
Abstract
Objective
The treatment and incidence of femoral neck fracture (FNF) in older patients is controversial. We investigated the new AO (Arbeitsgemeinschaft für Osteosynthese) classification in patients with FNF by age to determine the proportions of stable fracture and change trends according to patients’ age.
Methods
We divided patients with FNF hospitalized in Xi'an Honghui Hospital from 2018 to 2020 into five groups according to age: young (<50 years), middle-aged (50–59 years), young-elderly (60–69 years), middle-elderly (70–79 years), and very elderly (≥80 years) groups. We retrospectively collected data of patients’ sex, admission date, fracture side, mechanism of injury, and new AO classification.
Results
In total, 2071 patients were included for analysis, with 1329 women (64.2%); 1106 patients (53.4%) had left-side fracture. The main mechanism of injury was falling. In the young-elderly, middle-elderly, and very-elderly groups, 33.3%, 29.2%, and 24.1% had stable fracture type, respectively). The proportion of patients with FNF did not show a change trend by age during the 3-year investigation period.
Conclusion
In our study, the proportion of older patients with FNF did not increase, and as many as a third of patients with FNF aged 50 to 70 years had stable fracture.
Introduction
Femoral neck fracture (FNF) is a common clinical proximal femoral fracture with high morbidity and mortality, especially in older people with osteoporosis. 1 Three types of classification are commonly used by surgeons: the Pauwels classification according to the angle of the distal fracture line, the Garden classification according to the displacement type of the fracture, and the anatomical classification according to the location of the fracture line. The previous AO (Arbeitsgemeinschaft für Osteosynthese) classification was infrequently used owing to its complexity and low intra- and interobserver agreement.2,3
Orthopedic surgeons normally use the Garden classification to select the treatment for elderly patients with FNF. Most previous studies comprise elderly patients with displaced FNF, according to the inclusion criteria for hip arthroplasty.4–8 However, the Garden classification is too simple to distinguish some stable or well-vascularized types of FNF. Hospitalized elderly patients with hip fracture usually need interdisciplinary management, and the treatment cost is generally higher than that for other types of fracture.9–11 Patients who are able to choose and decide to undergo hip arthroplasty rather than internal fixation (IF) may not only lose the opportunity to preserve their native hip joint but may also have a large economic burden that is shared by their family and medical insurance institutions. In 2018, the International Comprehensive Classification of Fractures and Dislocations Committee proposed a new classification of FNF, 12 called the new AO classification. This classification combines the Garden and Pauwels classifications but distinguishes the anatomical location of the fracture line, which makes this classification easy to use and facilitates more comprehensive determination of the FNF classification.
The treatment for FNF depends not only on the fracture classification but also on the age and physical condition of the patient.13,14 In younger patients, surgeons usually do not pursue the surgical option of hip replacement. The selection of IF and arthroplasty is mainly between made in patients between age 50 and 70 years, although the appropriate age is controversial.5,15–18 Aging of the Chinese population has gradually increased in recent years. The incidence of FNF in older adults has increased each year according to most epidemiological studies, although these findings are controversial.19–22
In the present study, we aimed to classify FNF according to the new AO classification in different age groups and to determine the proportion of stable fracture in each age group. Our findings can provide a reference for surgeons to rationally differentiate stable FNF in older patients. As a secondary objective, we sought to reveal short-term trends in the age distribution according to the above proportions over a 3-year study period.
Methods
Study design and setting
This single-center, retrospective observational study involved hospitalized patients diagnosed with FNF in the Department of Orthopaedic Trauma, Xi'an Honghui Hospital, from 1 January 2018 to 31 December 2020.
We collected epidemiological data on age, sex, admission date, fracture side, mechanism of injury, and fracture classification. According to the medical records, the mechanism of injury in FNF was categorized as low-energy injury (fall from standing height or lower, sports injury, or fight) and high-energy injury (traffic accident, fall from height higher than 2 meters, blunt force injury, and machine injury.
