
Abstract
Introduction/Objectives:
Asynchronous electronic consultations (eConsults) support primary care providers (PCPs) by providing rapid specialist feedback and improve medically underserved patients’ access to care.
Methods:
This cross-sectional study assessed all eConsults requested over a one-year period at a multi-site federally qualified health center in Texas. We analyzed eConsult content and quality and conducted chart reviews for a randomly selected subsample (n = 100) to determine whether PCPs implemented specialists’ recommendations within 90 days. Semi-structured interviews with PCPs assessed their ability and willingness to follow recommendations.
Results:
There were 367 eConsults submitted by 25 PCPs across 15 adult medical and surgical specialties. Of the 100 charts reviewed n = 77 (77.0%) contained documentation indicating that the PCP had followed at least 1 of the specialist’s recommendations within 90 days. In two-thirds of the cases (n = 66, 66%) the reviewing specialist indicated that a face-to-face referral was not needed. PCPs were most likely to follow recommendations for new medications and least likely to document that they had obtained additional patient history. PCPs noted that they were sometimes unable to follow recommendations when patients could not afford or access treatment or did not return for follow up care, or when they felt that the specialist did not address their specific question.
Conclusions:
eConsults delivered to medically underserved patients in primary care help PCPs provide timely care for their patients. PCPs utilized a broad range of eConsult specialties and generally implemented eConsult specialists’ recommendations within 90 days.
Keywords
Introduction
Federally Qualified Health Centers (FQHCs) form the backbone of the nation’s healthcare safety net, providing high-quality, affordable outpatient care to low-income patients, many of whom lack medical insurance or receive coverage through state Medicaid programs. The Health Center program serves more than 30 million people, including 1 in 5 rural residents and 1 in 3 people living in poverty. 1 While FQHCs improve access to primary care, their patients often struggle to gain access to specialty care.
Uninsured patients who need to see a medical or surgical specialist often must rely on a patchwork of charity care programs or incur substantial out-of-pocket expenses. Many simply forego seeking specialty care at all, often with significant negative long-term health consequences. 2 Additional access barriers include lack of specialists within geographic proximity, long wait times, and the limited number of specialists who will see uninsured or publicly insured patients. 3 Disparities are more pronounced in rural areas, which generally have fewer specialists. 4
Electronic consultations (eConsults) are secure, asynchronous communications that allow primary care providers to submit a clinical question and supporting information about the patient’s case to obtain care and treatment recommendations from a specialist. 5 eConsults are ideal for primary care providers seeking cognitive input and guidance from specialists and have been shown to reduce the need for face-to-face referrals and increase the scope of primary care while saving time and money.6 -8
Texas, 1 of 10 remaining states that has not expanded its Medicaid program, has the highest percentage of uninsured people in the United States, with an estimated 18% of the population under age 65 lacking any form of medical insurance. 9 Previous work has demonstrated that eConsults play an important role in improving access to specialty care for uninsured patients in Texas. 7 Although limited prior research indicates that primary care providers (PCPs) intend to apply guidance received from eConsults in practice,10 -12 less is known about how this intention translates into actual changes in clinical practice. 13
To address this question we conducted a retrospective evaluation of an eConsult program for uninsured patients in central Texas cared for at a large, multi-site FQHC. We address the following research questions: (1) What types of recommendations do eConsult specialists make to PCPs caring for medically underserved patients? (2) Did PCPs take the steps to implement the recommendations in the eConsult? (3) What factors impact PCPs’ willingness and ability to implement eConsult recommendations?
Methods
Design, Setting, and Participants
Design
Cross-sectional study assessing submission quality and outcomes of eConsults submitted and answered between June 1, 2020 and May 31, 2021. The study was approved by the Institutional Review Board at Community Health Center, Inc. (Protocol #1189, 9/23/2021), which granted waiver of informed consent for retrospective analysis of existing eConsult and chart data and approved all procedures for provider interviews, including provision of verbal informed consent. We followed SQUIRE reporting guidelines. 14
Setting
This eConsult program was implemented in 2018 in a large-multi-site FQHC in central Texas to provide access to electronic consultations (eConsults) for uninsured and underinsured patients. eConsults were offered for 15 specialties—allergy, cardiology, dermatology, endocrinology, gastroenterology, hematology, infectious disease, nephrology, neurology, orthopedics, otolaryngology, pain medicine, pulmonology, rheumatology, and urology.
