
Abstract
Introduction:
The mortality of patients with neck-of-femur (NOF) fractures remains high, with increasing recognition of a subgroup of patients with predictable mortality. The role of palliative care in this group is poorly understood and underdeveloped. This research aims to investigate current clinician attitudes toward palliative care for patients with NOF fracture, and explore processes in place for early identification for patients nearing the end of life.
Materials and Methods:
An online survey was constructed with reference to National Institute for Health and Clinical Excellence end-of-life guidelines (CG13) and distributed to multidisciplinary teams involved in the care of NOF fracture patients in 4 hospitals of contrasting size and location in the United Kingdom.
Results:
Forty health-care professionals with a broad range of seniority and roles responded. The palliative care team was felt to have several potential roles in the care of NOF fracture patients, but there was difference of opinion between specialties about what these were. A number of barriers to palliative referral were identified, including stigma and active surgical management. The majority (75%) felt that all NOF fracture patients should have a discussion about ceiling of care, with difference of opinion about who should do so, and when.
Discussion:
As the elderly population has grown, so too has the volume of NOF fracture patients. It is increasingly important to identify and escalate patients who have poor prognosis following hip fracture and ensure they benefit from palliative care where appropriate. This survey demonstrates a barrier to addressing the care of these patients and a lack of consensus on identification and referral to appropriate palliative care planning.
Conclusions:
There should be close communication between specialties with regard to requirements for palliative care in NOF fracture patients, with ongoing education and clear local and national guidance to ensure they receive the right care at the right time.
Introduction
Neck-of-femur (NOF) fractures continue to be a common reason for admission to all orthopedic units, with over 75 000 such injuries sustained annually in the United Kingdom. 1 Patients who sustain these injuries are often elderly, and have significant comorbidities, requiring complex care by a multidisciplinary team (MDT). As a result, the average length of inpatient stay per patient admission is 21.6 days with an estimated health and social care bill of over 1 billion pounds in the United Kingdom. 2 The morbidity and mortality of patients with these injuries is well documented and the 1-year mortality rate remains around 30%. 2 With an aging population, the scale of this problem is likely to continue growing.
Given these alarming statistics, there has been a concerted national effort to improve management of these patients. The introduction of the National Hip Fracture Database in 2007 allowed the collection and reporting of important data regarding NOF fractures from 177 hospitals, encompassing 65 645 patients in the latest report in 2017. 2 Following the evidence generated by this database, a “Best Practice Tariff” was introduced in 2012, which provided financial incentives to hospital trusts to provide optimum care for patients with NOF fracture. This includes early surgery, physiotherapy and orthogeriatric review, as well as bone health and falls assessment, and thorough documentation of cognition.
These measures, among others, have begun to show benefit, with the 30-day mortality improving from 10.9% in 2007 to 6.7% in 2016. 2 However, the rate of improvement has reached a plateau, and evidence now suggests there is a subgroup of patients who, due to comorbidity and frailty prior to their injury, are likely to have poor outcomes and mortality despite recent improvements in care. 3,4 Research from our center sought to assess this group of patients retrospectively and found that of the 1033 NOF fracture patients admitted over a 2-year period, 74 died as inpatients. Of the 74 deaths, it was felt that 42% were predictable by orthogeriatricians using risk factors on admission and a further 40% were predictable following an acute deterioration. These patients died in hospital, contrary to most patients’ preference to die at home, 5 having received an average of 28 blood tests, 6.8 X-rays and computed tomographies, and 33% of them never received formal end-of-life supportive care. 3 This research has led us to explore the potential role of palliative care for this patient group.
The role of palliative care is well established in the treatment of patients with cancer. 6 Furthermore, palliative care has increasingly been integrated into the management of diseases such as chronic cardiac failure, chronic obstructive pulmonary disease, and diabetes, with improved quality of life and symptom control. 7,8
Despite NOF fractures being common and carrying a similar morbidity and mortality to some cancers, there is little research regarding palliation of NOF fracture patients, and we were unable to find any evidence of targeted palliative care plans for them in the literature. Furthermore, national guidelines, while mentioning the need to consider surgery for palliative purposes, do not explicitly mention the role of palliative care. 9,10
This research aims to gain a deeper understanding of current attitudes and approaches to palliative care of NOF fracture patients, by surveying members of the MDT involved in their care, across National Health Service (NHS) hospitals of contrasting sizes in different areas of the United Kingdom.