FNFs were graded according to the new AO classification (Figure 1). Any fracture centered between a line drawn at the distal extent of femoral head articular cartilage and the intertrochanteric line distally was considered an FNF; this is type 31B according to the new AO classification. This type is divided into three groups: 31B1 is subcapital fracture, 31B2 is transcervical fracture, and 31B3 is basicervical fracture. Type 31B1 is divided into three subgroups: type 31B1.1 is valgus-impacted fracture, type 31B1.2 is nondisplaced fracture, and type 31B1.3 is displaced fracture. Type 31B2 is also divided into three subgroups according to Pauwels angle and fragment type in the femoral neck. In this study, we mainly used the Pauwels angle to judge the classification. Type 31B2.1 is simple fracture (Pauwels angle <30°), type 31B2.2 is multifragmentary fracture (Pauwels angle 30°–70°), and type 31B2.3 is shear fracture (Pauwels angle >70°). In this study, we classified types 31B1.1, 31B1.2, 31B2.1, and 31B3 as stable fracture. In the new AO classification, type 2.2 uses 70° rather of 50° as a classification criterion, and stability also depends on the number of fragments; therefore, this subgroup was not included in the stable-fracture type. 23

In the new AO classification, type 31B is femoral neck fracture (FNF). Types 31B1 (subcapital), 31B2 (transcervical), 31B3 (basicervical) represent three different fracture sites. Types 31B1.1 (valgus-impacted), 31B1.2 (nondisplaced), and 31B1.3 (displaced) represent three types of subcapital FNF. Types 31B2.1 (<30°, simple fracture), 31B2.2 (30°–70°, multifragmentary fracture), and 31B2.3 (>70°, shear fracture) represent three types of transcervical FNF. Types 31B1.1, 31B1.2, 31B2.1, and 31B3 are classified as stable fracture.
Patients were divided into five age groups: a young adult group (<50 years old), middle-aged group (50–59 years old), young-elderly group (60–69 years old), middle-elderly group (70–79 years old), and very elderly group (≥80 years old).
Patient selection and data
The inclusion criteria were as follows: (1) fresh FNF; and (2) complete medical records and preoperative X-ray imaging data. The exclusion criteria were: (1) peri-implant, periprosthetic, and pathological fractures; (2) combined with other ipsilateral proximal femoral fracture; and (3) severe hip deformity.
In this study, all imaging data were classified by three attending orthopedic surgeons and two radiologists. Doctors participating in the film reading had received previous training to ensure that they had mastered the classification standards. With two or more differing results, the chief physician held discussions with five other physicians to determine the final classification.
Statistical analysis
Categorical data are presented as number and percentage, and continuous quantitative data are presented as mean ± standard deviation. The authors used IBM SPSS version 25 (IBM Corp., Armonk, NY, USA) to conduct descriptive statistical analysis.
Ethical considerations
This study was approved by the Ethics Committee of Hong Hui Hospital (No. 202208003). Signed informed consent was not required as this study involved review of clinical records and all patient information was de-identified. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 24
Results
A total of 2071 patients were enrolled in this study. The mean patient age was 68.31 ± 15.85 years (range, 16–99 years). The study population included 742 men (35.8%) and 1329 women (64.2%), and the sex ratio was 1:1.79. In total, 1106 patients (53.4%) had left-side fracture and 965 (46.6%) had right-side fracture. Among the total, 1781 patients (86.0%) had low-energy injury and 290 (14.0%) had high-energy injury. The most common mechanism of injury was falling. Among the new AO classifications, type 31B1.3 accounted for the highest proportion (49.4%) with 1023 cases. Type 31B1.2 and 31B2.3 had the lowest proportions (3.3% and 2.9%, respectively)
In a comparison of different age groups, the highest number of patients was found in the very elderly group (n = 600, 29.0%) and the fewest in the young adult group (n = 260, 12.6%). The number of men in the younger age group was much higher than the number of women (n = 177 and n = 83, respectively). However, there were more women in the other age groups, with a female-to-male ratio >2:1 in groups over age 60 years. In all age groups, left-side injury was more common than injury on the right side, and the proportion of patients with low-energy injury was greater than the proportion with high-energy injury. The proportion of patients with low-energy injury increased with increased age (Table 1).