Participants and Data Sources
We collected data on all eConsults submitted for patients age ≥18 and selected a random sample of 100 for further, in-depth chart review. All data were obtained from the eConsult vendor’s platform and the health center’s electronic health record. Semi-structured key informant interviews were conducted with a convenience sample of 9 PCPs on their experiences using eConsults.
Measures
Request Content and Quality
We collected data on specialty and consult question for each eConsult request answered during the study period and evaluated the quality of each request by ascertaining whether it contained summary information about the case and a clearly described consult question.
Response Content
The principal investigator completed inductive content analysis of all eConsult responses to identify the types of clinical recommendations provided by the specialist. Clinical recommendations were grouped into the following categories: face-to-face specialty visit, new medication, change in medication dosage/frequency, vaccination, new imaging, new procedure, additional clinical history, additional laboratory testing, additional physical exam, patient education, and other recommendations.
Recommendation Follow-Up
We collected patient demographic data (age, sex, race, Hispanic/Latino ethnicity, preferred language, and insurance status) for the 100 eConsults selected for chart review and reviewed the electronic health record for evidence that the specialist’s recommendations had been followed within 90 days after receipt of the eConsult. We considered the presence of orders, results, or documentation indicating the intent to implement the specialist’s recommendations as sufficient evidence that the PCP had taken appropriate action to follow the recommendation. Research team members conducted semi-structured interviews with PCPs, during which PCPs commented on their ability to implement eConsult recommendations.
Analytic Methods
The eConsult was considered the unit of analysis for chart review. Descriptive statistics were obtained using Microsoft Excel and SPSS statistics version 27 (IBM, Armonk, NY). We conducted bivariate statistical analyses using χ2 tests and computed post-hoc Fisher’s Exact tests using the method described by Shan and Gerstenberger (2017) and an alpha level of P ≤ .05 with Holm-Bonferroni correction to adjust for multiple comparisons. 15 We used Microsoft Excel and NVivo software (QSR International, Sydney QLD, Australia) to maintain qualitative data for thematic analysis.
Results
Characteristics of eConsults Completed During the Study Period
Twenty-five PCPs submitted 367 eConsults in 15 different specialties during the study period (mean = 14.7, range 1–40). Requests for consultation from gastroenterology (n = 115, 31.3%), rheumatology (n = 45, 12.3%), and hematology (n = 39, 10.6%) comprised over half of all eConsults submitted (54.2%) (Table 1).
eConsults by Specialty (n = 367).

PCPs’ eConsult Requests
PCPs provided brief patient case summaries in about two-thirds of eConsult requests (n = 239, 65.1%), and stated a clear clinical question in about half (n = 192, 52.3%).
Chart Review Sample
The subsample of 100 eConsults selected for further evaluation included requests from 18 PCPs (m = 5.56 eConsults/provider, SD = 4.0) for consultation in 14 specialties. As with the larger sample, gastroenterology was the most requested specialty (n = 27) (Table 1). There were no statistically significant differences between the charts selected for review and the larger sample of eConsults.
There were 97 unique patients in the sample. Most were uninsured (n = 76, 78.4%), female (n = 66, 68.0%), White (n = 65, 67.0%), Hispanic/Latino (n = 49, 50.5%), and preferred to receive care in English (n = 72, 74.2%). The average age of the patient sample was 46.7 years (SD = 14.1) (Table 2).
Demographics of Patients in Chart Review Sample (N = 97 Patients).

The 100 charts reviewed belonged to 97 unique patients. There were 3 patients who each had 2 eConsults in the sample.
PCP Follow-Up on Specialist Recommendations
In total, the 100 eConsults reviewed contained 247 specific recommendations (mean = 2.5 recommendations per case, range 1–6, SD = 1.3). Most consults (n = 66; 66%), suggested that a face-to-face visit with a specialist was not necessary. We observed a statistically significant difference in whether or not a recommendation was followed based on the type of recommendation (P ≤ .001). PCPs were more likely to follow eConsult recommendations for new medications (n = 18, 81.8%, P = .007) and less likely to follow recommendations related to obtaining additional history (n = 0, 0.0%, P ≤ .001). Table 3 shows rates of compliance with specialists’ recommendations by recommendation category.
Recommendations Followed Within 90 Days in Chart Review Sample by Category.
