
Abstract
Introduction
Femoral neck fractures (FNF) represent a significant challenge in orthopedic practice, demanding prompt intervention to restore function and mobility in affected individuals. Numerous surgical interventions have been developed to address these fractures, including internal fixation with devices such as the Femoral Neck System (FNS, DePuy Synthes, Inc., West Chester, PA, USA). However, the optimal fixation system remains unclear. Understanding the postoperative outcomes associated with these interventions is crucial for optimizing patient care and informing treatment decisions.
Significance
This PRISMA-compliant systematic literature review evaluates the efficacy and safety of the Femoral Neck System relative to other operative treatment options. Clinical and safety outcomes included mortality, perioperative complications, postoperative complications at 1 year, and reoperation.
Results
A total of 117 studies with 68,567 patients with FNF treated with internal fixation were identified. Of these, thirteen included FNS as a treatment arm (1078 patients). Due to heterogeneity in study designs and populations, only the eleven studies that directly compared FNS to other operative treatments, and 2 non-comparative studies that treated with FNS were included in the systematic review. Seven of the eleven included studies had high risk of bias, 2 had moderate risk of bias, and 2 had low risk of bias. FNS groups had similar or significantly lower incidences of postoperative complications, reoperations, and mortality compared to cannulated screw, cancellous screw, or dynamic or sliding hip screw groups in all studies.
Conclusion
FNS can be a safe and effective operative treatment option for FNF. Safety outcomes and reoperation rates are comparable between patients treated with FNS and patients treated with cannulated screws, cancellous screws, and dynamic or sliding hips screws. Future prospective, controlled studies are needed to confirm the safety and efficacy of FNS relative to other operative treatment options.
Introduction
Femoral neck fractures (FNF), the most common hip fracture,
1
are frequently treated with internal fixation, but complications frequently arise, which may require reoperation.
2
Recently, a new fixation device, Femoral Neck System (FNS, DePuy Synthes, Inc., West Chester, PA, USA) was launched for treatment of femoral neck fractures, including basilar, transcervical, and subcapital fractures, in adults and adolescents (age 12-21 years) in which the growth plates have fused or will not be crossed (Figure 1). FNS was developed to reduce complications and reoperations by increasing construct stability, reducing surgical invasiveness, and reducing the risk of lateral implant protrusion.
3
The FNS design compensated for 15 mm of femoral neck shortening without lateral protrusion by a telescoping mechanism.
3
Moreover, a single insertion handle allows for placement of the central bolt as well as the antirotation screw to reduce procedural complexity and enhance operational efficiency.
3
The bolt is currently available in units of 5 mm and a technical note has reported a modified technique for improved control of the depth of the bolt.
4
Three dimensional models of the FNS device. Used with permission.
Mechanical testing of FNS with standardized foam models has indicated up to 40% increased rotational stability compared to a sliding hip screw (SHS), and a minimum of 150% more rotational stability compared to a 3 cannulated screw.5,6 A biomechanical study in a cadaveric model found that FNS had comparable stability to dynamic hip screws paired with antirotation screws or blades and superior stability compared to 3 cannulated screws for treating femoral neck fractures. 7 However, the relative safety and efficacy of FNS compared to other treatment options remain undetermined. Here, we report the results of a systematic literature review to evaluate safety and efficacy outcomes associated with FNS relative to traditional operative treatment options in femoral neck fractures resulting from any mechanism of injury.
Methods
Literature Search and Study Selection
This study adheres to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 8 The PRISMA checklist associated with this systematic review can be found in Supplemental Files 1 and 2. A protocol was prepared based on the PROSPERO protocol guidelines. The review was not registered. Searches of PubMed were completed using the Application Program Interface (API) in the AutoLit platform (Nested Knowledge, nested-knowledge.com). All study metadata and abstracts from the search results were also obtained via API. Searches of Cochrane Library and Embase databases were completed through their respective web interfaces and the results were uploaded to the AutoLit platform. Searches were restricted to studies published after January 1, 2012 to capture the previous decade of comparative treatments and cover the date that FNS came on the market in 2017. Search terms included the phrases “femoral neck fracture”, “femoral neck system”, “sliding hip screw”, “cannulated screw”, and “internal fixation”. The full search strings are available in Supplemental Table 1.