Materials and Methods
The coordinating team for this survey was based in Southmead NHS Hospital, Bristol, United Kingdom. The proposal was submitted to the local audit and research department who confirmed ethical approval was not required as no patients were directly involved. All survey respondents provided written consent including for the use of anonymized quotations.
Questionnaire/Survey
Questions were formulated to provide useful information about the role of responders, referral systems, attitudes, and responsibilities with regard to palliation of NOF fracture patients using a combination of multiple-choice questions and free-text comment boxes (see Appendix A). Questions were designed to reflect key statements in the National Institute for Health and Clinical Excellence (NICE) guidance for end-of-life care for adults. 11 National Institute for Health and Clinical Excellence provides guidance for United Kingdom health-care providers for a wide range of clinical and social topics.
Questions were distributed via an online questionnaire survey, with answers being confidential and anonymous. The survey took place between February 22, 2018, and September 22, 2018.
Selection of Participating Hospitals
To provide a range of perspectives, we surveyed 4 NHS hospitals. To provide comparison between areas, this included 2 hospitals from south-west England, and 2 hospitals from the London area. In each area, a smaller district general hospital (DGH) and a larger major trauma center (MTC) in order to identify any differences in practice between hospitals of varying sizes. Hospital names have been withheld to ensure anonymity.
The questionnaire was distributed by e-mail to members of the MDT involved with care of NOF fractures. Responses were received via a password protected online platform by the study lead and analyzed.
Results
General Frequency of Response
From the 67 people asked, 40 people responded, representing a 60% response rate. Of these, 25 were from MTCs and 15 from DGHs, from a broad range of specialties and seniority (see Table 1).
Frequency of Response by Health-Care Professional (Divided by Hospital Site).a
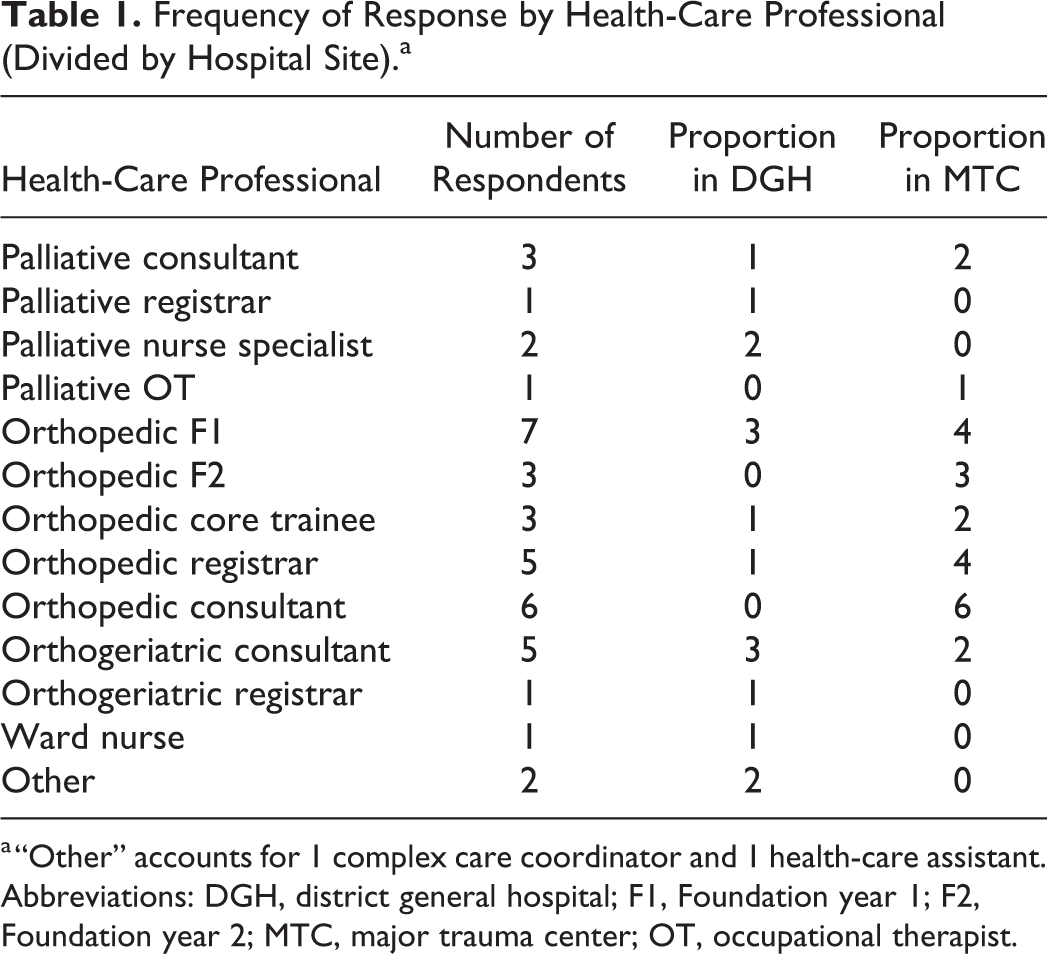
a “Other” accounts for 1 complex care coordinator and 1 health-care assistant.
Abbreviations: DGH, district general hospital; F1, Foundation year 1; F2, Foundation year 2; MTC, major trauma center; OT, occupational therapist.
Practicalities: Access to Palliative Care
The majority (63%) of clinicians felt able to access palliative care, even at night, although 22% were still unsure, with the majority (5/6) of people in one hospital unsure if they had access to specialist palliative care advice out of hours. Free text indicated that in all centers advice was sought either through the palliative consultant on call or via the local hospice.
