
Abstract
Introduction:
In an effort to improve health outcomes and promote health equity, healthcare systems have increasingly begun to screen patients for unmet social needs and refer them to relevant social services and community-based organizations. This study aimed to identify factors associated with the successful connection (ie, services started) to social needs resources, as well as factors associated with an attempt to connect as a secondary, intermediate outcome.
Methods:
This retrospective cohort study included patients who had been screened, referred, and subsequently reached for follow-up navigation from March 2019 to December 2020, as part of a social needs intervention at a federally qualified health center (FQHC). Measures included demographic and social needs covariates collected during screening, as well as resource-related covariates that characterized the referred resources, including service domain (area of need addressed), service site (integration relative to the FQHC), and access modality (means of accessing services).
Results:
Of the 501 patients in the analytic sample, 32.7% had started services with 1 or more of their referred resources within 4 weeks of the initial referral, and 63.3% had at least attempted to contact 1 referred resource, whether or not they were able to start services. Receiving a referral to resources that patients could access via phone call or drop-in visit, as opposed to resources that required additional appointments or applications prior to accessing services, was associated with increased odds (aOR 1.95, 95% CI 1.05, 3.61) of connection success, after adjusting for age, sex, race, ethnicity, education, number of social needs, and resource-related characteristics. This study did not find statistically significant associations between connection attempt and any variable included in adjusted analyses.
Conclusion:
These findings suggest that referral pathways may influence the success of patients’ connection to social needs resources, highlighting opportunities for more accessible solutions to addressing patients’ unmet social needs.
Keywords
Introduction
In response to accumulated evidence that social determinants of health shape both downstream health outcomes1-3 and healthcare value,4-6 healthcare systems have increasingly begun to adopt interventions that identify and address the unmet social needs of individual patients as a part of routine clinical care.7-12 These interventions involve screening patients for social needs, such as food, housing, and employment. 13 Patients can then elect to be referred to relevant social needs resources based on their identified needs. Social needs resources may encompass a broad range of services within the health system itself (eg, pharmacy vouchers, transportation vans), local to the community (eg, food pantries, emergency shelter), and part of public programs (eg, the Supplemental Nutrition Assistance Program or Medicaid). Once referred, patients may also receive follow-up assistance in connecting to these social needs resources 14 ; and, in some healthcare systems, volunteers augment the capacity of clinical staff by providing continued support and resource navigation.15-18
In the past 2 decades, evaluations of these clinical interventions have reported success in both the identification of patients’ unmet social needs and referral to address those needs; however, the results of studies that assess patients’ actual connection to social needs resources, once referred, have been mixed. 19 An interplay of individual, community, and policy-level factors contribute to this gap between receiving a referral and receiving the referred services, motivating a multilevel perspective informed by multiple disciplines.20-22 Understanding the factors associated with the successful connection to social needs resources may offer new insights into the barriers and facilitators of an effective social needs response within clinical settings. 23
The primary aim of this study was to examine the association between patients’ successful connection to referred social needs resources and demographic, social need, and resource-related factors at a federally qualified health center (FQHC), which has implemented a protocol to screen and refer patients for multiple social needs. As a secondary aim, we examined factors associated with patients’ attempts to connect with referred resources, independent of whether or not these attempts were successful, since this may be a more proximal outcome and potential intervention point in the process of achieving a successful connection. Findings can guide the ongoing development of clinical interventions that address patients’ health-related social needs, informing opportunities in everyday practice to improve integration across the socio-medical care continuum.
