
Abstract
Objective
This study was performed to evaluate the mid-term clinical efficacy of the Femoral Neck System (FNS) (DePuy Synthes, Zuchwil, Switzerland) in treating young patients with unstable Pauwels type III femoral neck fractures.
Methods
We performed a retrospective observational analysis of 21 young adults treated with the FNS. Clinical outcomes were assessed based on fracture reduction quality, Harris hip scores, and postoperative complication rates.
Results
The study comprised 21 patients with a mean age of 35 years (range, 20–50 years) who were followed for a mean duration of 22.8 months (range, 16–30 months). Closed reduction was unfeasible in three (14.3%) patients, each of whom required open reduction. Notable postoperative complications were avascular necrosis in two (9.5%) patients, nonunion in one (4.7%), and implant failure in one (4.7%). Each of these complications led to the requirement for total hip arthroplasty.
Conclusion
The favorable mid-term clinical outcomes of this study indicate that the FNS is a potentially effective treatment modality for young individuals with unstable Pauwels type III femoral neck fractures.
Introduction
The treatment of displaced femoral neck fractures in younger patients is a significant clinical challenge, especially in the presence of a high Pauwels angle. 1 These types of fractures are inherently prone to augmented shear forces across the hip joint, elevating the risk of complications such as nonunion or failure of fixation.2–4 Previous reports have described the use of various fixation implants in the management of unstable Pauwels type III femoral neck fractures, encompassing strategies such as employing multiple cancellous screws or utilizing dynamic hip screws. 4 However, in spite of these technical advancements, determining the most effective treatment protocol continues to be a matter of active debate. 5
The Femoral Neck System (FNS) (DePuy Synthes, Zuchwil, Switzerland) has been meticulously engineered to optimize patient outcomes and reduce complications. This innovative system incorporates key advancements including minimally invasive surgical techniques, enhanced procedural efficiency, and improved anti-rotational stability. 6 In vitro studies have shown promising biomechanical results regarding the stability provided by the FNS in fracture management. 7 However, the current literature regarding application of the FNS in the management of these fractures is limited in scope, and studies to date are characterized by relatively short follow-up periods. This study was performed to assess the mid-term clinical results of using the FNS in a consecutive series of unstable Pauwels type III femoral neck fractures.
Materials and methods
This study involved 21 consecutive young patients aged 20 to 50 years with Pauwels type III femoral neck fractures who underwent surgical treatment with the FNS from August 2018 to August 2021. The exclusion criteria for this study were rigorous, encompassing patients with pathological fractures, existing coagulopathies, a history of ipsilateral hip surgery, and general surgical contraindications. Patients with femoral neck fractures occurring in the context of coxarthrosis, avascular necrosis of the femoral head, or severe rheumatoid arthritis and those with fractures resulting from polytrauma were also excluded. This study was conducted in strict accordance with ethical research standards and in compliance with applicable guidelines and regulations, and formal ethics approval was not required. All patients were fully informed about the study’s aims, procedures, risks, and benefits as well as their right to withdraw at any time. All patients then provided verbal consent, which was documented in writing. Additionally, our methodology and reporting adhere to the relevant Equator Network guidelines. 8
The patients were positioned supine on a standard orthopedic fracture table for the procedure. Closed reduction was initially attempted, employing a combination of traction, internal and external rotation, abduction, and adduction maneuvers on the affected limb with adjustments made in response to the specific demands of the fracture reduction. Efforts were made to correct any retroversion deformity by applying anteroposterior pressure at the hip joint. When closed reduction proved unsuccessful, we proceeded to open reduction and internal fixation. This was facilitated using a modified Smith–Petersen approach, which assisted in achieving anatomic or near-anatomic reduction. The anti-rotation guidewire was strategically placed near the superior aspect of the femoral neck and laterally positioned away from the midline within the neck. A longitudinal incision of approximately 4 cm in length was made parallel to the lesser trochanter. We then employed an angled guide to insert a pin, targeting a central position within the femoral neck. This approach was crucial for ensuring optimal placement of the lag screw within the center of the femoral head. Following accurate determination of the guidewire’s depth, an implant comprising a bolt and screw was introduced via the insertion handle, completing the fixation process.
In the immediate postoperative period, patients were encouraged to initiate hip muscle strengthening and stretching exercises within the first 24 hours following surgery. Commencement of partial weight-bearing exercises was advised at the 3-month postoperative mark, with gradual progression to ambulation without crutches as clinical and radiological signs indicated successful bone union. Follow-up evaluations were systematically conducted at 1, 3, 6, and 12 months postoperatively and annually thereafter. These assessments encompassed a comprehensive evaluation of the fracture reduction quality, incidence of nonunion, and Harris hip score in addition to monitoring for femoral head necrosis and other complications. The quality of fracture reduction was determined using anteroposterior and lateral hip X-rays, employing the method established by Haidukewych et al. 9 Nonunion was defined as either failure of fixation or the absence of fracture healing for a minimum of 6 months post-fracture, with no signs of healing progression over a 3-month period. 2 Osteonecrosis of the femoral head was assessed radiographically and classified according to the Ficat criteria. 10 Additionally, each follow-up visit involved documentation of complications such as infection, deep vein thrombosis, or ectopic ossification. The Harris hip score, which is used to evaluate pain, function, range of motion, and gait, was also systematically recorded, providing a multifaceted assessment of patient recovery. 11
Results
The mean age of the 21 young adult patients in this retrospective analysis was 35 years (range, 20–50 years). The mean duration from admission to surgery was 1.9 days (range, 1–5 days). The mean duration of the surgical procedures was 65.5 minutes (range, 55–125 minutes). Throughout the course of our study, we followed up the 21 patients for a mean duration of 22.8 months (range, 16–30 months). These details are provided in Table 1 and Table 2.
