
Abstract
Introduction/Objectives:
With redistribution of resources and time during the COVID-19 pandemic, the Thrive Bridge Clinic altered its focus, alongside the changes in the healthcare system and needs of the population. This paper describes how the Thrive clinic services have been altered between 2019 and 2022 as a result of COVID-19.
Methods:
Data was collected via retrospective chart review of patient encounters.
Results:
Following the onset of the COVID-19 pandemic, utilization of acute medical triage decreased while community resources requests increased. Of the community resources requested, all services increased with the largest increase being transportation. Primary care, specialty medical care, legal assistance, and substance use were additional topics commonly discussed.
Conclusion:
Social support and community resource requests now act as the primary focus of the Thrive Bridge Clinic following the COVID-19 pandemic. Future studies can focus on better understanding whether these resources truly reflect patient needs and how often resources that we refer are being utilized.
Keywords
Introduction
Founded by students at the Lewis Katz School of Medicine at Temple University (LKSOM)], the Thrive Bridge Clinic provides acute medical triage care and addresses barriers to healthcare for residents at the One Day at a Time shelter (ODAAT). The shelter is an organization for homeless individuals with concurrent substance use disorder. The in-person Thrive Bridge Clinic is separated into 5 stations that all provide different aspects of care to the patients. These teams include Check-In, Vitals, Medical Team, Opioid Wellness Liaisons (OWLs), and Community Resource Liaisons (CRLs). A figure of the clinic flow and layout can be seen below (Figure 1). Patients are not required to visit all 5 stations but are instead encouraged to stop by stations that could address their primary concerns. At check-in, patients are introduced to the services offered at the clinic. At the vitals stations, patients are screened for abnormal vital signs, including hypertension and hyperglycemia. The medical team is composed of volunteer medical students and physicians, who are available to counsel and provide over-the-counter medications to patients for acute concerns. The Thrive Bridge Clinic’s Community Resource Liaisons (CRLs) discuss long-term social goals with patients and assist in scheduling health care and dental appointments, obtaining health insurance, coordinating transportation, finding legal resources, and obtaining driver’s licenses and other forms of identification. Founded in January 2022, Opioid Wellness Liaisons (OWLs) specialize in substance use disorder support and resources. Outside of Thrive Bridge Clinic, OWLs and CRLs contact community services on behalf of patients to schedule appointments. In addition to connecting ODAAT residents to substance use support, OWLs also distribute Narcan to clinic participants.

Thrive bridge clinic stations and clinic flow.
On top of the general difficulties that patients face navigating the healthcare system, North Philadelphia faces increased poverty and housing insecurity, resulting in increased all-cause mortality rates and decreased life expectancy. 1 Consequently, one of the main aims of the Thrive Bridge Clinic is to act as a collaborator between ODAAT residents and the healthcare system. Through its services, Thrive CRLs aim to reduce health disparities, hospitalizations, and cumulative healthcare costs. 2 While many pop-up clinics are unable to provide long-term care, Thrive Bridge Clinic connects individuals to resources within the community to improve healthcare access and longitudinal care.
During the COVID-19 pandemic, the clinic was faced with the challenge of supporting the North Philadelphia community while maintaining safe distancing protocol. Due to this constraint, a shift in operation and services took place from the fall of 2020 to March of 2022, wherein the Thrive Bridge Clinic operated exclusively through telehealth. Telehealth services were limited to the CRL team. The Thrive Bridge Clinic returned to in-person operations in the spring of 2022, adopting telemedicine as a contingency for COVID-19 outbreaks or any other barriers to in-person operations. Throughout all of 2022, the clinic was challenged to re-establish itself as a clinic while also meeting the ever-changing needs of this marginalized population. With redistribution of resources and time during the COVID-19 pandemic, the Thrive Bridge Clinic altered its focus, alongside the changes in the healthcare system and needs of the population. This paper describes how the Thrive clinic services have been altered between 2019 and 2022 as a result of COVID-19.
Methods
A retrospective data analysis was performed to compare patient encounters and CRL services between 2019 and 2022, before and after COVID-19. All patient encounters from January to December 2019 and January to December 2022 were extracted from AirTable, a de-identified database used during each encounter to keep track of resources utilized with the patients. This information was filled out at the beginning of each patient encounter to track the patient’s progress through their desired stations. No encounters were excluded and those lost to follow-up while going through the stations were considered not visited at those stations. Data was then collected for the total number of encounters, patients, and a breakdown of the number of encounters for each individual clinic station. Data collected in a separate CRL-specific AirTable survey was also extracted from PracticeFusion, an electronic medical record utilized within the clinic, for all encounters that included CRL and/or OWL visits from January to December 2019 and January to December 2022. The CRL survey collected data about issues discussed during every CRL encounter including primary care, specialized medical care, legal/identification concerns, health insurance, substance use, transportation, mental health, and other. All data was compiled and analyzed using Microsoft Excel.