Methods
Study Setting
This retrospective cohort study was conducted with data from an FQHC that serves a diverse, metropolitan population in the southeastern United States. In 2019, the partnering FQHC saw 36 361 unique patients, of which 57% were uninsured and 93% were members of racial or ethnic minority groups. Of the 25 156 patients with known income status, 97% of these patients earned household incomes at or below 200% of the federal poverty guideline. 24
Program Model and Data Collected
In 2017, the FQHC implemented the Protocol for Responding to and Assessing Patients’ Assets, Risks, and Experiences (PRAPARE) 25 within the pediatrics, adult medicine, and family medicine clinics as a structured procedure to screen patients for health-related social needs. One of the most common screening tools in the United States, 26 PRAPARE consists of a validated set of national core measures integrated into the electronic health record (EHR), which include patient demographics (eg, race, ethnicity, education) and social needs (eg, housing stability, material security, stress). Case managers with social work background administered the PRAPARE assessment via patient interview and made referrals to community-based organizations (CBOs), government agencies, or services internal to the health center based on identified needs. 27 Social needs resources existed to address all screened domains, though quantity and quality of resources varied. Since 2019, trained volunteer community resource navigators have followed up by phone with patients who had received referrals, providing further assistance as well as collecting information about patients’ ability to connect to their referred resources. 18 To avoid overwhelming patients during follow-up, standard protocol instructed community resource navigators to identify and focus navigation efforts on the single most important resource to each patient, since many patients received multiple referrals from case managers. These follow-up calls were scheduled for 2 and 4 weeks after the case manager encounter for patients who consented to follow-up contact.
On March 10, 2020, the governor declared a statewide state of emergency to respond to the COVID-19 pandemic, which issued the first set of public health recommendations that affected the partnering FQHC. As a result, from March to September 2020, case managers conducted proactive screening and referral by phone for the lowest income patients in response to COVID-19 safety precautions and state executive orders. 28 During this time, the local service landscape also experienced major shifts and closures due to stay-at-home orders and pandemic-exacerbated need.
Study Sample
The analytic sample for this study consisted of all patient encounters where: (1) patients were screened for unmet social needs, (2) patients had at least 1 referral from a case manager, (3) patients consented to follow-up contact, and (4) patients were subsequently reached at least once within 4 weeks of the case manager encounter by a community resource navigator to collect connection data.
Outcomes and Measures
This study examined “connection success” as a primary binary outcome, defined as the patient-reported initiation of services with 1 or more referred resources within 4 weeks of the case manager encounter. This measure aligns with the protocol of community resource navigators to focus navigation efforts on the 1 resource most important to each patient, if multiple referrals were given. In addition, we examined “connection attempt” as a secondary binary outcome, defined as a patient-reported attempt to contact 1 or more of their referred resources within 4 weeks of the case manager encounter. All patients who reported connection success were considered to have also met the criteria of a connection attempt.
Adapting Andersen’s Behavioral Model of Health Services Use to the context of health-related social services, 20 we identified predisposing (age at encounter, sex, race, ethnicity, education), enabling (service domain, service site, access modality), and need (unmet social needs) factors for this study. “Service domain” described the area of need that referred resources addressed: food, transportation, housing, financial assistance, healthcare access, social or emotional health, or other. “Service site” described the integration of referred resources relative to the FQHC: internal, such as the FQHC’s own transportation and pharmacy discount programs, or external, such as other community-based or public programs. “Access modality” described the means of accessing the services of referred resources: direct, such as food pantries or assistive hotlines that provided immediate access to services via phone call or drop-in visit; or indirect, such as public programs that required additional appointments or applications prior to accessing services. For multivariate analysis, a single variable tallied the total number of unmet social needs reported by each patient across twelve domains, captured from the PRAPARE assessment: food, transportation, housing, employment, utilities, insurance, healthcare access, stress, social isolation, intimate partner violence, safety at residence, and other material need.
Statistical Analysis
Descriptive statistics were reported to provide information about the demographic, social needs, and resource-related (ie, service domain, service site, access modality) characteristics of the patient sample. Bivariate analyses compared the prevalence of these characteristics between primary (“connection success”) and secondary outcome (“connection attempt”) groups, using appropriate non-parametric, 2-sided tests (Fisher’s exact test or the Mann–Whitney–Wilcoxon test). Unadjusted odds ratios (ORs) were also computed by logistic regression, regardless of bivariate significance level, for comparison with an adjusted model.
For each outcome, a multiple logistic regression analysis with complete cases included all demographic, social needs, and resource-related variables, also adjusting for case manager outreach modality (ie, by phone vs in-person) and screening date (ie, before vs after March 10, 2020) to account for programmatic and broader societal changes due to COVID-19. Standard errors for both the unadjusted and adjusted odds ratios (aORs) were estimated via bootstrap with 1000 replications to correct for bias due to overfitting. 29 For sensitivity analysis, additional multiple logistic regression analyses were conducted with a multiple imputation by chained equations procedure for missing data. 30 Additional details and pooled analysis results are presented in Supplemental Material 1. All analyses were performed using Stata (Release 16; StataCorp LLC, College Station, TX).
