Abstract
Introduction
Hip fractures are common among older adults; and while urgent fracture fixation is recommended, it is often weighed against preoperative optimization needs. Previous studies have reported conflicting findings on the association between time to surgery and mortality risk. In this study, we investigated the association between surgical timing and mortality. We also explored the relationship between time to surgery and secondary outcomes, including length of stay and hospital readmission.
Methods
We conducted a retrospective cross-sectional study of 967 adults aged
Results
For 30-day, 90-day, and 365-day mortality, each additional day of delay in surgery was associated with an increased risk of mortality, with adjusted hazard ratios (HR) of 1.15 (95% CI [1.02, 1.30], P = .02), 1.13 (95% CI [1.02, 1.26], P = .02), and 1.09 (95% CI [1.01, 1.19], P = .03), respectively. Similarly, each additional day of delay was associated with an increased risk of a length of stay >7 days and readmission within 30 days of discharge, with adjusted odds ratios (OR) of 2.26 (95% CI [1.89, 2.74]) and 1.16 (95% CI [1.05, 1.29]), respectively.
Conclusion
Delaying surgery in older adults increases the risk of mortality, along with a potential elevated risk of prolonged hospital stays and readmission. We recommend that, when safe, surgery should be performed promptly for these patients.
Introduction
Older adults suffering ground level falls and subsequent hip fracture are common presentations to emergency departments across the country. 1 These hip fractures carry high mortality with more than one–third dying within 12 months according to some estimates.2-4 These injuries also carry high morbidity with only a fraction of this population regaining their baseline functional status, often impacting their independence and ability to live in the community. 5 In a recent American Academy of Orthopedic Surgeons (AAOS) Clinical Practice Guideline, prompt surgical fixation is cited as a main strategy to reduce mortality. 6 Another meta-analysis also found an association between early surgery and survival after 1 year of surgery in support of this school of thought. 7
Debate remains over the definition of “prompt” or “early” surgery. One retrospective study found that a surgery delay of more than 12 h increased the odds of mortality within 30 days of surgery, while a delay of more than 24 h increased the odds of 90-day mortality. 8 Another meta-analysis found that a delay of more than 48 h increased the odds of mortality significantly at 30 days and 1 year from surgery. 9
Older adults often carry multiple comorbidities that can contribute to complicated preoperative assessments and needs for medical optimization that can impact time to surgery. Patients requiring medical optimization due to pre-existing medical conditions had elevated risk of mortality within 30 days of surgery, according to 1 study. 3 This may speak to the fact that older adults are living longer, often with more chronic comorbid disease burden, elevating their surgical risk.
We embarked on this study to better examine the association between the timing of hip fracture repair surgery and mortality, length of hospital stay and readmission within 30 days of discharge among an older adult population admitted to a single-site urban academic center.
Methods and Materials
Patient Selection
Due to the use of de-identified patient records posing minimal risk, the institution’s Committee on Clinical Investigations approved this research as exempt on 02/08/2023 (Protocol # 2023P000072). Using a cross-sectional study design, we conducted a retrospective chart review of our hospital surgical records from January 1, 2018, to January 1, 2023, identifying 53 232 patients who underwent surgery. We excluded 30 220 patients based on age (<65 years) at surgical encounter. Of the remaining 23 012 older adult patients, a further 22 044 were excluded for non-hip fracture surgeries. Hip fractures were defined using ICD-10 codes S72.012, S72.21, and S72.141. Surgical fixation included total or hemiarthroplasty, open reduction and internal fixation (ORIF) with gamma nail, trochanteric fixation nailing (TFN) system, percutaneous cannulated screws, dynamic hip screw (DHS) system, and gouffon pinning. We followed the STROBE Guidelines for the preparation of this manuscript. Figure 1 displays the flowchart for the analytic sample selection.
Study Variables
In our study, the time to surgery (in days) was defined as the interval between the patient’s presentation to our hospital (ED arrival or direct admission) and the start of the operative hip fracture fixation procedure. The primary outcome was time to mortality, measured as time to death from hospital discharge, assessed at 30 days, 90 days, and 365 days. Secondary outcomes included length of stay (LOS) exceeding 7 days and 30-day readmission for any cause. We collected demographic data for all participants, including age, sex, race, and ethnicity, along with additional covariates such as the American Society of Anesthesiologists (ASA) score and frailty index (FI) score, both of which were included in the analysis model.