Patient characteristics (21 patients with 21 fractures).

Data are presented as n, n (%), or mean (range).
Patients’ clinical details.

Closed reduction was initially attempted but proved unsatisfactory in three patients, each of whom required transition to open reduction. One patient developed a postoperative superficial infection, which was effectively managed with antibiotic therapy. Ectopic ossification was observed in one patient during follow-up; however, this did not result in any reported discomfort. The patients were generally permitted to bear full weight at a mean of 6.5 months postoperatively (range, 5–8 months). At the latest follow-up, the mean Harris hip score was 88.6 points (range, 78–100). Notably, one patient developed nonunion, one patient developed fixation failure (occurring at 6 months postoperatively and attributed to an off-center position of the implant on the anteroposterior radiograph (Figure 1)), and two patients developed avascular necrosis of the femoral head (Figure 2). All four of these patients ultimately required total hip arthroplasty.
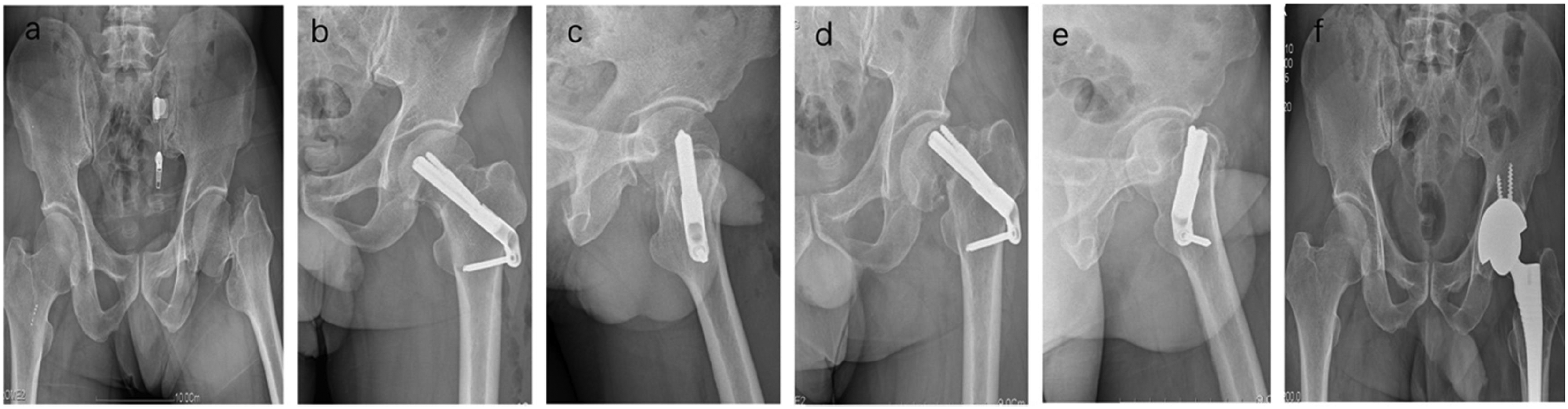
Radiographs of a 45-year-old man with a left femoral fracture treated by fixation with the Femoral Neck System. (a) Preoperative radiograph. (b, c) Immediate postoperative radiographs. Note that the implant is not in the central position on the anteroposterior view and (d–f) six-month postoperative radiograph showing internal implant cut-out necessitating total hip arthroplasty.

Radiographs of a 48-year-old woman with a left femoral fracture treated by fixation with the Femoral Neck System. (a) Preoperative radiograph. (b, c) Immediate postoperative radiographs and (d–f) three-year postoperative radiographs showing femoral head avascular necrosis necessitating total hip arthroplasty.
Discussion
Pauwels’ classification system categorizes femoral neck fractures based on the angle of the fracture line relative to the horizontal plane. 12 According to this system, an increased angle is associated with a higher postoperative vertical load at the fracture site. Unstable Pauwels type III fractures represent a particular challenge, especially in young adults, who are at higher risk of complications such as femoral head osteonecrosis and nonunion. The reported incidence of osteonecrosis following femoral neck fractures in this demographic widely ranges from 11% to 86%.1,13,14 Achieving anatomically accurate reduction and secure fixation is paramount for successful surgical outcomes. This is especially critical for young adults, whose active lifestyles heighten the risk of complications from improperly managed fractures.