Identified studies were evaluated for inclusion in the systematic review. Study inclusion criteria included those reporting adult patients with femoral neck fracture treated with FNS. All mechanisms of injury were included. Exclusion criteria were studies that did not report patients treated with FNS, studies that did not report the outcomes of interest, studies that did not separate patient outcomes by intervention, studies with less than 5 patients, studies that did not relate to femoral neck fracture, studies not reporting interventions or outcomes of interest, and studies reporting on a subpopulation that could introduce bias, including studies that focused on patients with cancer, HIV, or Parkinson’s disease. In vivo/in vitro studies, symposium/conferences, qualitative review articles, letters of correspondence, in silico study/mathematical models, guideline articles, technical notes, editorial/opinion articles, meta-analyses or systematic reviews, secondary analyses, protocols, studies not written in English, or interim analyses were also excluded. The reference lists of identified articles were also screened for potentially relevant papers. Each study was screened by a single investigator.
Data Extraction
Data was extracted by a single investigator for each study and reviewed by 2 independent investigators. Patient characteristics included age and fracture stability (Garden classification). Procedure characteristics included length of operation, intraoperative blood loss, and length of hospital stay. Methods for measuring blood loss vary widely, potentially introducing heterogeneity into the data. Intraoperative blood loss was extracted as reported in the study. Clinical and safety outcomes included mortality, perioperative complications (deep vein thrombosis [DVT] and perioperative surgical site infection), postoperative complications at 1 year (avascular necrosis [AVN] of the femoral head, non-union, internal fixture loosening, postoperative surgical site infection, hematoma, iatrogenic fracture, and femoral neck shortening), and reoperation (unspecified, implant removal, or conversion to another treatment).
Risk of Bias
Risk of bias (RoB) was assessed for comparative studies using the Newcastle-Ottawa Scale. 9 Criteria for rating a study as low, moderate, or high risk of bias were made based on the decision rules described by Sharmin et al, 10 outlined in Supplemental Table 2. The RoB was completed independently by 2 reviewers with any disagreements adjudicated by a third reviewer.
Statistical Analysis
Due to heterogeneity in data and the limited number of multi-armed studies available that distinguished between patients with acute and delayed instrumentation, inferential statistics were not performed, and data are expressed as descriptive statistics only. Statistics are reported as counts and percentages, median (interquartile range (IQR)), or mean ± standard deviation (SD).
Results
Literature Search Results