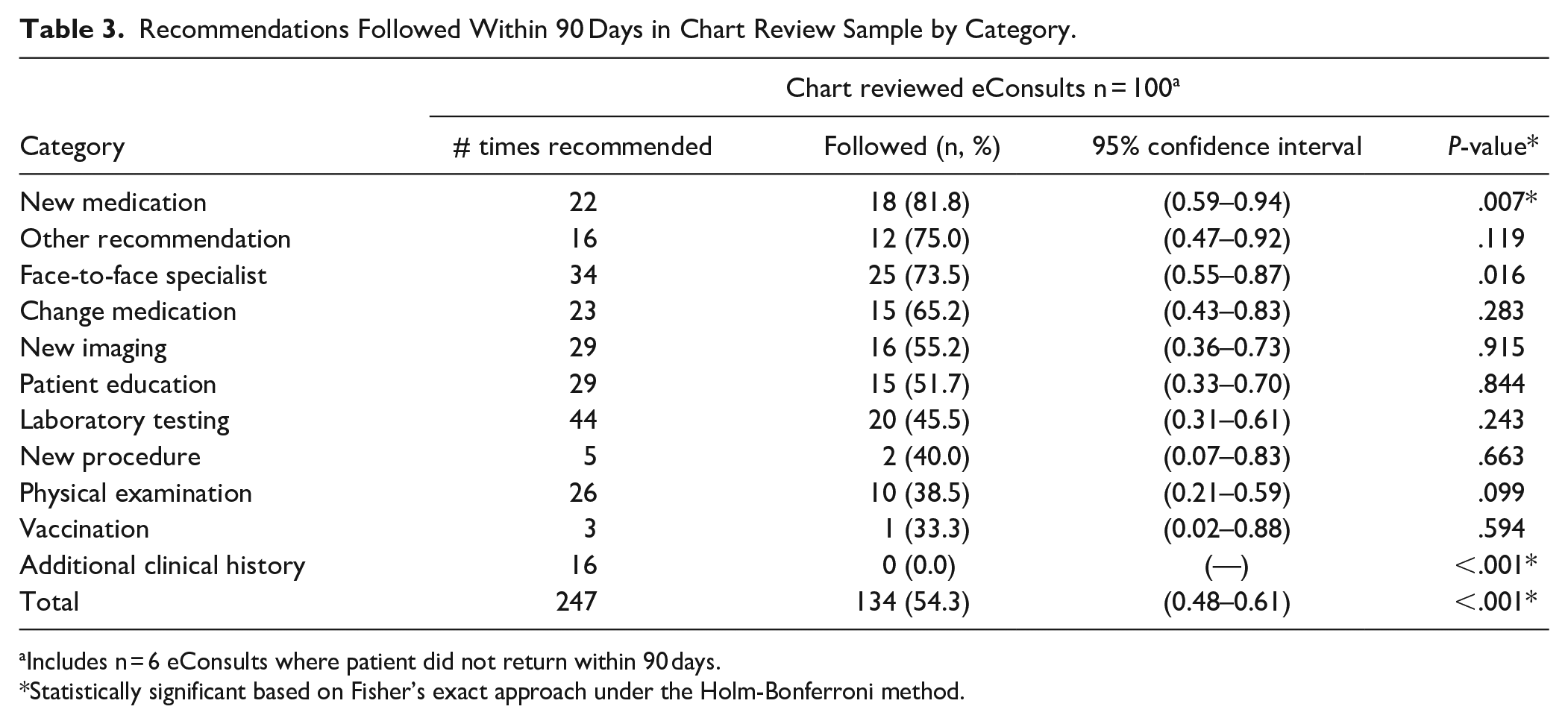
Includes n = 6 eConsults where patient did not return within 90 days.
Statistically significant based on Fisher’s exact approach under the Holm-Bonferroni method.
There was documented evidence in the medical record for 77% of the cases (n = 77) that the PCP had followed at least 1 of the specialist’s recommendations within 90 days, including 42 cases (42.0%) where the PCP followed all of the specialist’s recommendations within 90 days. There were 6 eConsults (6.0%) for which recommendations were not followed due to the patient not returning to the practice within 90 days. Table 4 shows rates of compliance by eConsult specialty.
Recommendations Followed Within 90 Days in Chart Review Sample by Specialty.

Abbreviations: n/a, not assessed.
Includes n = 6 eConsults where patient did not return within 90 days.