Statistical Analyses
Demographic Characteristics of Study Participants

We assumed independent censoring in the time-to-event analysis. For the primary outcomes—30-day, 90-day, and 365-day mortality—patients who survived beyond 30 day, 90 day and 365 day after discharge were censored at 30, 90, and 365 days, respectively. We presented Kaplan-Meier curves for 30-day, 90-day, and 365-day mortality, stratified by quartiles of time to surgery in Figures 2-–4 (please see appendix) and conducted log-rank tests to examine association between time to mortality and discretized time to surgery. To assess the association between time to surgery and these primary outcomes, we used multivariate Cox proportional hazards models, adjusting for age, gender, race, ASA score, admission through the ED and frailty score. Hazard ratios (HRs), 95% confidence intervals (CIs), and associated P-values are reported.
To examine the association between secondary outcomes and time to surgery, and to address potential separation due to missing frailty index (FI) data, we employed a Firth penalized logistic regression model. This model was adjusted for age, gender, race, ASA score, ED admission, frailty index and indication of missing frailty index. We reported odds ratios (ORs) with 95% confidence intervals (CIs) and P-values.
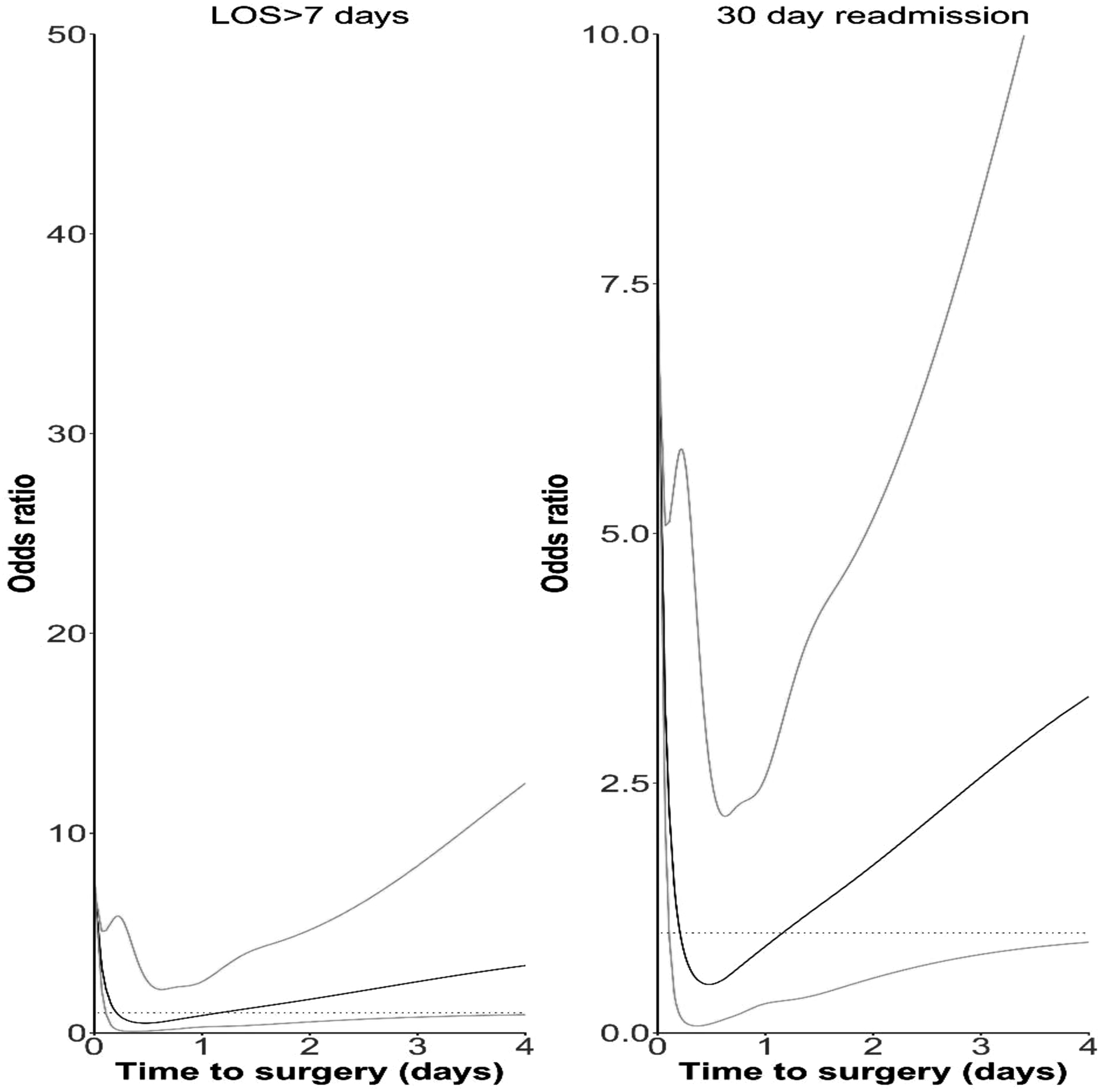
Finally, considering the possibility of non-linear effects of time to surgery, we conducted sensitivity analyses by repeating above analyses. In those analyses, we replaced time to surgery by B-spline transformation of time to surgery with 5 knots fixed at 0th, 25th, 50th, 75th and 100th percentile. For primary outcomes and secondary outcomes, we plotted the associated relative death rate and the associated odds ratio over time to surgery by setting 1.02-day time to surgery as the reference, which is the median of time to surgery.