Our searches identified 1674 individual studies. Of the identified studies, 1394 were excluded based on title and abstract review (see PRISMA flowchart in Figure 2). The remaining 271 articles underwent full-text review. Four articles were identified through expert recommendation, which also underwent full-text review. Nine articles did not have full texts available, and 259 articles were excluded for other reasons, while 108 studies reported a comparable intervention but did not report patients treated with FNS (see PRISMA flowchart in Figure 2). Due to heterogeneity in study designs and populations, only the 13 studies that included patients treated with FNS were included in the systematic review.11-23 Results from all 117 studies reporting either FNS or a comparable intervention are summarized in Supplemental Tables 3-6. Of the 13 studies reporting FNS, all were retrospective cohort studies.11-23 Three studies compared dynamic or sliding hip screws or cannulated screws to FNS,16,17,20 2 studies had a single intervention of FNS with no comparator,12,18 1 study compared dynamic or sliding hip screws or cancellous screws to FNS,
21
1 study compared dynamic or sliding hip screws to FNS,
16
and 6 studies compared cannulated screws to FNS.13-15,19,22,23 Two studies were found to have low risk of bias,19,23 2 had moderate risk of bias,13,16 and 7 had high risk of bias.11,14,15,17,20-22 The 2 non-comparative studies were not included in the risk of bias (Supplemental Table 7) PRISMA study selection flowchart.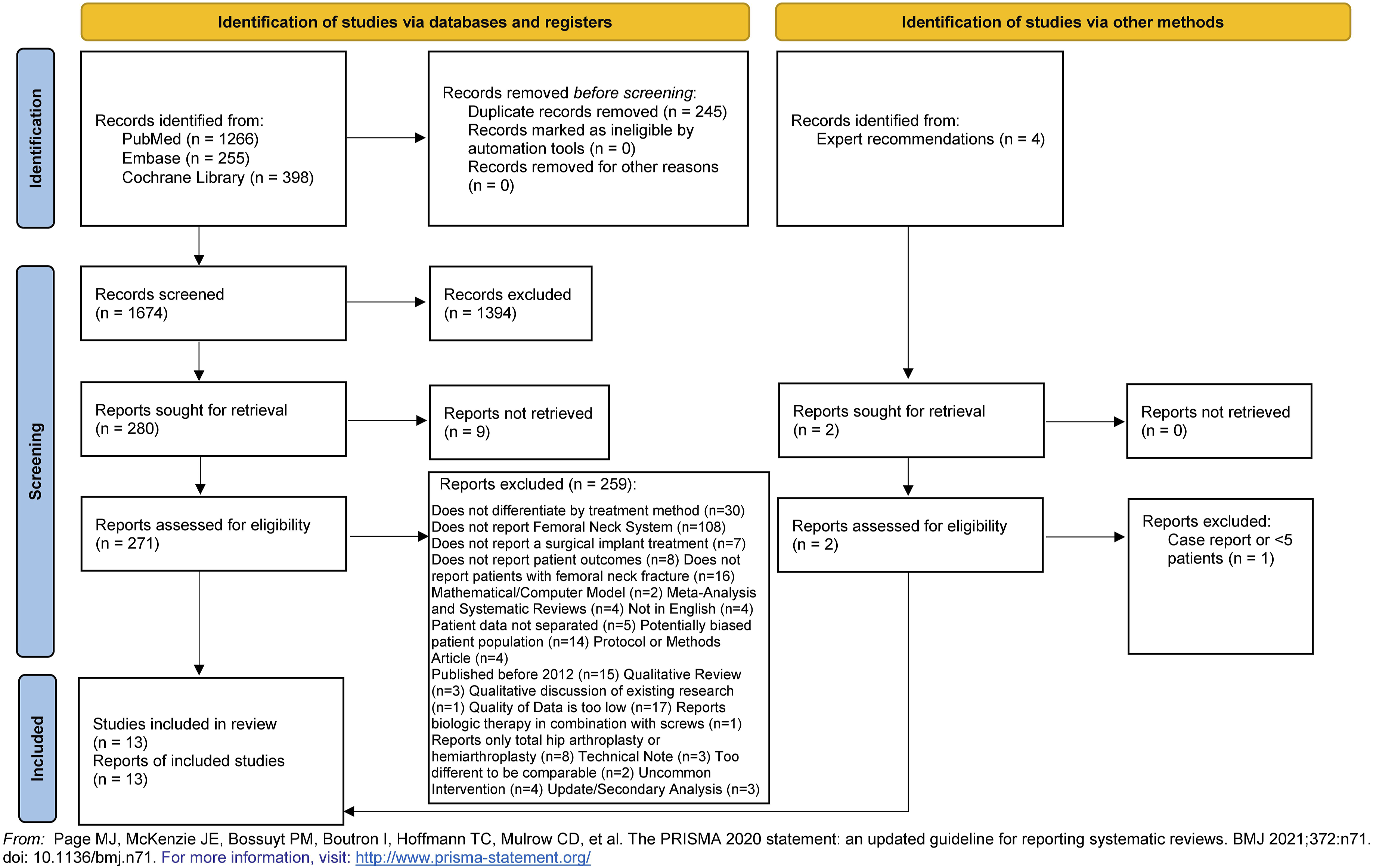
FNS vs Cannulated Screws
Study Characteristics
Seven studies compared FNS against cannulated screws.13-15,19,20,22,23 Of these, Vazquez et al 20 compared a third treatment such that head-to-head comparisons between FNS and cannulated screws were not made. Nibe et al 15 and Zhang et al 22 restricted study patients to ≥65 years old and Vazquez et al 20 reported outcomes in patients ≥75 years old. Hu et al restricted to patients under 60 years old. 14 Zhang et al 22 restricted their study to patients with AO31-B type fractures, which include Garden Type II, III, and IV, Zhou et al 23 reported only patients with Pauwels Type III fractures, and Vazquez et al 20 restricted their study to patients with Garden Type I and II fractures. Two studies did not apply fracture type or age-based selection criteria, but excluded pathological fractures.13,19
Three studies did not specify mechanism of injury.14,19,20 In He et al, the majority of fractures were caused by falls in both groups (63.6% [21/33] in patients treated with FNS and 69.4% [25/36] in patients treated with cannulated screws). 13 In Nibe et al, the majority of fractures were caused by low-energy falls in both groups (88.0% [22/25] in patients treated with FNS and 81.5% [22/27] in patients treated with cannulated screws). The remaining fractures were caused by traffic accidents (8.0% [2/25] in patients treated with FNS only), other high-energy injuries (3.7% [1/27] in patients treated with cannulated screws only) or unknown causes (4.0% [1/25] in patients treated with FNS and 14.8% [4/27] in patients treated with cannulated screws). 15 In Zhou et al, fractures were caused by traffic accidents or falls and pathological fractures were excluded. 23