Results
Sample Description
From March 11, 2019 to December 28, 2020, a total of 1682 patient encounters were recorded as a part of the FQHC’s screening and referral process. Based on inclusion criteria, 501 patient encounters comprised the analytic subsample for this study (Figure 1). No notable differences in characteristics were found between reached and unreached patients, of those who consented to follow-up.

Eligibility of screened patients for inclusion in analysis.
Characteristics of the analytic sample, including patient demographics, social needs prevalence, and resource-related characteristics, are presented in Table 1. Approximately one-third of patients (34.2%) identified as male, 51.0% as Black or African American, and 40.0% as Hispanic or Latino. A majority of patients were uninsured (69.2%) or unemployed (69.0%). Other prevalent needs included high stress (72.7%), housing insecurity (43.3%), limited access to healthcare (40.4%), and food insecurity (36.2%). Patients most often received referrals to resources in the service domains of healthcare access (47.5%), food assistance (37.5%), financial assistance (32.1%), and social and emotional health (27.9%). About 41.3% of patients had received a referral to a resource internal to the FQHC. Most patients (81.8%) had a referral to at least 1 resource with an indirect access modality, and 53.5% of patients had a referral to at least 1 resource with a direct access modality.
Demographic, Social Need, and Resource-Related Characteristics of an Analytic Sample of Patients with Referrals for Unmet Social Needs, by Connection Outcome (N = 501).
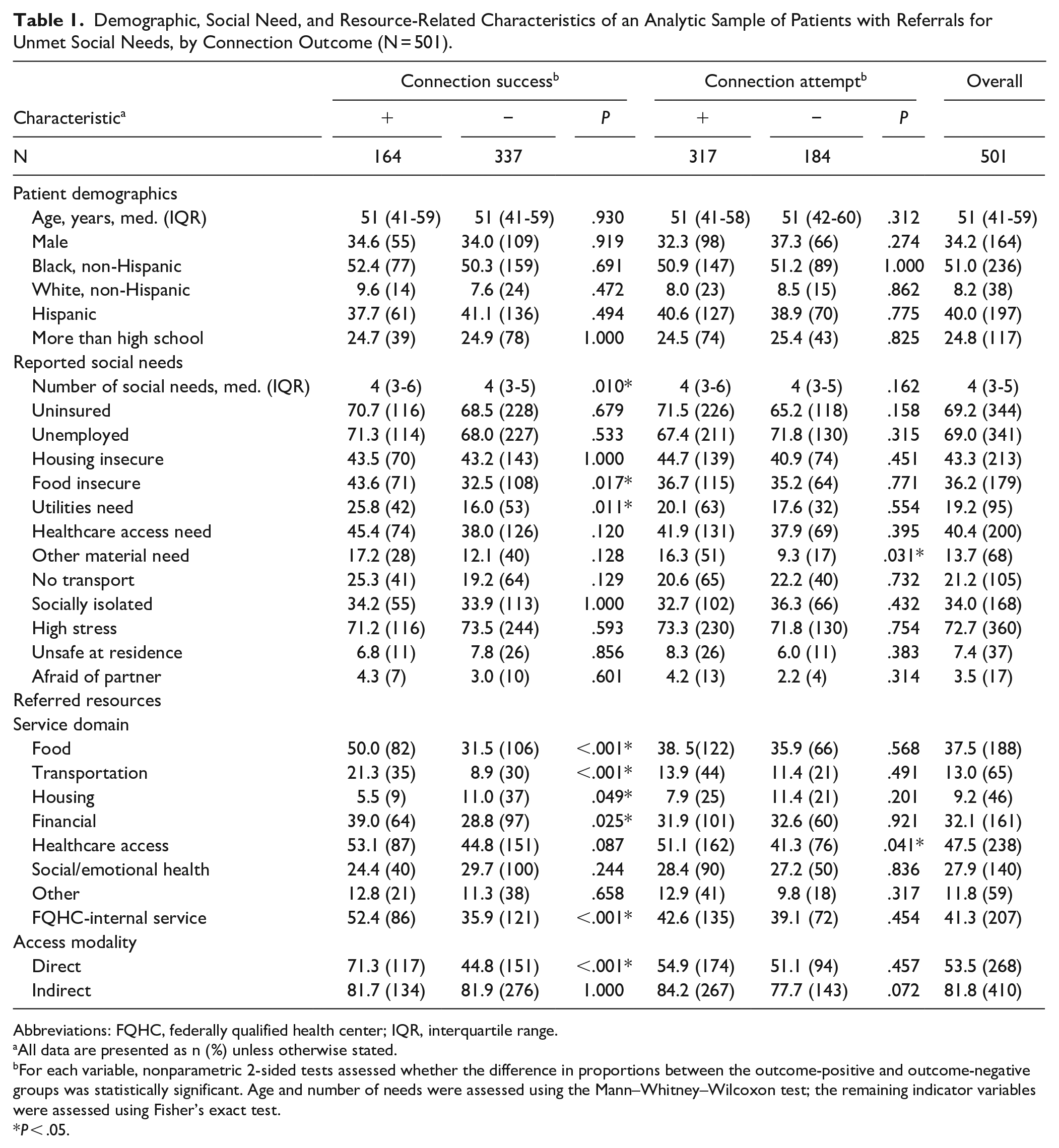
Abbreviations: FQHC, federally qualified health center; IQR, interquartile range.
All data are presented as n (%) unless otherwise stated.
For each variable, nonparametric 2-sided tests assessed whether the difference in proportions between the outcome-positive and outcome-negative groups was statistically significant. Age and number of needs were assessed using the Mann–Whitney–Wilcoxon test; the remaining indicator variables were assessed using Fisher’s exact test.
P < .05.
About one-third of patients (32.7%) in the analytic sample had started services from at least 1 referred resource, the study’s primary outcome. Almost two-thirds of patients (63.3%) had attempted to contact one of their referred resources, whether or not they were able to eventually start services with a resource. The COVID-19 pandemic did not noticeably impact overall proportions of connection success: 32.5% of 286 patients before March 10, 2020 compared to 33.0% of 215 patients after March 10, 2020 (P = .490). Proportions of connection attempt were similar as well: 63.6% of pre-pandemic patients compared to 62.8% of patients during the pandemic (P = .459). For both connection outcomes, differences in patient age, race, ethnicity, and education were not statistically significant.