We considered P < .05 as statistically significant and all P-values were two-sided. All statistical analyses were performed using R Statistical Software (version 4.2.2; R Foundation for Statistical Computing, Vienna, Austria).
Results
Our analytic sample consisted of 967 patients, with a median age of 84 years (IQR 77.00, 90.00). There were 326 men (33.7%) and most patients identified as white (86.1%). 696 patients, representing 72.0% of the total sample size, had an ASA score of 3, and we had a median frailty index score of 0.36 (IQR 0.22, 0.46). The medians values for time to surgery and length of stay were 1.02 days and 5 days respectively, with 118 patients (12.2%) readmitted within 30 days of hospital discharge. Furthermore, 22 patients (2.3%) developed deep venous thrombosis while 17 patients (1.8%) developed pulmonary embolism. In Table 1, we presented analytic sample population characteristics.
Primary Outcomes
Figures 2-4 display Kaplan-Meier curves for primary outcomes stratified by quartiles of time to surgery. The quartiles are defined as follows: first quartile (Q1) [0, 0.713] days, second quartile (Q2) (0.713, 1.02] days, third quartile (Q3) (1.02, 1.71] days, and fourth quartile (Q4) (1.71, 18.3] days. For all primary outcomes, patients with longer times to surgery exhibited a higher risk of mortality. Log-rank tests revealed that patients in higher quartiles of time to surgery had increased mortality risk at 30 days, 90 days, and 365 days after discharge (P = .002, P < .001, and P < .001, respectively).
Hazard Ratios (HRs), Associated 95% Confidence Intervals (CIs), and Two-Sided P-Values From Multivariable-Adjusted Cox Proportional Hazards Models for the Association Between Time to Surgery and 30-Day, 90-Day, and 365-Day Mortality

Secondary Outcomes
Association Between Time-To-Surgery and LOS>7 Days and 30-Day Readmission

In a similar fashion, sensitivity analyses (Figure 6) suggested possible non-linear effects of time to surgery on 30-day readmission.
Discussion
In this study, we evaluated the association between time to surgery and 30-day mortality, 90-day mortality and 365-day mortality as primary outcomes, finding that delay to surgery was significantly associated with 15%, 13% and 9% higher risk of mortality, respectively. Secondary outcomes—length of stay >7 days and 30-day readmission— were also examined with respect to their association with time to surgery and we found a higher odds of longer length of stay and 30-day readmissions with longer time to surgery.
Other studies have similar results. In a study of 269 patients over 50 years old undergoing hip fracture surgery, 10 there was a significant association between time to surgery and mortality at 1 year after the surgery. Similarly, in a study among patients aged 85 or above, it was found that surgery to repair hip fractures done within 48-72 h was associated with a lower prevalence of mortality at 30 days and 1 year after surgery compared to surgery done after 72 h. 11 Lieten et al 12 found a lower prevalence of mortality among patients who had hip fracture surgery done within 24 h (early) compared to those who had surgery after 24 h (late). Fenwick et al 13 found significant decrease in mortality when comparing a group that had surgery within 48 h to those who had surgery after 48 h.
