
Abstract
Background:
Food insecurity (FI) affects health outcomes, yet screening in primary care remains limited and little is known about how patients view the physician’s role. This study examined patient comfort and expectations with FI-related care.
Methods:
A cross-sectional survey of adult patients was conducted at family medicine clinics in New Jersey. The survey assessed patient comfort and expectations regarding FI discussions. Associations were analyzed using ANOVA and probit regression.
Results:
Among 250 respondents, 17.2% screened positive for FI. Few participants reported previous FI screening (1.2%), discussions with their primary care provider (1.2%), or referrals to FI resources (1.6%). Most respondents felt comfortable discussing FI. Patients identified roles for physicians in screening (24%) and providing referrals (37%).
Conclusions:
FI was common, yet screening, discussion, and referral rates were low despite patient comfort with physician involvement. Integrating patient perspectives into screening may improve FI identification and support within family medicine settings.
Keywords
Introduction
Food Insecurity (FI) is defined as limited or uncertain access to adequate food. 1 FI has been associated with adverse health outcomes, including increased risk of obesity, diabetes, hypertension, cardiovascular disease, depression, and higher health care utilization and costs. 2 In 2024, 13.7% of US households—18.3 million households—experienced food insecurity. 1 Despite its associations with adverse health outcomes, FI remains under addressed in routine primary care visits.3,4 The Hunger Vital SignTM, a validated 2-item screening tool for FI, has been incorporated into some electronic medical record systems, but screening remains inconsistent.5,6 In a 2019 cross-sectional study, only 29.6% of physician practices and 39.8% of hospitals reported screening. 7 Despite inconsistent implementation, some state Medicaid programs and managed care organizations have incorporated social risk screening expectations or incentives through state plan authority and Section 1115 waivers, reflecting growing policy recognition of food insecurity as a health-related social need. 8 This gap limits opportunities for patients to connect with resources and challenges family medicine’s holistic approach to care.
While literature acknowledges the role of primary care providers (PCPs) in addressing FI, studies have traditionally focused on the physician perspective. 9 Commonly cited barriers include lack of time, competing priorities and limited resource knowledge.3,4 The patient perspective, how patients view the physician’s role in addressing FI, remains underexplored.10,11 Factors such as comfort and expectations of physician involvement may shape whether FI screening is feasible and effective.
To address this gap, we conducted a cross-sectional survey of patients in 2 family medicine clinics in southern New Jersey. The primary aim was to evaluate patient perspectives on physicians’ roles in addressing FI, including comfort, perceived importance, expectations, and barriers.
Methods
The study was conducted between May 2023 and December 2024 at 2 family medicine clinics in southern New Jersey. Adults aged 18 years and older who could complete the survey in English were recruited during routine clinic visits and invited to complete an anonymous Qualitrics survey. Anyone under the age of 18, or who were unable to complete the survey independently, were excluded. The study was conducted using tablets provided by study staff. Staff would introduce the survey at the start of office visits, before being seen by the physician, and consent was obtained prior to the start of the survey. Participants did not receive any incentive for completing the survey. The study was IRB approved.
Food security status was assessed using the Hunger Vital Sign tool. 5 Participants were classified as food insecure if they responded “often true” or “sometimes true” to either of the following:
“Within the past 12 months, we worried whether our food would run out before we got money to buy more,”
“Within the past 12 months, the food we bought just didn’t last and we didn’t have money to get more.”
The remainder of the survey was developed by study staff. Data were analyzed using STATA 12 with ANOVA and probit regression.
Results
Among 250 survey respondents, 43 individuals (17.2%) screened positive for FI. Income was the strongest correlate (P < .001): 56.7% of respondents earning <$25 000 annually were food insecure versus 3.5% earning >$100 000 (Table 1). Among participants with only a high school diploma, 28.7% screened positive for FI, compared with 10.1% of college graduates (P = .025). Similarly, 50% of participants reporting poor health screened positive, compared with 10.7% of those reporting good health (P = .006). Gender and race were not statistically significant, although FI rates trended higher among Black respondents (26.1%) than White respondents (14.8%).
Participant Demographics.