Connection Success
Social need and resource-related characteristics differed between patients who reported a connection success and those who did not (Table 1). Compared to patients without connection success, it was more common for patients with a connection success to report food insecurity (P = .017) and utilities need (P = .011), as well as more social needs in total (P = .010). Patients with connection success also more often had referrals (1) in the service domains of food (P < .001), transportation (P < .001), or financial assistance (P = .025); (2) internal to the FQHC (P < .001); and (3) with a direct access modality (P < .001). Conversely, it was more common for patients without connection success to have a referral to a resource that addressed housing instability (P = .049).
Unadjusted and adjusted associations between connection success and patient demographic, social needs, and resource-related characteristics are presented in Table 2. In the adjusted analysis, having a referral to a resource that permitted direct access to services (eg, via call or drop-in visit) was associated with a statistically significant increase (aOR 1.95, 95% CI 1.05, 3.61) in the odds of successfully connecting with a referred resource. The following resource-related characteristics were statistically significant in unadjusted analyses only: referral to a resource in food, transportation, or financial assistance service domains and referral to a resource internal to the FQHC.
Unadjusted and Adjusted (N = 423) Associations between Connection Success and Demographic, Social Need, and Resource-Related Characteristics.

Abbreviations: aOR, adjusted odds ratio; CI, confidence interval; FQHC, federally qualified health center; OR, odds ratio.
Model also adjusts for case manager outreach modality (ie, by phone vs in-person) and screening date (ie, before vs after March 10, 2020) to account for programmatic and broader societal changes due to COVID-19.
Hosmer–Lemeshow, P = .6246; c-index = 0.6973, 95% CI 0.6458-0.7488.
P < .05.
Connection Attempt
Among patients who had reported attempting to connect with a resource, it was more common to report “other” material need (P = .031) and to have a referral to a resource for healthcare access (eg, medication assistance programs, Medicaid; P = .041), compared to patients who had not attempted to connect with any referred resource.