Not all previously done studies agree with our findings. One recent retrospective study carried out among 194 patients undergoing hip fracture surgery found no significant differences in 1-year mortality between those who had surgery within 48 h and those who did between 48-96 h, 14 finding instead that ASA score was better correlated as a predictor of mortality.
Prolonged hospital stay resulting from a delay to surgery may expose to the risk of developing hospital acquired-infections and other complications,15,16 leading to a longer overall hospital stay and readmission, and may partly explain our secondary outcome findings. In 1 study among patients who were 65 years and older at the time of surgery, a longer average length of stay was associated with longer time to surgery. 17 Another study that supports our finding was by Liu et al 18 in a study of over 200 000 patients who underwent hemiarthroplasty for hip fractures. They found a shorter length of stay and fewer complications with early surgery compared with delayed surgery with the results being statistically significant. Similarly, Murphy et al 19 found a lower average length of hospital stay when patients had hip fracture repair surgery within 48hours of surgery compared to when they had surgery after 48 h. Likewise, in a study among 701 older adults aged 65 years and above, Sun et al 20 found that patients who had surgery within 48 h of hospital admission had a statistically significant lower odds of being readmitted to the hospital within 30 days of discharge compared to those who had their surgery after 48 h.
This study, to the best of our knowledge, is one of the first studies in recent times with a relatively large cohort carried out to assess the association between timing of surgery and mortality following hip fractures among the older adult population, most of whom are moderately-severely frail, to include the frailty index in the analysis. The frailty index has been shown in literature to be a strong predictor of mortality,21,22 and is regarded by some to be a stronger predictor of mortality than age or injury severity alone,23,24 making the inclusion of this variable in our analysis of utmost importance. While we did not collect data on co-morbidities for each study participant, we utilized the ASA score as a surrogate variable for co-morbidity. As shown in Table 1, 86.4% of our study population had an ASA score greater or equal to 3, reflecting a significantly co-morbid population. This is contrasted with a recent study of 905 hip fracture patients under 50 years where 83% of the study population had ASA scores equal to or less than 2. 25
This study was not without limitations. Firstly, because we relied on hospital data alone to obtain records of mortality in the study participants, we may have inadvertently underestimated mortality as some deaths are not reported at all or in a timely fashion and are thus not captured in this study. Second, our hospital is a quaternary medical facility, providing care for the sickest patients and receiving patients referred from other facilities. Thus, our sample size may be biased to reflect a frailer or co-morbid population compared to a random selection of older adults with hip fractures. Although we adjusted for ASA score and frailty index, we lacked detailed data on individual comorbidities. Therefore, residual confounding by unmeasured or inadequately captured comorbidities remains possible. In addition, because we could not distinguish whether surgical delays were due to clinical optimization needs or organizational factors, the observed associations may reflect system-level delays rather than patient’s clinical need for delays. This is a single site study and thus, misses out on a more diverse and representative study population that may have been obtained with a multi-site study. Furthermore, this study lacked a formal power analysis for sample size calculation. As such, the study may be underpowered to detect small but potentially meaningful differences. Finally, the retrospective nature of this study left us with a limited number of variables to include in the analysis; in addition to some of the variables being missing for some study participants.
Conclusion
Determination of the optimal time of surgery is challenging for older adults with hip fractures who require surgery. There are variations in institutional practices, and these are further complicated by administrative delays. Another infrequently acknowledged challenge relates to delayed hospital presentation; as some of these patients are injured hours before they can reach or call for help and are brought to the hospital.
Our results show that a longer time to surgery is associated with a higher risk of mortality at all 3 time intervals examined. We also found in a sensitivity analysis, that this effect may be non-linear. For our secondary outcomes, we found that earlier fracture fixation is associated with a lower odd of readmission within 30 days and longer length of stay. These findings suggest that when safe, surgery should be done as soon as feasible for these patients.
The orthogeriatric multidisciplinary management model has been adopted by our institution and many other institutions with a widely-reported positive impact on healthcare outcomes of these individuals.26-28 By utilizing this, we have minimized delays and streamlined clinical decision making pathways with most remaining delays in definitive fixation of hip fractures for older adults being logistical or administrative in nature. This model facilitates earlier surgery by ensuring prompt communication between different teams and clear transmission of goals and targets of care for each individual; and we recommend that this model be adopted where possible to optimize care.
Footnotes
Acknowledgements
This research has had an abstract presented at the Beth Israel Deaconess Medical Center Research Retreat that took place on September 5, 2024.