Two studies had low risk of bias,19,23 1 had moderate risk of bias, 13 and 4 had high risk of bias.14,15,20,22 Common sources of risk of bias were selection bias, lack of comparability between groups, and short follow-up. A summary of risk of bias assessments can be found in Supplemental Table 7.
Patient Baseline Characteristics
Patient baseline characteristics are presented in Supplemental Table 3. Across studies, the average age ranged from 47.6 ± 10.3 13 to 85.0 ± 6.6 20 for patients with cannulated screws, and from 50.5 ± 8.5 14 to 86.1 ± 4.6 20 for patients with FNS. No studies reported statistically significant differences in age between groups. Only Nibe et al 15 and Zhou et al 23 did not present Garden classification. Except for Vazquez et al, 20 in which most injuries were Type I, most injuries were Type II or above. No study reported significant differences for Garden classification between groups. Most studies had follow-up periods >12 months, but Vazquez et al 20 had follow-ups from 1-6 months and Zhou et al 23 had follow-ups from 10-22 months. The longest follow-up period was a range of 14-24 months. 19
Procedure Characteristics
Procedure Characteristics.

Data are expressed as mean ± SD or median (IQR). “--” indicates no data reported.
aIndependent-samples t test.
bAnalysis unclear (either Mann-Whitney U test or independent-samples t test).
cLinear regression.
dKruskal-Wallis test.
eMann-Whitney U test.
fStatistical methods not clearly reported.
Patient Outcomes
Patient Outcomes.

Data are expressed as mean ± SD, median (IQR), or % (n) unless otherwise indicated. “--“ indicates no data reported.
AVN = avascular necrosis; DVT = deep vein thrombosis; FNS = Femoral Neck System; HA = hip arthroplasty; THA = total hip arthroplasty.
aChi-squared test of independence.
bIndependent-samples t-test.
cFisher's exact test.
dStatistical methods not clearly reported.
eKruskal-Wallis test.
FNS vs Dynamic or Sliding Hip Screw
Study Characteristics
Four studies compared FNS with dynamic or sliding hip screws.16,17,20,21 Of these, Vazquez et al 20 and Xu et al 21 compared a third treatment such that head-to-head comparisons between FNS and cannulated screws were not made. Three studies applied age-related inclusion criteria: Vazquez et al 20 (≥75 years old), Schuetze et al 17 (≥50 years old) and Xu et al 21 (<65 years old). Vazquez et al 20 and Xu et al 21 restricted their studies to patients with Garden Type I and II fractures. Niemann et al 16 and Schuetze et al 17 excluded pathological fractures. No studies specified mechanism of injury. One study had moderate risk of bias 16 and 3 studies had high risk of bias.17,20,21 Common sources of risk of bias included selection bias, failure to account for imbalances in important patient characteristics between cohorts, short follow-up, and failure to properly adjust analyses for imbalances in follow-up periods between cohorts. A summary of risk of bias assessments can be found in Supplemental Table 7.