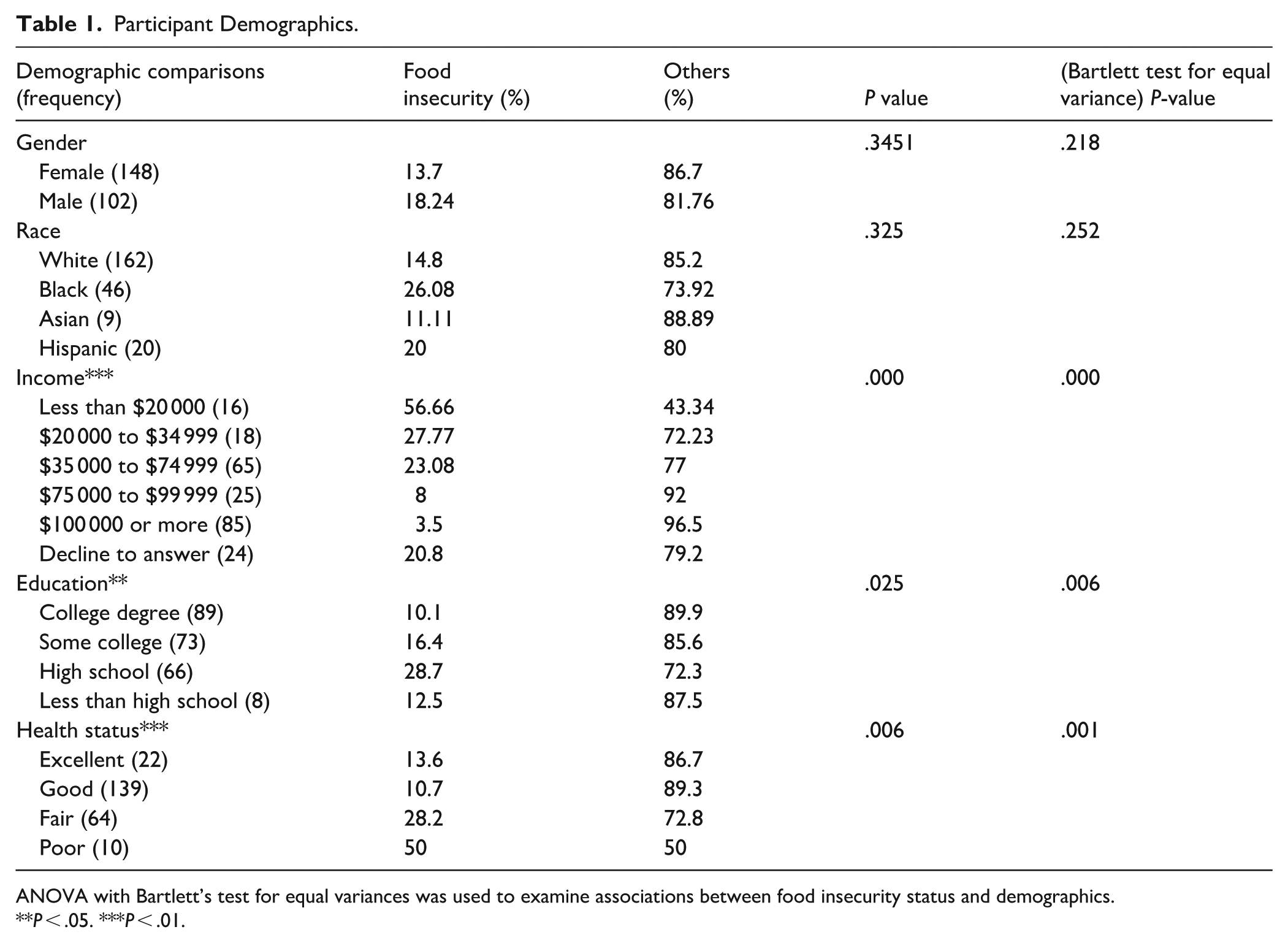
ANOVA with Bartlett’s test for equal variances was used to examine associations between food insecurity status and demographics.
P < .05. ***P < .01.