General participant information according to different age groups.

In patients aged <50 years, 31B2.2 accounted for the largest proportion of FNFs (n = 82, 32.7%). Type 31B1.3 (n = 90, 33.1%) and 31B2.2 (n = 85, 31.3%) were the main types in the middle-aged group. Type 31B1.3 was the predominant type in the young-elderly, middle-elderly, and very elderly groups, with 174, 285, and 413 patients (42.5%, 53.8%, and 68.8%), respectively (Table 2). A total of 611 patients (29.5%) had stable fracture. In the young-elderly, middle-elderly, and very-elderly groups, 33.3%, 29.2%, and 24.1% had stable fracture type, respectively).
Distribution of new AO classification in different age groups.
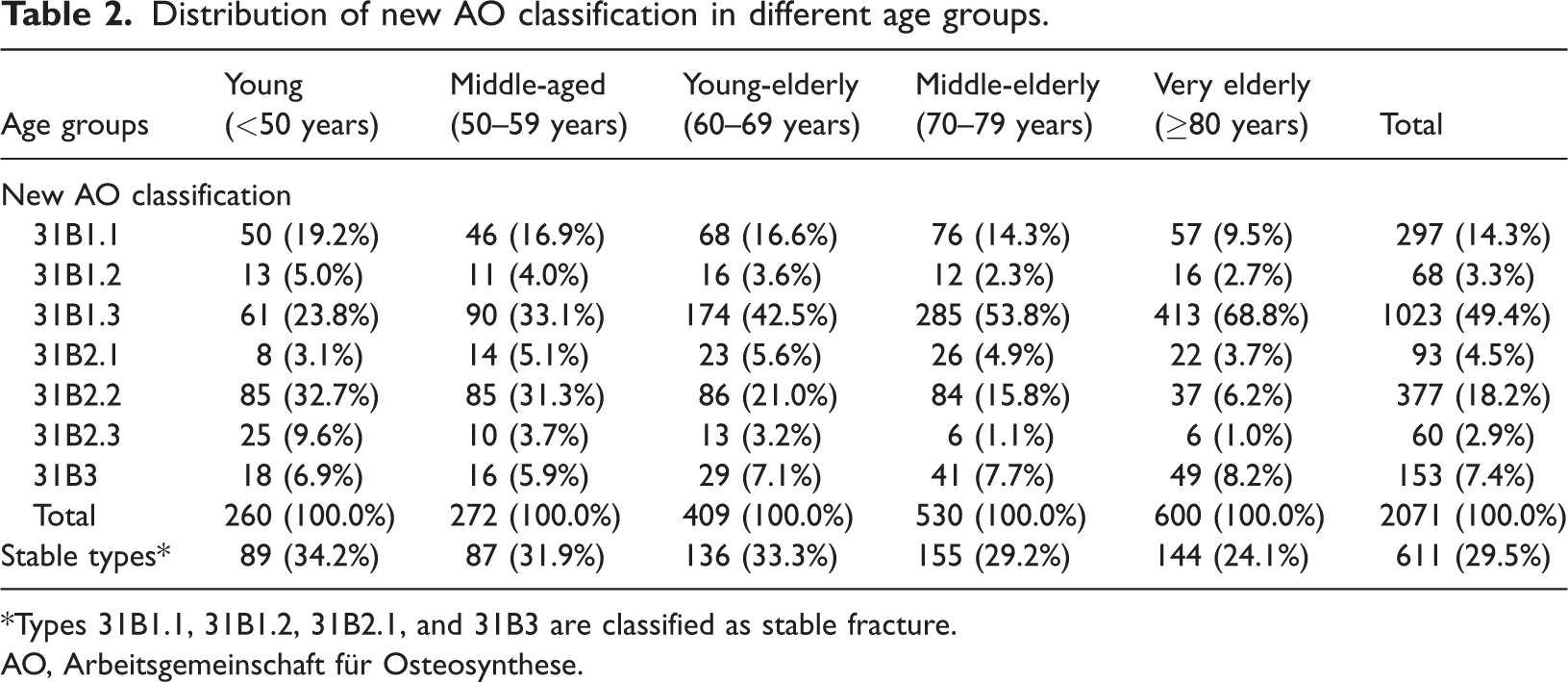
*Types 31B1.1, 31B1.2, 31B2.1, and 31B3 are classified as stable fracture.