Results
In 2019, there were 336 individual patients seen over 891 encounters. Follow-up appointments either addressed the same concern or focused on a new concern. In comparison, in 2022 there were 221 individual patients with 544 patient encounters. The total number and percent of total encounters of both medical team encounters and CRL/OWL encounters for 2019 and 2022 can be seen in Figure 2.
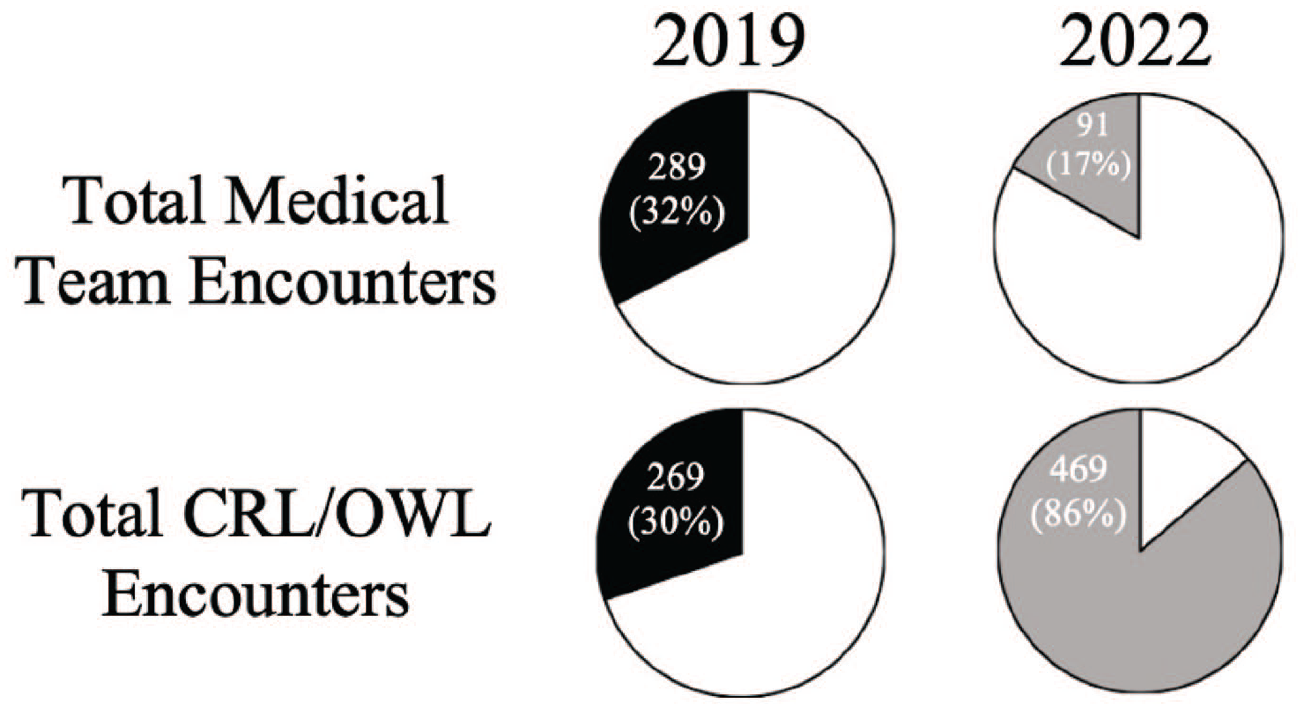
Clinic service statistics of services provided in 2019 and 2022 compared to total number of encounters.
The distribution of resources discussed during CRL encounters in 2019 compared to 2022 is seen in Figure 3. While nearly all topics discussed from 2019 to 2022, transportation saw the largest increase followed by legal/identification services. All CRL topics increased except “other” which included a broad range of topics including general health guidance, clothing, housing, and employment.

CRL/OWL topics discussed during clinic encounters in 2019 and 2022.
Discussion
Prior to 2020, Thrive Bridge Clinic acted mainly as a triage center with only 30% of patients engaging in longitudinal health care connection and social assistance with the CRLs. Following the COVID-19 pandemic, Thrive Bridge Clinic refocused their community resource efforts, resulting in 86% of clinic encounters having CRL involvement. In comparing 2019 to 2022, CRL encounters increased by about 75% in just 3 years. This change reflects a combination of changes to the medical system, the patient’s needs, and the services provided by the clinic. In 2022, the in-person clinic was dependent on the COVID-19 pandemic and ODAAT regulations surrounding gathering in-person. Consequently, the clinic ran with reduced student staffing for 2022. This contributed to a significant reduction in total patient encounters when comparing 2022 to 2019. In addition, only CRL telehealth services were available from March 2020 to March 2022, accounting for 156 of the 469 encounters (33%) which also relatively decreased the number of medical team encounters and increased the number of CRL encounters. In the coming years, patient encounters are expected to continue to increase alongside CRL visits with the return to full in-person operations.