Notably, few participants reported being screened or discussing FI with their PCP (Table 2). Only 3 (1.2%) reported ever discussing FI (P < .001), 3 (1.2%) reported formal screening, and 4 (1.6%) reported receiving a referral or resource recommendations; all 4 participants were food insecure. Overall, the majority of respondents felt comfortable discussing FI with their provider (Table 2). Among food insecure participants, 43% felt “very comfortable” versus 18% felt “very uncomfortable.” When asked about the importance of addressing FI during visits, most respondents were either neutral or did not view it as important. Regarding physicians’ roles, 24% of respondents believed physicians should identify at-risk patients (n = 60), 37% believed physicians should provide referrals to resources (n = 92), 2% believed physicians should directly provide food assistance (n = 4), and 27% endorsed “all of the above” (n = 67). Food insecure respondents were represented in each of these groups except direct food provision.
Patient Perspectives and Experiences Related to Food Insecurity.

Abbreviation: PCP, primary care provider.
ANOVA with Bartlett’s test for equal variances was used to examine associations between food insecurity status versus patient perspectives and experiences with primary care providers.
P < .05. ***P < .01.
Respondents indicated a number of different perceived barriers to food insecurity discussions with their PCP’s. Among the possible barriers, the most commonly stated potential barriers include “lack of time during appointments” (82), “lack of training or knowledge about resources” (64), “patient reluctance to discuss food insecurity” (127), and “insurance or payment restrictions” (82).
Logistic regression analysis confirmed several independent predictors of FI (Table 3). Age, Income over $100 000, and “Good” Health Status are the only variables that are statistically significant at the 95% confidence level. For every 1-unit increase in age, the odds of the outcome (food insecurity) decrease by approximately 6% (OR = 0.9401). Individuals in the highest income bracket ($100 000) have significantly lower odds (OR = 0.0951) compared to the reference group. Those reporting good health have 64.7% lower odds (1 − 0.3527) of the outcome compared to others. Compared to White respondents, Black participants were found to have a higher odds ratio (2.58) to report FI (P < .10).
Logistic regression results examining the association between food insecurity and the socioeconomic and demographic variable, reporting estimated odds ratios to interpret the magnitude of effects
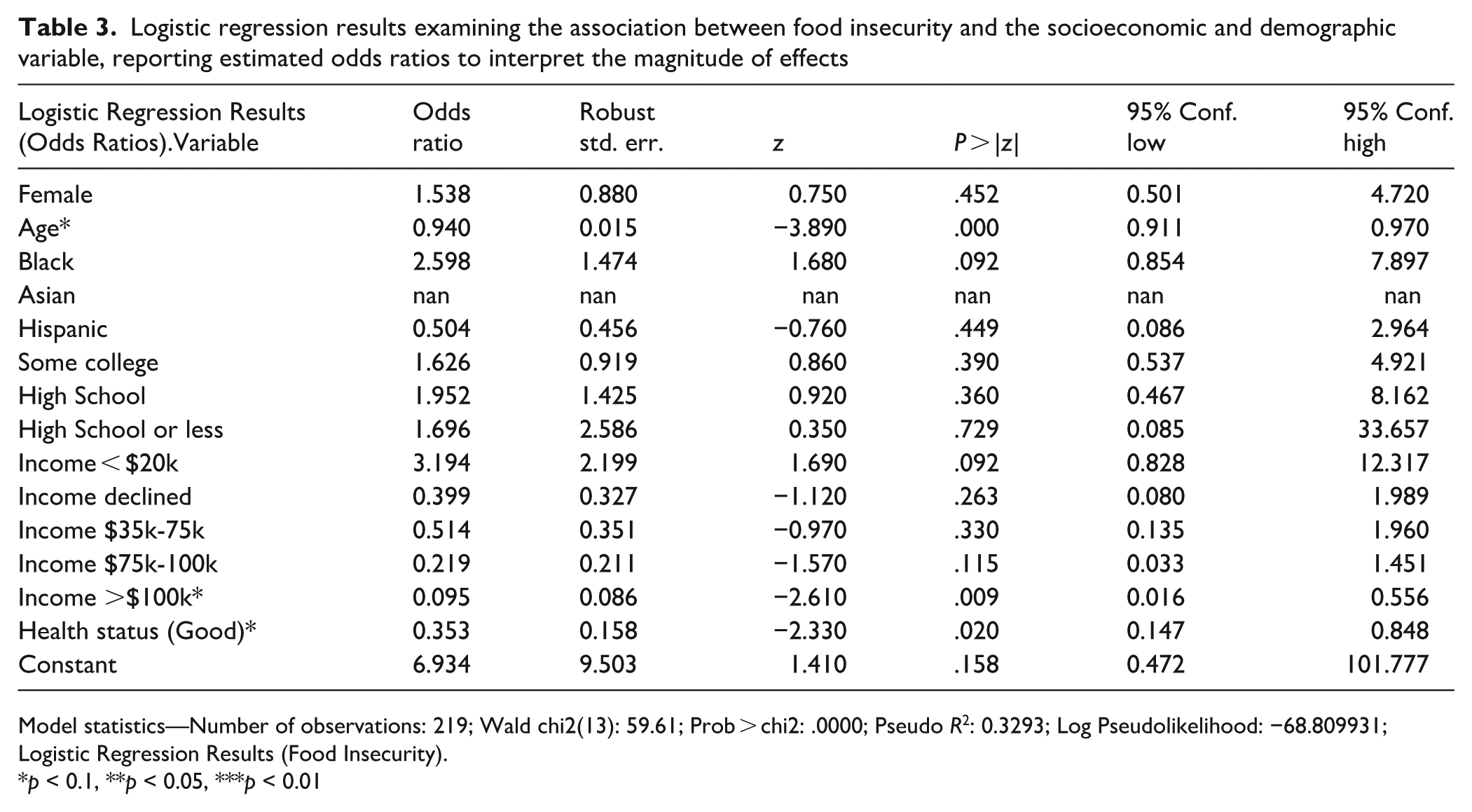
Model statistics—Number of observations: 219; Wald chi2(13): 59.61; Prob > chi2: .0000; Pseudo R2: 0.3293; Log Pseudolikelihood: −68.809931; Logistic Regression Results (Food Insecurity).
p < 0.1, **p < 0.05, ***p < 0.01
Discussion