AO, Arbeitsgemeinschaft für Osteosynthese.
We identified 719 hospitalized patients in 2018, 694 in 2019, and 661 in 2020. The number of patients showed a decreasing trend each year, and the sex ratio and injury mechanism showed no obvious change trend. The number of patients with FNF decreased each year, but there was no trend in the proportion of patients with FNF in each age group during the 3-year study period (Figure 2).

Proportion of patients in different age groups per year. There was no increase in the proportion of adults aged >60 years, and there was no change trend in the other groups.
Discussion
FNFs are affected by a variety of factors and are generally considered to be closely associated with femoral neck bone mineral density and osteoporosis. In our study, FNFs were more common in women, with an overall sex ratio of 1:1.79; however, in the younger age group, the sex ratio was 2.13:1. This is consistent with previous studies. 25 In investigations of FNF, the main injury mechanism in elderly adults is fall with low energy, and high energy injury is the main cause of FNF in young people.19,25 In our study, the main injury mechanism in all age groups was low-energy injury dominated by fall; high-energy injury accounted for 42.3% of the young adult age group and only 1.2% of the very-elderly group. A large sample survey in Japan found that fall was the injury mechanism in 80% of patients with hip fracture. 19
In recent years, most countries are finding that the incidence of FNF among elderly people is increasing every year.19–21,26 However, in the United States, this trend is experiencing a decline, which may be related to increased safety awareness and promotion of osteoporosis prevention in older adults. In this study, there was no obvious trend in the proportion of patients more than age 60 years. In a comparison over the 3-year study period, no change trend was found regarding the proportion of FNF incidence in each age group.
In previous application of FNF classification, the position of the fracture line is not distinguished, and the classification of FNF is often unclear. Studies on the classification of FNF in recent years indicate that the previous AO classification, Pauwels classification, and Garden classification have interobserver variation, and the inter-observer reliability of AO classification in nine subgroups is low.2,3,27,28 This is mainly because the original AO classification was based on X-ray images and was judged based on patient imaging data. However, the new AO classification combines the above three FNF classifications and distinguishes the location of fracture lines. This results in more detailed FNF classification, increased inter-observer reliability, and more accurate identification of stable femoral neck fracture, such that the surgeon can choose the most appropriate surgical method.
In previous studies of FNF, types 31B1.1, 31B1.2, 31B2.1, and 31B3 were usually considered stable fractures. In 31B1.1, the cortex of the femoral neck is inserted into cancellous bone, and the fracture ends overlap. When the initial valgus and posterior tilts are less than 15°, the risk of IF failure and femoral head necrosis is not high. 29 It is generally difficult to release the insertion state with closed reduction. If the surgeon cannot ensure accurate reduction, fracture type 31B1.1. should be fixed in situ. Types 31B1.1 (valgus-impacted) and 31B1.2 (nondisplaced) were classified as Garden type 2 in previous studies and were primarily treated with IF.30,31 In a study of patients with FNF aged 50 to 60 years, Wang et al. found that those with Pauwels type II had optimal outcomes after successful IF. 32 In a long-term follow-up study of FNF treated with cannulated IF, Ju et al. found that patients aged ≥60 years with Pauwels I and II fractures exhibited a significantly lower necrosis rate than those with Pauwels III fractures, 33 which means that type 31B2.1 and part of 31B2.2 can have good outcomes with IF in elderly patients.