Ability and Willingness to Follow Specialists’ Recommendations
Interviewed PCPs confirmed that they were generally amenable to accepting and implementing eConsult specialists’ recommendations. A PCP described a typical discussion with a patient about moving forward with eConsult recommendations and noted the ease of using eConsults to help patients avoid face-to-face specialty visits:
I’ll tell [the patient] that it’s the follow-up for what the specialist recommended [when] they reviewed your records and [that] they agree with the plan so far. [Or] that we’re doing this, this, and this, or they recommend we should test this, and do this . . . I just reviewed one [with a patient], and she was like, “Okay, So we have plans for the next step.” And everybody just—they seem agreeable. They say “okay,” they say they understand, and we go forward with the process. I have not had anyone who says, “but I wanted to see someone in person.” No one has been upset or seemed confused. It just seems to go well from my experience. (PCP #1)
A second PCP confirmed that when they requested an eConsult, they intended to follow the specialist’s recommendations:
Before I put in that referral I explain [to the patient] that we have access to a group of consultants or specialists who are remote and all I have to do is send them details of what’s going on with you with your labs and your imaging and all of that and they’ll give me recommendations based on what I send. And when that recommendation comes in, I’m gonna invite you back, and we’re gonna talk about what they want us to do. (PCP #6)
Although PCPs generally appreciated eConsult recommendations and expressed intent to implement them, some also provided insight on reasons they might decline to follow a recommendation.
Several described receiving eConsult recommendations that were medically appropriate but impracticable for their low-income, uninsured patients:
I have had some [eConsult] specialists send me a message back saying, “you just need to send that patient for a face-to-face with the specialist.” But I can’t though. (PCP #2)
Another agreed:
Sometimes they’ll recommend certain medications that are far out of a patient’s ability to purchase. Though I understand giving that as an option. (PCP #5)
A third voiced frustration with a response that assumed the patient would have access to a specialized test:
You’re not gonna be telling me get the electrical whatever when clearly this patient doesn’t have access to that. There is no way. When you tell me she has to get this kind of imaging—she can’t get that. (PCP #6)
PCPs also expressed that specialists’ responses did not always address their case-specific clinical question. One observed:
The most helpful consults are the ones that are tailored to what you say. A few of them have been like cut and paste, cut and paste, with no specificity to your case, and they’re not very helpful. (PCP #8)
Two others described the challenge of formulating eConsult questions. One reflected that PCPs had gradually become more accustomed to using eConsults to help with care planning versus just asking for help:
So it’s building up and using [the eConsult] as a source of “okay, what’s next?” Not only, “what should I do?” but “did I do all the tests I need to do to get the complete picture?” (PCP #9)
Another posited, “Our eyes are not always trained for what we’re looking for when it comes to specialty care” (PCP #7).
PCPs also confirmed that they might be unable to implement a recommendation if the patient did not return to care on schedule. A PCP offered, “A telephone call is usually not sufficient enough to go into the extent we need to” (PCP #7). Another noted:
I’ve sent eConsults and I’m waiting on the patient to come on back in again for months . . . I have a responsibility to provide a patient with outstanding care, and that patient has a responsibility to maintain a follow-up and consistency in taking care of themselves as well. (PCP #3)
Discussion
eConsults address specialty care access challenges and improve the efficiency of referral and consultation. We observed that PCPs submitted eConsults across a broad variety of specialties with the intent of following the specialists’ recommendations, and demonstrated that specialty eConsults provided guidance that PCPs were able to implement in primary care. In two-thirds of cases analyzed in this study, eConsult specialists offered recommendations that could be implemented by the PCP in primary care. This is particularly important for uninsured patients who often have very few options for obtaining face-to-face care from specialists, and is consistent with literature showing that eConsults have a positive impact on uninsured patients’ access to care.7,13
This study was conducted in an FQHC treating a large proportion of rural, uninsured patients. Insufficient access to specialty care perpetuates health care inequality for uninsured and under-insured patients who may be unable to pay for specialty care, and may experience stigma associated with being poor and/or uninsured when seeking care.16 -18 Rural patients experience additional systematic barriers including lack of specialists willing to care for them, long wait times, travel distance, and lack of transportation.4,19 eConsults can help circumvent provider shortages in these settings.20,21
Comments from the PCPs we interviewed reinforced our chart review findings. PCPs affirmed their appreciation for eConsults and their intent to act on eConsult specialists’ recommendations, but noted that their patients’ inability to access or afford some types of treatment impacted whether they would incorporate the recommendation into their treatment plan. We observed during chart review that PCPs implemented higher proportions of recommendations for new medications, face-to-face specialist visits, and medication frequency/ dose changes versus recommendations to order procedures or laboratory testing, which would likely be more complex and costly for uninsured patients to follow. This may reflect PCPs’ sensitivity to the cost and access barriers that some types of treatment recommendations would impose on their uninsured patients, and their willingness to account for their patients’ needs and preferences.22,23
Our findings confirm that clear communication between primary care provider and specialist helps ensure that patients receive care.24,25 Our observation that approximately one-third of the eConsults analyzed did not contain a clear clinical question and only half contained a case summary aligns with findings from a 2022 study by Timmins et al., where over 20% of 4866 PCP survey respondents reported sending clinical information to a specialist about the patient’s condition either “sometimes,” or “seldom or never.” 26 Qualitative interviews affirmed that some PCPs in our study had difficulty formulating a question for the specialist, which could have impacted the specialist’s response, and may help account for comments that some eConsults didn’t address the submitter’s specific clinical concern. Increasing the proportion of eConsult requests with a clear clinical question and case summary is likely to increase the specificity of eConsult responses and further improve their usefulness to PCPs.