Patient Baseline Characteristics
Across studies, the average age ranged from 60.5 ± 17 16 to 83.4 ± 7.3 years 20 for patients with dynamic or sliding hip screw, and from 60.7 ± 15.2 21 to 86.1 ± 4.6 years 21 for FNS patients. No study found significant differences in age between groups. Likewise, no study reported significant differences in Garden classification between groups. Follow-up periods ranged from 7.4 ± 3.4 days 16 to 12-16 months. 21 No study reported significant differences for follow-up periods between groups (Supplemental Table 3).
Procedure Characteristics
The average duration of operation ranged from 54.7 ± 17.4 17 to 91.7 ± 24.0 minutes 16 for dynamic or sliding hip screw patients, and from 36.3 ± 11.6 17 to 54.0 ± 26.1 minutes 16 for FNS patients. In each study, FNS had significantly shorter operation time than dynamic or sliding hip screws.16,17,20,21 Only Xu et al 21 reported on intraoperative blood loss; dynamic or sliding hip screws operations had significantly more blood loss than FNS (median, range: 50, 30-50 vs median, range: 30, 20-50; P < 0.01). Length of hospital stay ranged from 3-6 21 to 12.4 ± 5.3 days 20 for dynamic or sliding hip screws and from 2-4 21 to 10.3 ± 6.0 days 20 for FNS. Only Schuetze et al 17 and Xu et al 21 found significant differences for length of hospital stay between groups; in both cases, FNS patient stays were significantly shorter than dynamic or sliding hip screw patient stays (Table 1).
Patient Outcomes
No study reported incidence of non-union. No significant differences between FNS and dynamic or sliding hip screws were reported for loosening or failure of the internal fixure,17,21 avascular necrosis,17,21 deep vein thrombosis, 21 femoral neck shortening,16,17,21 hematoma or surgical site infection, 17 reoperation,17,20 or mortality17,20 (Table 2).
FNS vs Other Comparators
Xu et al 21 compared FNS with cancellous screws. The study excluded patients >65 years old who had Garden Type III or IV fractures or pathological fractures and did not specify mechanisms of injury. The study had a high risk of bias, primarily due to selection bias, failure to account for imbalances in important patient characteristics between cohorts, short follow-up, and failure to properly adjust analyses for imbalances in follow-up periods between cohorts. Xu et al 21 used linear regression that included a third procedure such that head-to-head comparisons were not made, median operation time, blood loss, and length of hospital stay were lower for FNS than cancellous screws (Table 1). No differences in patient outcomes were reported between the FNS and cancellous screws (Table 2).
Cintean et al 11 compared FNS with hemiarthroplasty. The study did not apply age-based selection criteria and did not specify mechanisms of injury. The study had high risk of bias due to lack of comparability between the groups, short follow-up, and loss of patients to follow-up. There were no significant differences between groups for age, Garden classification, or follow-up period (Supplemental Table 3). Cintean et al 11 found that length of hospital stay was significantly shorter for FNS than hemiarthroplasty (Table 1), but did not find any differences in patient outcomes (Table 2).
Non-Comparative Studies
There were 2 non-comparative studies of FNS.12,18 Davidson et al 12 excluded cases with pathological fractures and Stassen et al 18 excluded patients with polytrauma. Neither study applied age-related selection criteria or specified mechanism of injury. The average age in both studies was 63 years. In both studies, more than half of the fractures were at or below Garden Type II. The mean follow-up periods were 7 12 and 6 months 18 (Supplemental Table 3). Mean length of operations were 44 12 and 33 minutes. 18 Mean intraoperative blood-loss was 51 12 and 34 mL. 18 Average length of hospital stay was 5.7 ± 3.9 12 and 4.0 ± 2.8 days 18 (Table 1). Davidson et al 12 reported 1.0% (1/102) non-union events and 1.0% (1/102) patients with loosening/failure of internal fixtures, while Stassen et al 18 did not report on non-union events and reported 5.9% (2/34) patients with loosening or failure of internal fixtures. Avascular necrosis was reported in 2.9% (3/102) 12 and 11.8% (4/34) 18 cases. Davidson et al 12 reported that 8.8% (9/102) of cases were converted to hemiarthroplasty while Stassen et al 18 reported that 17.6% (6/34) were converted with another 5.9% (2/34) implants removed. Neither study reported any deaths12,18 (Table 2).