Unadjusted and adjusted associations between the connection attempt and patient demographic, social needs, and resource-related characteristics are presented in Table 3. In unadjusted analyses, having a referral to a resource for healthcare access was associated with a statistically significant increase (OR 1.49, CI 1.03, 2.15) in the odds of at least attempting to connect with a referred resource; however, no factors were significantly associated with the study’s secondary outcome in adjusted analysis.
Unadjusted and Adjusted (N = 423) Associations between Connection Attempt and Demographic, Social Need, and Resource-Related Characteristics.
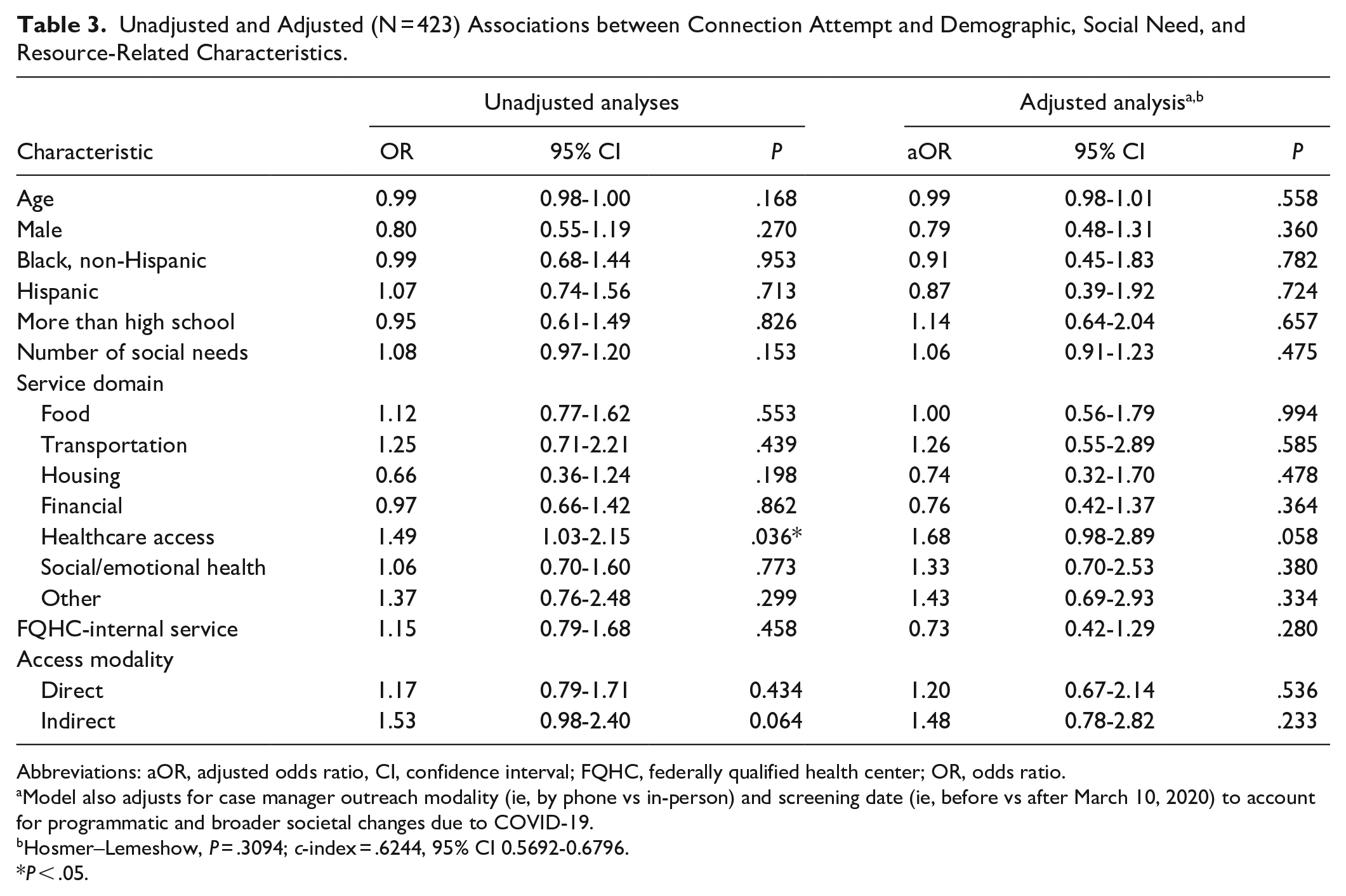
Abbreviations: aOR, adjusted odds ratio, CI, confidence interval; FQHC, federally qualified health center; OR, odds ratio.