Numerous treatment options are available for femoral neck fractures, including multiple cannulated screws, the dynamic hip screw (DHS), and the more recently developed medial support plate. 5 Despite the range of options, there is no consensus has been reached on the gold standard treatment protocol. The recently developed FNS incorporates the benefits of both multiple cannulated screws and the DHS. However, only a few clinical studies to date have evaluated the use of the FNS, especially in young adults with unstable Pauwels type III fractures. Additionally, these studies often have relatively short follow-up periods, which may not adequately capture the long-term outcomes and efficacy of the FNS in these unstable cases. Schuetze et al. 15 assessed the clinical outcomes of the FNS versus the DHS in treating Garden grade I–IV fractures, highlighting quicker implantation and reduced blood loss with the FNS. Stassen et al. 16 evaluated application of the FNS in treating Pauwels type I–III fractures with a 1-year follow-up, and their results suggested that the FNS is a promising, safe, and effective treatment option.
Previous investigations have corroborated the biomechanical stability provided by the FNS in managing Pauwels type III femoral neck fractures. Stoffel et al. 6 conducted a biomechanical analysis comparing the FNS, DHS, and cannulated screws in stabilizing such fractures using a cadaveric model. Their findings suggested that the FNS is an efficacious alternative, offering stability comparable to that of the DHS and surpassing that of cannulated screws. 6 Additionally, Jung et al. 7 investigated the efficacy of the FNS in finite element models for securing Pauwels type III femoral neck fractures. They found that incorrect positioning of the FNS bolt could result in increased interfragmentary movement and elevated compressive and shear stresses. 7
This retrospective analysis was performed to evaluate the mid-term outcomes of patients with Pauwels type III femoral neck fractures treated using the FNS. In our patient cohort, we observed a high union rate of 90.5%, surpassing the reported nonunion rates of 16% to 59% in prior studies that used various devices for similar fractures.1,13,14 During the follow-up period, two patients developed avascular necrosis, one developed nonunion, and one developed implant failure. The considerable success rate observed in our study can likely be attributed to several key factors. First, surgery was performed within 48 hours for the majority of patients, a practice known to reduce the incidence of avascular necrosis.13,14 Second, a focused effort was made to achieve optimal anatomical reduction, predominantly through closed reduction techniques. The need for an anterior surgical approach in only three patients also contributed by minimizing vascular trauma. Third, extending the weight-bearing restriction period to 3 months may have helped to reduce the incidence of fixation failure by promoting more robust fracture healing. It is imperative to recognize that vascular injuries resulting from the fracture itself and unstable fixation are significant contributors to nonunion and avascular necrosis. Primary total hip arthroplasty may be a treatment option for young patients at high risk of complications such as avascular necrosis of the femoral head or nonunion. 17 The keys to favorable outcomes are timely surgical intervention, stable fixation, preservation of the hip vasculature, and achievement of satisfactory anatomical reduction.
This study has several limitations that should be taken into consideration. First, the retrospective design and absence of a control group may have impacted the robustness and generalizability of our findings. Retrospective analyses have inherent biases, and such biases might have affected the validity of our conclusions. Second, the relatively small sample size, a consequence of the rarity of these fractures, further constrained the statistical power of our study. Although this limitation is understandable, it underscores the need for caution in extrapolating our results to the broader population of patients with femoral neck fractures. The limited statistical power may have inhibited our ability to detect significant differences or nuances in patient outcomes that could inform clinical practice. Third, although our follow-up period was relatively extensive, averaging 22.8 months, this time frame may not be comprehensive enough to encompass all instances of osteonecrosis of the femoral head. This complication can arise up to 5 years post-injury; thus, our duration of follow-up, while adequate for evaluating immediate healing outcomes, might have been insufficient for capturing the full extent of potential long-term complications. Consequently, our findings should be interpreted with caution, particularly those findings related to long-term complications. To more conclusively determine the efficacy of the FNS and its long-term effects on patient outcomes, further research involving larger patient cohorts and longer follow-up periods is essential. Such studies would provide a more comprehensive understanding of the performance of the FNS and its role in the management of Pauwels type III femoral neck fractures.
Conclusion
The mid-term outcomes of our study suggest that the FNS represents a potentially effective treatment modality for young patients with unstable Pauwels type III femoral neck fractures. The results of our research demonstrate favorable clinical outcomes associated with use of the FNS, thereby positioning it as a viable therapeutic option in the management of this specific patient cohort.
Footnotes
Acknowledgments
We would like to thank all participants in this study for their enthusiasm, tireless work, and sustained support.
Author contributions
ChangYong Guo: Writing of the paper, data collection and analysis.
JiaPing Huang: Writing of the paper, data collection and analysis.
ZhiBiao Chen: Data collection.
ZeMing Cai: Searching of related articles and data analysis.
TaoYi Cai: Data collection, performance of surgeries, and management of the research team.
All authors have made significant contributions and approved the content of the manuscript. All listed authors meet the authorship criteria according to the latest guidelines of the International Committee of Medical Journal Editors, and all authors are in agreement with the manuscript.
Data availability statement
Data are available on request from the authors.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This study was supported by the Special Project for Research on Prevention and Treatment of Military Training Injuries (No. 21XLS23).