Identifying NOF Fracture Patients With Palliative Needs
When asked about perceived palliative care needs of orthopedic patients, free-text answers were grouped around common themes; the frequency with which each theme was mentioned is detailed in Figure 1.

Multidisciplinary team perceptions about what palliative care needs their orthopedic patients have. “Other” accounts for 1 complex care coordinator and 1 health-care assistant.
If broken down by hospital, or by hospital size, the answers were similar. However, answers commonly given by palliative and orthopedic teams were different (see Figure 2).

Stacked bar chart showing frequency of reference to common themes divided by specialty.
The orthopedic teams largely saw the most important roles of the palliative team being symptom management, communication with patient or family, and managing complex patients with multiple comorbidities:
“Palliative care can help with pain relief, symptomatic management, in patients who quickly decline with multiple comorbidities”. (Orthopedic consultant, site 1)
Although the palliative team responses included most of these, they more frequently referenced the role of advance care and discharge planning:
“The palliative care can help manage expectations and make practical plans when a patient deteriorates.” (Palliative consultant, site 1)
Junior doctors were more likely to state that symptom control and patients nearing end of life as reasons for referring to palliative care. In contrast, consultants were more likely to mention communication with patient/family advance care planning and nonoperative management of NOF fractures.
Advance Care Planning in NOF Fracture Patients
There was considerable variability in responses about the most appropriate time frame for putting in place escalation of care plans (see Figure 3).

Multidisciplinary team opinion as to when escalation of care plans should be put in place for orthopedic patients.
All responding orthogeriatricians felt escalation of care plans should be put in place either on admission or within 72 hours of admission:
“Certainly I feel it would be beneficial to discuss escalation and end of life care decision with all patients on admission.” (Orthogeriatric consultant, site 2)
Answers from other teams were variable, with 7 people feeling that this was variable depending on the patient, or on call team. Thirty people responded that all NOF fracture patients should have a discussion about escalation of care. Ten stated that all patients with significant comorbidity should have this discussion, with 5 respondents mentioning an age cut off. The majority of respondents felt at least a Foundation year 2 (F2) doctor or above should be having these discussions with patients, with only 1 person feeling that it should be a consultant.