Model also adjusts for case manager outreach modality (ie, by phone vs in-person) and screening date (ie, before vs after March 10, 2020) to account for programmatic and broader societal changes due to COVID-19.
Hosmer–Lemeshow, P = .3094; c-index = .6244, 95% CI 0.5692-0.6796.
P < .05.
Discussion
Understanding the factors associated with patients’ ability to access resources for their unmet social needs is a critical implementation consideration for social needs screening and referral programs. In this study, we examined the association between connection success and several demographic, social need, and resource-related factors, repeating the analysis for patients’ attempted connection as an intermediate connection outcome. Only a third of patients reported a successful connection (ie, starting services) with any one of their referred resources. Almost two-thirds of patients reported at least attempting to connect with a referred resource, a total that includes the one-third of patients who had started services. Multivariate analysis identified the access modality of the resource itself as the most significant factor associated with connection success. Referrals to resources that patients could access via phone call or drop-in visit, as opposed to resources that required additional appointments or applications prior to accessing services, were associated with increased odds of a patient starting services within 4 weeks of the initial referral. In unadjusted analyses only, referrals to resources in food, transportation, or financial assistance service domains were also associated with increased odds of connection success, as was a referral to a resource internal to the FQHC. This study did not find statistically significant associations between either connection outcome and patient demographics (age, race, ethnicity, sex, education) or reported social needs in adjusted analysis. These findings suggest that referral pathways may influence the success of patients’ connection to social needs resources, highlighting opportunities for more accessible solutions to addressing patients’ unmet social needs.
The reported proportion of connection success in our study population falls on the lower end of the existing literature, with reported results ranging from 32% to 64% for interventions that screen and refer for multiple social needs in a primary care setting. 19 This may be due to shorter or less frequent follow-up in this study compared to previous studies; however, heterogeneity across the literature in patient population, screening instrument, available resources, and other intervention characteristics complicate comparison. Rigorous operationalization of core intervention components, as well as evaluations of comparative effectiveness, will be crucial as research about social needs interventions continues to advance. 23 The COVID-19 pandemic did not appear to noticeably affect either connection outcome in this study, but a more thorough, particularly qualitative, study of barriers will be necessary to gain a more nuanced understanding of how the pandemic has impacted patients seeking social needs resources.
Of the studies that report connection outcomes, only a few have analyzed the factors associated with a successful connection. Building on previous findings that have identified the importance of programmatic intervention characteristics, such as intervention dosage31,32 and length of follow-up, 32 the present study contributes novel evidence about the characteristics of social needs resources associated with a successful connection. Our results align with early qualitative evidence7,33-35 that it is easier for patients to connect with resources (1) in domains where more immediate solutions are readily available, (2) embedded within a health system as opposed to external to it, and (3) for services with more direct, less complicated pathways for access. In our analysis, the significance of access modality calls attention to intervention points beyond the screening, referral, and navigation activities in the clinical setting, underscoring the need to also consider the accessibility and availability of the resources to which patients are being referred.