Discussion
The results of our systematic literature review suggest that FNS can be safely and effectively used to treat FNF compared to other operative treatments. The majority of studies reported no significant difference in patient outcomes including non-union,11,15,19 change in internal fixture loosening/failure,17,19,21,22 postoperative complications,11,16,17,23 reoperation, 11 and mortality,11,17,20 with respect to the comparator device. Studies identified significantly better outcomes associated with FNS compared to cannulated screws, for reduced femoral neck shortening length and incidence, 14 reduced incidence of reoperation, 15 and lower incidence of implant removal. 22 One study, a systematic review by Zhou et al, reported that FNS were associated with a significantly lower incidence of overall complications compared to those treated with cannulated screws. 23
The relative incidences of complications and mortality found in the thirteen studies reporting FNS are also comparable or lower than the incidences reported for comparators in the 104 comparator-only studies, supporting the conclusion that FNS is comparable to similar operative treatments. The 2 non-comparative studies found similar results when using FNS. These conclusions are also in line with previous systematic reviews comparing operative treatments, which have found that dynamic and sliding hip screws and cannulated cancellous screws are largely comparable with respect to safety outcomes.24,25 Recently, another case series was published reporting outcomes in 12 patients after treatment with FNS, which found higher rates of complications compared to previously reported incidences for comparators. 26 A larger case series recently reported a high incidence of femoral neck shortening in patients treated with FNS, with no effect on fracture healing. 27 However, a recent comparative study found no difference in incidence of complications between patients treated for femoral neck fractures with FNS or cancellous screws, while patients treated with FNS had significantly better joint function, 28 and another comparative study found that FNS was more effective compared to a dynamic compression locking plate system. 29 Future comparative studies are need to confirm the relative incidence of complications in patients treated with FNS and address considerations such as long-term stability and mobility, which may have different priorities in different patient populations, depending on age and activity.
Factors other than implant choice impact revision and conversion rates and incidence of AVN, potentially explaining the low effect size between groups. The use of computed tomography scans or magnetic resonance imagery, rather than basic X-rays, may improve diagnostic accuracy by allowing physicians to visualize the fracture more clearly. Different imaging methods and protocols for when patients received imaging may have contributed to heterogeneity in reported incidence AVN between studies and among patients in individual studies. Better visualization may lead to more accurate classification of fracture displacement, informing treatment decisions.30-32 Stable internal fixation is key to prevent non-union and allow for positive functional outcomes, especially in younger patients, who have higher functional demands 33 and a high rate reoperation and conversion to total hip arthroplasty. 34 Young patients with Pauwels Type III FNF specifically have increased likelihood of loss of reduction and non-union. 35 The use of adjunctive implants is currently uncommon, but combining established implants with other stabilizing measures may provide additional stability and improve patient functional outcomes, particularly in young patients with displaced fractures.36-39
A simplified classification scheme of stable vs unstable may also improve treatment decision-making. Current guidelines suggest classifying fractures as non-displaced (Garden Type I or II) or displaced (Garden Type III or IV). 40 Both non-displaced and displaced fractures may be treated with internal fixation in younger patients,33,41 but currently only non-displaced fractures are recommended to be treated with internal fixation in older patients. 40 However, Vazquez et al suggest that using implants, including FNS, cannulated screws, or dynamic or sliding hip screws, to treat displaced fractures in older patients can lead to positive safety outcomes and low rates of reoperation. 20
Reduction quality and implant placement were not consistently reported in the studies reviewed. Achieving excellent reduction, including open reduction if necessary, and using standardized intraoperative imaging to ensure correct implant placement can both lower the need for revision or conversion and lower the incidence of AVN.42-44 Reduction quality and measures of implant placement should be assessed during treatment and reported in further studies to enable future analyses to accurately compare implants.