Perceived Barriers to Referral of NOF Fracture Patients to Palliative Care
A number of common themes emerged in response to potential barriers for referral of NOF fracture patients to palliative care. From the palliative care team, the most common concern was that orthopedic doctors might not fully understand what services palliative care offers or how to refer patients. Of note, 25% of orthopedic respondents felt that that presentation for surgery with an acute injury was a barrier to recognizing the need for palliative care:
“The expectation after they’ve just have surgery is to give full escalation and resuscitation.” (Orthopedic core trainee, site 3)
There was also concern from 4 orthopedic team members and 1 palliative care team member that the stigma associated with a palliative referral may upset the family or patient.
Neck-of-Femur Fracture Surgery in Palliative Patients
The majority of respondents across all specialties felt there was no specific life expectancy limiting operative management of NOF fracture patients, with 16 suggesting their decision was dependent on patient pain, another 10 based their decision on patient frailty/comorbidity:
“Surgery is best for most patients in pain however individual patients factors must be considered in each case.” (Orthopedic consultant, site 2)
Of the 19 people who offered a suggested time frame, 5 felt a life expectancy of less than 48 hours was inappropriate for surgery, 7 felt less than 1 week, 3 felt less than 2 weeks, 2 felt less than 4 weeks, and 2 felt less than 3 months.
Continuing Care
With regard to the question on handover, the majority (58%) of responders suggested using discharge summaries (23 people), with 5 (13%) saying they would also phone the patient’s general practitioner (GP). Four said they would phone the community palliative care team. Ten people, however, commented that they would use a combination, or as many options as possible, particularly in the more complex or more end-of-life patients. Members of the palliative team were more likely to use multiple methods of handover to the community, and there was again little variation between hospitals.
Discussion
Main Findings/Results
Opinions about provision of palliative care for NOF fracture patients were varied in this survey; however, the majority (68%) of respondents felt that they could access specialist palliative care advice for orthopedic patients out of hours. There remain, however, a significant number of clinicians who were unsure, or who felt they could not, which may indicate a need for education or awareness.
The role of palliative care can be wide reaching and insight into perceptions about the role of palliative care for different patients can be a useful aid to improving understanding and cooperation between care teams. 12 The most commonly referenced role in this survey was symptom or pain management (see Figure 3), particularly among members of the orthopedic team. Palliative team members’ responses suggested they perceived their role was more focused on advance care and discharge planning. This difference in the perception of roles may result in a lack of referral to palliative care, or inappropriate referral for patients with little to gain from it. A clearer understanding of the role of palliative team members and appropriate referral guidelines for patients, as well as inclusive MDT meetings would improve more efficient and appropriate use of palliative care services for NOF fracture patients. Responses from more junior members of the MDT indicated a lack of confidence with symptom control, which could be rectified with greater teaching on the role of palliative care teams and appropriate escalation.
A key part of palliative care is early recognition of patients requiring palliative input and advance care planning. 4 Advance care planning involves helping patients to choose the best management options in the context of prognosis, available treatments, and best interests. In other countries such as the Unites States, the same discussions are termed “goals of care.” There was a wide variation in the opinions of responders about the timing of these discussions. Twenty-eight percent suggested at admission, 30% within 72 hours, and 20% suggested after an acute deterioration (see Figure 3). Seventeen percent were not willing to commit to a particular time frame, preferring to judge this on a patient-to-patient basis. This wide variation in practice could lead to confusion, especially among admitting junior doctors. Local clarification about creating escalation-of-care documents and development of protocols could improve planning and early discussions with patients and family. Previous studies suggest that some doctors avoid these discussions for fear they would upset or anger relatives/patients. 13 However, our study suggests palliative care and orthogeriatricians favor early discussion and documentation of escalation plans in order to address and overcome these concerns.