The topics discussed at CRL encounters also changed from 2019 to 2022, as seen in Figure 3. Of the various social needs of our patients, transportation was found to be the most addressed and largest growing CRL topic from 2019 to 2022. Those with low socioeconomic status and chronic medical conditions have been found to be more at risk of transportation being a barrier to accessing medical care.2 -4 To mitigate these barriers for Thrive patients, the clinic provides bus passes and assists patients in applying for reduced bus fare programs. While these services were both present in 2019, an increased budget in 2022 as a result of reduced expenses during COVID-19 allowed bus passes to be offered alongside every appointment discussed or scheduled through our clinic. One of the largest and most consistently high services provided by the CRLs from 2019 to 2022 was medical appointment referrals and/or scheduling Although there are many primary care providers in the area, there continues to be a disconnect between health care services and the community. 5 This disconnect has only grown in recent years since COVID-19, with residents of Philadelphia experiencing increasing wait times for appointments and greater numbers of gaps in preventive services. 1 While the medical staff at the clinic is helpful in triaging acute medical problems, Thrive Bridge Clinic cannot provide the depth of care required for a full primary care work-up, especially in the management of long-term medical conditions such as hypertension and diabetes. Consequently, many patients seen are set up with a primary care provider to address these gaps in care. In addition, Thrive Bridge Clinic also assists in establishing specialty medical care. The most utilized specialties include dentistry, addiction medicine, mental health, ophthalmology, podiatry, dermatology, and physical therapy. In comparison to 2019 where patients were provided with contact information for any medical appointments they needed to schedule, CRLs during 2022 actively scheduled appointments on behalf of the patients. This change was first made possible by online and/or streamlined scheduling processes popularized during COVID-19. Now, this practice has continued in an effort to increase follow-through attending primary care and specialty care appointments that these patients needed. To further increase compliance with attending appointments, especially those far out, patients were given appointment card reminders the week of their appointments along with any needed bus passes.
Personal identification, the fourth most common resource referred to patients in 2022, remains an important and often overlooked barrier to health care access in both 2019 and 2022. Lacking forms of personal identification is a barrier to having a bank account, employment, housing and even medical care, particularly for people experiencing homelessness.6,7 The CRLs connect patients with local governmental agencies and free-of-cost legal programs are especially helpful when the lack of legal documentation, such as a social security card or birth certificate, is a barrier to medical care, housing, and employment.
While these provisions helped connect patients to long-term healthcare, they did not fully address many of the underlying confounding concerns of substance use disorders in the Thrive Bridge Clinic’s patient population at ODAAT. Unintentional drug overdose contributes significantly to premature mortality rates and a decrease in life expectancy in North Philadelphia. 8 In 2021, Philadelphia experienced 1276 unintentional drug overdoses, a 5% increase from 2020. 8 The Philadelphia zip codes with the 5 highest number of overdose fatalities in 2021 all reside within North Philadelphia. 8 In response, the OWLs were founded and trained to specifically address substance use resources and concomitant social needs. From their creation in January 2022 through December 2022, the OWLs had 22 patient encounters. The OWLs also provided approximately 576 naloxone nasal sprays to patients during clinic. While only a small percentage of the total patient population seen at the clinic, it is a starting point for the Thrive Clinic to provide substance-use focused counseling and resource management to these at-risk patients.
Finally, when further looking at Figure 3, the other category was largely the same between 2019 and 2022. Even still, this represented a change in what topics were discussed. In 2019, a large portion of this other category consisted of counseling patients on general health questions and medication compliance. By 2022, patient education was no longer as emphasized and instead saw increases in housing and employment.
Conclusion
Although the Temple University Hospital is in the heart of North Philadelphia, the surrounding community remains underserved with increased healthcare barriers. 9 A major barrier to accessing healthcare is an inability to navigate a complex system. 1 Even when resources are present, patients may have difficulties identifying programs they qualify for and physically accessing them. 1 While the clinic had a system to address these longitudinal concerns prior to COVID-19, clinic changes during and following the pandemic have allowed rapid expansion of these community resource services. With the addition of the OWLs program, the Thrive Bridge Clinic has better understood and addressed the complex substance use and concomitant social needs of this patient population. This shift is in line with the goals of the Thrive Bridge Clinic to encourage long-term health wellness in its patient population.
While many student-run and community clinics offer patient advocacy and community resource services, most primarily focus on acute medical and primary care.10,11 In comparison, the Thrive Bridge Clinic now predominantly serves to assist patients with social support. The changes made within the Thrive clinic during 2022 focus on the specific needs of the clinic’s patient population, such as scheduling appointments on behalf of the patients, providing bus passes, creating appointment cards, and having volunteers specialized in substance use resources. These specialized services geared toward the clinic’s at-risk patient population distinguish our clinic and can serve as an example of how to further improve other similar clinics. Future studies include assessing whether patients feel their needs were adequately met given the increased usage of community resources and known distribution of clinic services.
Footnotes
Non-Author Contributors
Volunteers at the Thrive Bridge Clinic collected data and provided care to study patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research and publication of this article was supported by the Greenfield Foundation.
Ethical Approval and Informed Consent
This study was waived from IRB approval on March 12, 2024, by the Temple University IRB. All patient information was de-identified and patient consent was not required. Patient data will not be shared with third parties.
Data Availability Statement
Access to all de-identified underlying research materials is available at request.