Limitations
The primary limitation of our review was the lack of prospective studies on patients treated with FNS, particularly the lack of RCTs. Heterogeneity in study design and patient and procedure characteristics prevented a broader meta-analysis, including studies that did not report use of FNS. This variability is likely due to heterogeneity in trauma patients, as well as differences in study designs. Many data elements were reported inconsistently, especially perioperative and postoperative complications. As mentioned above, methods for measuring blood loss varied widely, introducing heterogeneity into the data and precludes a definitive conclusion. Variations in fracture classification, patient age, follow-up time, mechanism of injury, and data collection methodologies between studies likely contributed to the heterogeneity of the results. Additionally, over half of the included studies had high risk of bias. Lack of comparability between cohorts was a common source of risk of bias, likely due to the heterogenous nature of trauma patient presentation. Finally, all but 1 study 19 in this review did not have long enough follow-up for the outcomes of interest to occur, indicating a need for longer-term studies on FNF treatment with FNS to verify these findings.
Conclusions
FNS can be a safe and effective treatment for FNF, including in older patients, with published incidences of complications similar to comparable treatment options. Further studies are necessary to prospectively compare FNS to other operative treatments.
Supplemental Material
Supplemental Material - Evaluation of Post-Operative Outcomes of Femoral Neck Fracture Interventions: A Systematic Review
Supplemental Material for Evaluation of Post-Operative Outcomes of Femoral Neck Fracture Interventions: A Systematic Review by Erin Sheffels, Mariam Khalil, Kristen Hutchison, Nicole J. Hardy, Ranita Tarchand, John M. Pederson, Anjani Parikh, and Michael Blauth in Geriatric Orthopaedic Surgery & Rehabilitation
Supplemental Material
Supplemental Material - Evaluation of Post-Operative Outcomes of Femoral Neck Fracture Interventions: A Systematic Review
Supplemental Material for Evaluation of Post-Operative Outcomes of Femoral Neck Fracture Interventions: A Systematic Review by Erin Sheffels, Mariam Khalil, Kristen Hutchison, Nicole J. Hardy, Ranita Tarchand, John M. Pederson, Anjani Parikh, and Michael Blauth in Geriatric Orthopaedic Surgery & Rehabilitation
Supplemental Material
Supplemental Material - Evaluation of Post-Operative Outcomes of Femoral Neck Fracture Interventions: A Systematic Review
Supplemental Material for Evaluation of Post-Operative Outcomes of Femoral Neck Fracture Interventions: A Systematic Review by Erin Sheffels, Mariam Khalil, Kristen Hutchison, Nicole J. Hardy, Ranita Tarchand, John M. Pederson, Anjani Parikh, and Michael Blauth in Geriatric Orthopaedic Surgery & Rehabilitation
Footnotes
Acknowledgements
The authors acknowledge Superior Medical Experts and Nested Knowledge, Inc. for research and editorial assistance. The authors acknowledge Karl Holub, Stephen Mead, Jeffrey Johnson, and Darian Lehmann-Plantenberg for their design, development, and support of the Nested Knowledge meta-analytical software.
Author Contributions
ES contributed to the study design and drafted and revised the manuscript. MK, KH, and RT contributed to the data acquisition. NJH contributed to the study design and the acquisition and analysis of the data. JMP contributed to the study design, data analysis, and drafting and revision of the manuscript. AP and MB contributed to the conception and design of the study and the revision of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ES is employed by and hold equity in Superior Medical Experts. JMP is employed by and hold equity in Superior Medical Experts and Nested Knowledge. MK and RT are employed by Nested Knowledge. KH is employed by Superior Medical Experts and Nested Knowledge. NJH is employed by and holds equity in Nested Knowledge. AP and MB are employed by Johnson & Johnson (JnJ) and own stock in the company.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is sponsored by Johnson & Johnson.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.