These results have pragmatic implications for the design and development of social needs interventions. When offering internal or on-site services is not feasible, the findings of this study support the importance of cultivating robust, streamlined partnerships between FQHCs and CBOs as a means of addressing patients’ unmet social needs.36,37 Communication and collaboration across the socio-medical care continuum could help both sides simplify processes for patients and address gaps in referral pathways where patients are commonly lost. Digital networks at the community and state level represent larger, emerging initiatives to coordinate care between healthcare systems and CBOs, offering centralized platforms to manage referrals, communicate with clients, and track outcomes.38,39 These platforms present an innovative opportunity to facilitate patient connection to an integrated system of health and social services. This will require robust investments in social needs interventions that can complement this developing technological infrastructure, alongside new approaches in workforce development and healthcare financing. 40
Our findings also suggest that it could be beneficial for FQHCs to provide additional case management and administrative support to patients who are required to complete applications or attend appointments in order to access needed services, especially in domains like housing where few resources exist with direct access to necessary services. For example, a strategy employed at the participating FQHC of this study had case managers begin applications for a medication assistance program with patients during their visit, facilitating the process of obtaining affordable medication. Moreover, our findings point to the importance of policy interventions that promote patient enrollment and reduce administrative burden, which often targets poor, Black, and disabled individuals. 41 In particular, the limited capacity of and integration between housing and health systems have long been a challenge, due to bureaucratic and infrastructural barriers as well as silo-ed and insufficient funding structures.42-44
This study has several limitations. First, connection outcome data were based on patient self-report in a conversation with a community resource navigator. Second, community resource navigators were not always in contact with the patient long enough to see the referral through to connection. This is a limitation of the retrospective nature of this study and the program’s protocols, which were designed to ensure continued case management capacity with limited staffing. Third, the external validity of our findings is limited by the single-site study design. Additional studies should be conducted in different community and clinical contexts, with larger sample sizes, and among programs with and without navigator programs. 45
Emerging evidence suggests that social needs screening and referral interventions within routine clinical care have the potential to resolve social needs, improve health outcomes, and reduce avoidable healthcare utilization.46-51 Exactly how and how well these interventions can achieve these outcomes, however, has yet to be established and remains an open and important area of research.23,52 Future directions should include further investigation, both quantitative and qualitative, of the barriers and facilitators of successful connection for different patient populations along specific referral pathways, with additional consideration for the impact of the COVID-19 pandemic. The impact of new technologies, such as digital care coordination platforms or low-cost SMS programs, on connection outcomes should also be evaluated. Finally, future research should continue to bridge evidence about connection outcomes to evidence about social needs resolution, healthcare utilization, and health outcomes in order to inform health care delivery.19,53 Despite recent advances in efforts to integrate across the socio-medical care continuum, healthcare systems must strive to develop interventions and policy that challenge the inequitable structures at the root of unmet social needs and health disparities.
Conclusions
Investigating the drivers of patients’ successful connection to social needs resources is critical to ensure that patients can realize the benefits of referred services. The findings of this study suggest that healthcare systems can best promote successful connection by understanding, strengthening, and simplifying the pathways to access referred resources, which often means building relationships with local CBOs and social service agencies. Specific strategies may include facilitating access to services that require additional applications or appointments, streamlining patient pathways to social service programs internal to the healthcare system, and identifying reliable, accessible resources in social needs domains (eg, housing) where direct access to immediate benefits is less possible. Further study is needed to better understand the factors that facilitate and impede patients’ connection to social needs resources and, importantly, partner with communities to develop and assess interventions that disrupt the systems of inequity that give rise to unmet health-related social needs.
Supplemental Material
sj-docx-1-jpc-10.1177_21501327211024390 – Supplemental material for Factors Associated with Patients’ Connection to Referred Social Needs Resources at a Federally Qualified Health Center
Supplemental material, sj-docx-1-jpc-10.1177_21501327211024390 for Factors Associated with Patients’ Connection to Referred Social Needs Resources at a Federally Qualified Health Center by Tyler Lian, Kate Kutzer, Diwas Gautam, Howard Eisenson, Jane C. Crowder, Emily Esmaili, Sahil Sandhu, Lawrence Trachtman, Janet Prvu Bettger and Connor Drake in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We are greatly indebted to both the behavioral health team at Lincoln Community Health Center (LCHC) and the community resource navigators of LCHC’s Help Desk for making this study possible.
Author Contribution
TL, KK, HE, JCC, JB, SS, and CD contributed to the study conception and design. All authors contributed to material preparation and data collection. Data analysis was performed by TL. All authors contributed to all versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CD reports a financial relationship with ZealCare, Inc.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by the Duke University Bass Connections Fund and the BlueCross and BlueShield of North Carolina Foundation.
Ethical Approval
This protocol was reviewed by the Duke University Health System Institutional Review Board and was determined to be exempt.
Availability of Data and Material
The dataset of this study is not available to the public as it contains confidential and sensitive information of participating patients. A limited dataset without identifiers is available on reasonable request and pending approval from the Institutional Review Board of Duke University. Code is available upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.