Type 31B3 (basicervical) is closer to the trochanteric region, which has good blood supply and a high probability of healing. Davanzo et al. followed up 154 patients who underwent arthroplasty and 72 patients who underwent IF for basicervical FNF over an average of 4.9 years. 34 There was no difference in terms of survivorship between IF and arthroplasty in the overall population. The incidence of postoperative complications in patients with arthroplasty was higher than that in patients with IF. An observational study of Sundkvist et al. found that among 40,049 FNFs registered in the Swedish Fracture Register, 14 11.6% were basicervical FNF. The treatment of patients over 60 years of age is almost equally divided into IF and arthroplasty. However, Johnson et al. 35 reported that the use of total hip arthroplasty (THA) in the treatment of FNF in patients aged 45 to 64 years increased 4.2-fold from 2002 to 2014. Some of these patients can achieve satisfactory results with only IF. That previous study demonstrates that patients undergoing THA have higher in-hospital complication rates and a longer length of stay than patients undergoing IF. The in-hospital mortality for patients undergoing a hip hemiarthroplasty (HA) is higher (1.2%) than that of either THA (0.2%) or IF (0.5%). Another study reported that HA was associated with poorer health and function outcomes and higher mortality than THA and IF, although no significant difference was found between THA and IF. 36 Elderly patients with nondisplaced FNF who are treated with arthroplasty have a higher 30-day mortality rate (11%), 17 and patients treated with IF have a higher 2-year mortality rate (36%). 16 Several studies have shown that IF may be more cost-effective than hip arthroplasty.11,35,37 Additionally, there are some unique problems after hip arthroplasty to consider, such as metal ion release, ceramic fracture, and noise.38,39
In the present study, between a quarter and a third of patients aged 50 to 70 years had stable fracture. Surgeons may consider preserving the original hip when treating older patients with stable FNF. Patients with fragility fracture or posterior tilt greater than 20° have a high incidence of revision surgery when treated with IF.40–42 When considering IF treatment, the surgeon should focus on the posterior tilt of the FNF and bone mineral density. Although there is a risk of femoral head necrosis with IF treatment, this approach offers the benefits of a biologically intact hip. In elderly people with an appropriate fracture type, it is important for doctors to choose IF to preserve the native hip joint. Rigorous and accurate classification of FNF prior to surgery is important to reduce reoperation rates in the elderly population treated with IF.
The study limitations include the short study period, which made it difficult to determine age-related change trends. Additionally, the sample size and single-center analysis were not representative of the entire region. The new AO classification is more detailed, with seven subgroups. However, no studies have evaluated the interobserver reliability in radiographic determination; this must be addressed in future research. Future studies should focus on older patients with stable FNF aged 50 to 70 years who are treated with IF, according to the new AO classification. A multicenter, multi-year, large-sample study of patients with FNF should be conducted to observe age-related trends.
Conclusion
In this study, we found no change trend in the number of patients in each age group during the period 2018 to 2020. With up to a third of patients with FNF aged 50 to 70 years having stable fracture, surgeons should comprehensively consider the health status of the patient and adopt IF treatment for appropriate fracture types.
Research Data
Research Data for Proportion of stable femoral neck fracture types in different age groups: a population-based study
Research Data for Proportion of stable femoral neck fracture types in different age groups: a population-based study by Yu-xuan Jiang, Dong-xu Feng, Xiao-long Wang, Wei Huang, Wu-qiang Jiang, Chengxi Wu, Yang-jun Zhu in Journal of International Medical Research
Footnotes
Availability of data and materials
The datasets used/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.