Ethical Considerations
Due to the use of de-identified patient records posing minimal risk, the Beth Israel Deaconess Medical Center Committee on Clinical Investigations approved this research as exempt on 02/08/2023 (Protocol # 2023P000072).
Author Contributions
All listed authors made substantial contributions to the study design and conceptualization, and participated fully in the drafting, multiple reviews and approval of the final manuscript. CZ performed formal analysis, MA, DR, NA, CZ, MM, CD, ER, KC and DO were responsible for the methodology and data acquisition. MA, DR, AS, NA, CZ, MM, CD, JW, KAH, PA, ER, KC, DO contributed to manuscript writing, editing and review.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data Availability Statement
The dataset generated during and analyzed during the current study are available from the authors on reasonable request.
Appendix
Flowchart for the Analytic Sample Selection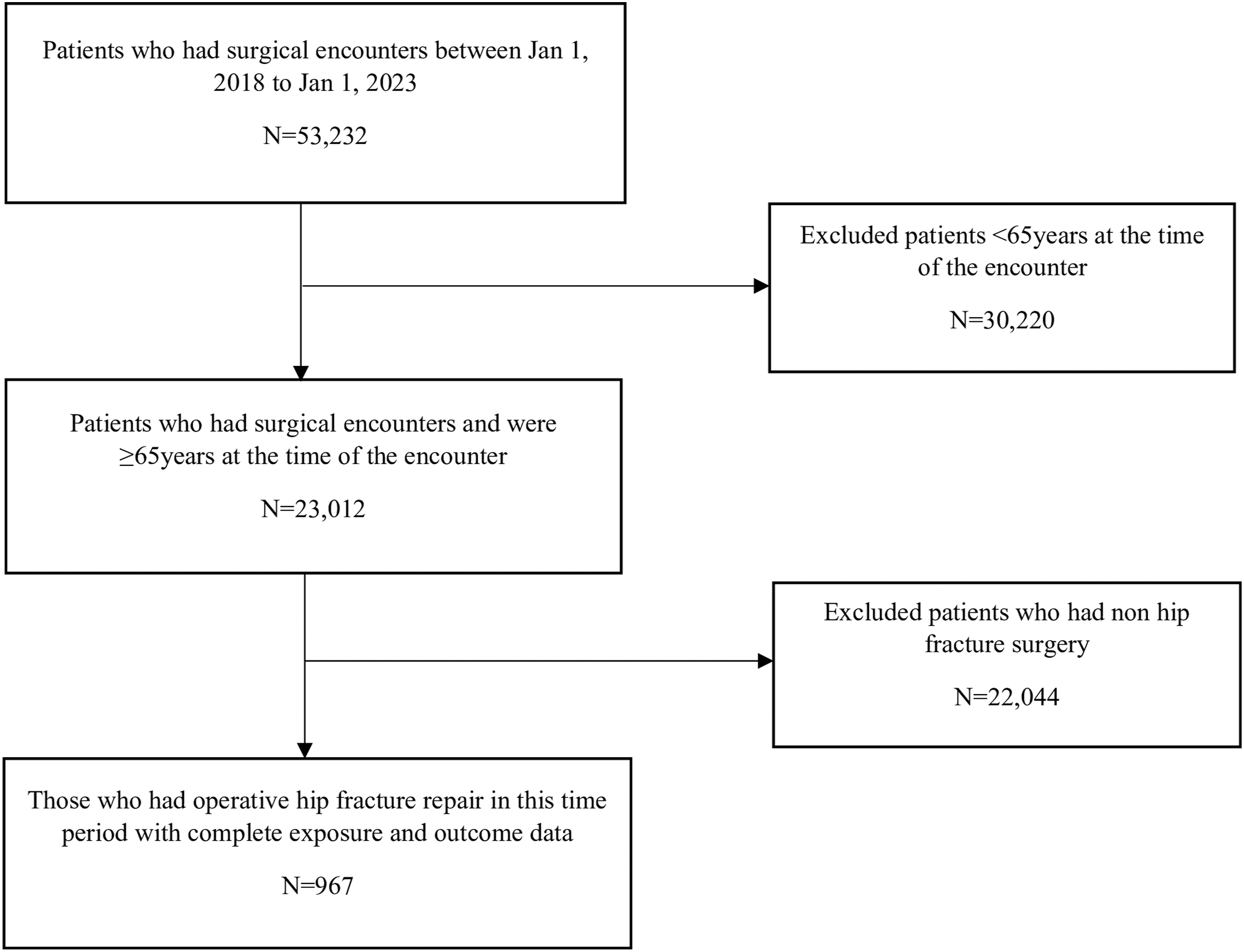
Kaplan-Meier Curves for 30-Day Mortality With Associated Two-Sided P-Value From Log-Rank Test (P = .0019)