Strengths of our study include its real-world pragmatic assessment of PCP use of a breadth of available eConsult specialties to serve a high-need, medically underserved population, and its examination of electronic health record data to determine whether PCPs implemented eConsult specialists’ recommendations.
Our study is limited by its focus on a small sample size at a single organization over a one-year period. In addition, the distribution of eConsults in this cohort is unique with respect to eConsult specialty, clinical conditions, questions, and disease states represented, which may limit the generalizability of these findings to other practice settings. Our assessment of whether or not a PCP followed a specialist’s recommendation within 90 days may underestimate the frequency with which PCPs follow specialty recommendations as it relied on information documented in the EHR. We were not always able to determine whether the suggested test or treatment was actually completed. As such, we were evaluating the primary care provider’s intent to implement the plan and their taking appropriate action to implement the plan.
Analysis of treatment outcomes beyond 90 days post-eConsult was outside the scope of the study. Further research is needed to examine the impact of eConsults on patients’ care utilization, including need for a subsequent specialty visit further in the future. Our study included eConsults submitted for a variety of specialty care conditions and our sample size was not sufficient for statistical analyses comparing treatment outcomes between specialty conditions. Future research should examine eConsults’ impact on care for specific specialty conditions, including longitudinal patient clinical outcomes, and should capture outcomes across a larger sample, with a focus on the impact of implementing disease-specific recommendations.
This study demonstrated substantial, positive impact on care for uninsured patients living in largely rural locations who are at particular risk for delaying or deferring needed care, and showed that eConsults result in actual changes in medical care that are implemented by the PCPs. PCPs utilized a broad range of eConsult specialties and generally complied with eConsult specialists’ recommendations within 90 days.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319231202201 – Supplemental material for Impact of eConsults on Clinical Care in Primary Care: A Cross-Sectional Analysis of Primary Care Provider Behavior
Supplemental material, sj-docx-1-jpc-10.1177_21501319231202201 for Impact of eConsults on Clinical Care in Primary Care: A Cross-Sectional Analysis of Primary Care Provider Behavior by Lauren Bifulco, Olivia Guidotti, Idiana Velez, Lynsey Grzejszczak, Tracy Angelocci, Lola Okunade and Daren Anderson in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We acknowledge Rocio Davis, BA at Lone Star Circle of Care, the ConferMED referral team for coordination of eConsults, and Giuseppe Macri, BA and Jose Montoya, MS for eConsult data management support. We thank Patricia (Pat) Ward, RN at Lone Star Circle of Care for providing chart review training and for providing clarification and disambiguation in response to data quality inquiries.
Author Contributions
• Lauren Bifulco, MPH—Drafted manuscript, study design, data collection, data analysis
• Olivia Guidotti, BA—Data Collection, manuscript preparation
• Idiana Velez, BSBM—Data Collection, manuscript preparation
• Lynsey Grzejszczak, MHA—Data Collection, manuscript preparation
• Tracy Angelocci, MD—Study design, data collection oversight, reviewed drafts of manuscript to provide line edits
• Lola Okunade, MD—Data collection oversight, reviewed drafts of manuscript to provide line edits
• Daren Anderson, MD—Drafted manuscript, developed research question, study design, data collection oversight
Data Availability Statement
Data are available from the corresponding author, D.A., upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: L.B., O.G., I.V., and L.G. have no conflicts of interest to report. L.O. is currently the Medical Director of Family, Adult, Convenient Care and Vision Care at Lone Star Circle of Care. T.A. was formerly the Chief Medical Informatics Officer at Lone Star Circle of Care. D.A. is the President and Founder of ConferMED, a non-profit specialty eConsult network, and the owner of ConferMED PC, a practice group responsible for delivering eConsults to its clients.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding to conduct and evaluate eConsults was received from the St. David’s Foundation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.