknowledgments
Gerardo Ardila Duarte M.Sc. in Statistics; M.Sc. in Quality and Production, Six Sigma Black Belt; Statistical consultant for the Fundación Santa Fe de Bogotá (FSFB) University Hospital.
Author contribution
Authorship has been granted only to those individuals who contributed substantially to the research or paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.