Kaplan-Meier Curves for 90-Day Mortality With Associated Two-Sided P-Value Obtained From Log-Rank Tests (P = .0003)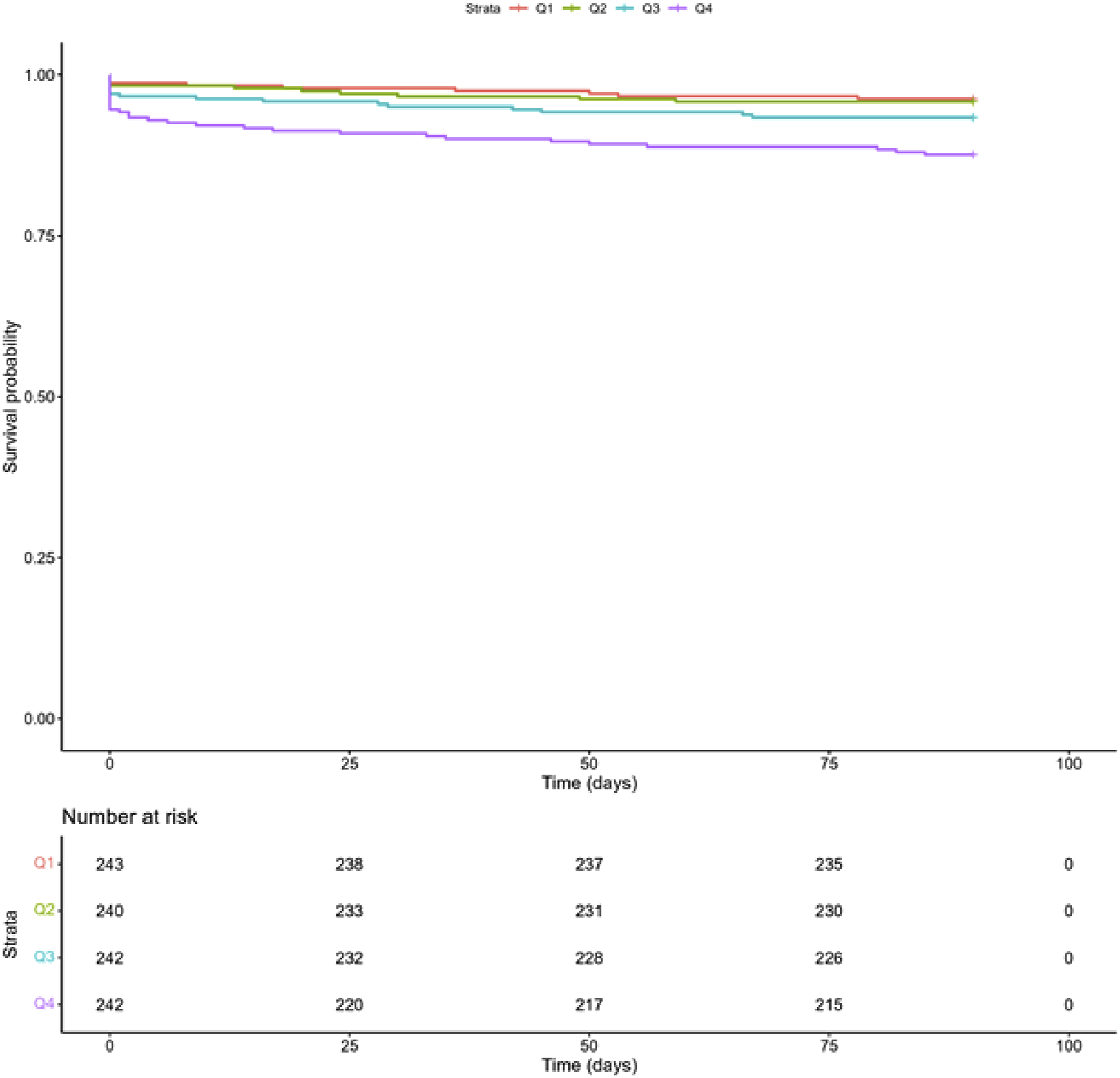
Kaplan-Meier Curves for 365-Day Mortality With Associated Two-Sided P-Value Obtained From Log-Rank Tests (P = .0002)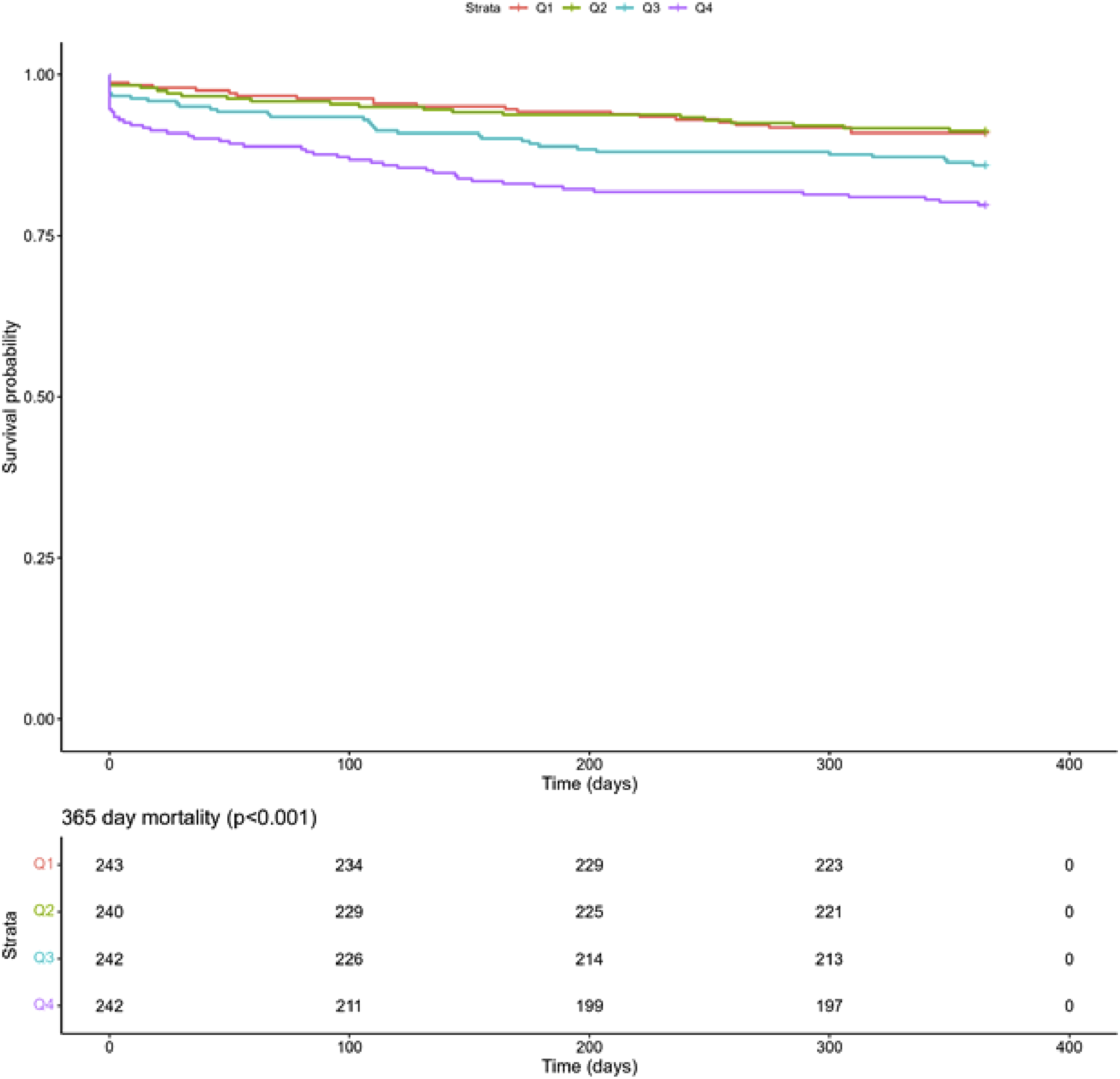
Sensitivity Analysis to Assess Non-Linearity of Exposure and Primary Outcome
Sensitivity Analysis to Assess Non-Linearity of Exposure and Secondary Outcomes