There was a strong consensus among survey respondents that all NOF fracture patients should be engaged in discussions about resuscitation and Do Not Attempt Cardiopulmonary Resuscitation (DNACPR) forms. Three-quarters of respondents felt this should apply to all NOF fracture admissions, with the remaining quarter adding a caveat that the patient should be either comorbid or older than 60 years. Again, a unified local policy on which patients should have a DNACPR discussion may prevent confusion, promote consistent practice, and provide clarity in the case a patient declines later in their admission. The grade of doctor responsible for this discussion provoked a wide range of answers. Most respondents felt it should be at least an F2 doctor; however, 15% would accept a Foundation year 1 (F1) doctor. National guidance from the General Medical Council does not explicitly mention what grade of doctor should initiate DNACPR discussions. 14 The United Kingdom Resuscitation Council guidance suggests that overall responsibility for these decisions lies with the consultant in charge of the patient’s care and that an F1 doctor should not be signing DNACPR forms legally. 15 This is in stark contrast with the findings of our survey where only 1 respondent felt a consultant should be having the DNACPR discussions and 6 felt it was appropriate for an F1 to have this discussion.
Improvements and clarity of national guidelines could result in more patients having these discussions, at the right time by the right grade of doctor and prevent potential medico-legal ramifications of failure to initiate and document these discussions appropriately. 16
Reassuringly, the majority of respondents felt there were no barriers to referring NOF fracture patients to palliative care. A number of orthopedic respondents felt that the stigma or negative connotations of referral to palliative care might be a barrier to referral. Furthermore, they raised the possibility that the surgical management of these patients may confuse the picture for these patients. It is important for all members of the NOF fracture patients’ clinical care team to be aware that NOF fracture surgery can be a palliative procedure and that referral to palliative care should not be seen as a failure of active management, but an adjunct to holistic care.
The NICE guidance on hip fragility fractures does mention the need to consider surgery as a palliative measure, 9 but selection of patients for nonoperative management remains at the discretion of clinicians. Surgery remains the mainstay in the majority of NOF fracture patients. What little research has been done into nonoperative management suggests worse mortality and morbidity. 17 Respondents in the survey suggested the decision to proceed to surgery was made on a patient-by-patient basis, with many feeling that pain and comorbidity were more important factors than life expectancy. For those offering a numeric life expectancy under which they felt surgery was not justified, there was a range of answers from less than 48 hours to less than 6 months. This is a significant range of time and opinion, which may lead to confusion and lack of cohesion between members of the MDT when making decisions about patients. Clearly though it is important to make these decisions on a patient-by-patient basis, the variety of answers highlights the need for clear communication and decision-making between MDT members.
Continuity of care following discharge home is especially important for patients with palliative needs, so it was relevant to poll opinion about how care should be communicated to the community health-care teams. Most respondents stated they would use discharge summaries (58%), but the majority of palliative care team members said they would prefer to use more than 1 modality, including a phone call to the patient’s GP or community palliative care team. This may reflect a better understanding of the nature of community care by members of the palliative team and emphasizes the importance of clearly delegating responsibility for handover of care within hospitals.
Strengths/Limitations
A strength of this survey was that it was distributed to multiple centers of varying size and location in the United Kingdom. Although this enables a better understanding of variability in opinions and practice across NHS hospitals in the United Kingdom, it does not necessarily allow for generalizability as only 4 hospitals were involved, this may be helped in future research by involving hospitals in different geographical regions and collecting more information about the palliative care setup and referrals system in each hospital, which can be variable across different United Kingdom hospitals. Our short survey was designed so that it took minimal time to complete ensuring a greater response. Our main aim was to gain an understanding of clinician attitudes toward palliative care for NOF fracture patients. We achieved this finding a wide variation in opinion across MDTs and hospitals. This suggests further in-depth research is required to understand the complexities of these variations.
Conclusion
The responses to this survey cover a range of important areas regarding palliative care for NOF fracture patients and reveal areas for improvement around advance care planning and communication and identification of patients with palliative care needs. To ensure optimal and holistic care for these complex patients, members of the MDT must work closely together, with communication and education being key to improving care, which includes the better integration of palliative care services. Increasingly, there should be a culture of early recognition and escalation to palliative care of patients with NOF fracture reaching the end of life, so that they receive the best care, at the right time.
Footnotes
Appendix A
Authors’ Note
There was no direct involvement of patients in the study. This research was discussed with the local research and audit department, who agreed formal ethical approval was not required for a study of this design that does not directly involve patients or influence their treatment.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.