This study highlights the prevalence of FI and patient perspectives on physicians’ roles in addressing it as a social determinant of health. Nearly 1 in 5 surveyed patients screened positive for FI, consistent with national trends across diverse populations. 1 In line with existing research, FI was strongly linked to lower income, lower education, and poorer self-reported health. 1 These findings illustrate how socioeconomic factors shape health outcomes and reinforce the role of family physicians in identifying and addressing FI in primary care. 9
Prior studies examining patient perspectives on FI screening in primary care have similarly demonstrated high levels of patient receptivity. Kopparapu et al. found that most patients valued screening and preferred referral to food banks or financial assistance programs, and that screening was unlikely to harm the physician-patient relationship. 13 Similarly, Kress et al, using qualitative interviews, reported that patients viewed screening and referral to community resources as helpful, and noted that screening often facilitated conversations patients might not otherwise initiate. 11 Our findings are consistent with this literature demonstrating that patients are generally comfortable discussing food insecurity and supportive of physician involvement. However, our study extends prior work by quantitatively examining perceived barriers alongside real-world screening and referral rates within family medicine clinics. In doing so, we highlight the persistent gap between patient openness and low real-world rates of FI screening and referral implementation, suggesting that structural and workflow-related factors may represent more substantial barriers than patient reluctance.
Despite the recognized burden of FI, our results show low rates of physician-initiated screening, discussion and referral. Few participants reported being asked about food needs or referred to community resources, mirroring national data showing fewer than 40% of physician practices and hospitals routinely screen. 6 Most patients were comfortable discussing FI and viewed physician involvement as important, suggesting receptivity is not a major barrier. This contrasts with physician concerns about stigma or patient discomfort. 9 The persistence of low screening rates despite patient openness likely reflects a gap within structural and system-level factors, which may include limited visit time, lack of education or training, inadequate reimbursement, and poor referral infrastructure. The gap between patient openness and clinical practice represents a missed opportunity for intervention. Importantly, these findings suggest that patient reluctance may not be the primary barrier to screening, shifting attention toward system-level and workflow-related factors that are more amenable to intervention.
Our findings align with emerging evidence that routine social risk screening is feasible and improves connections to community resources. 6 Embedding the Hunger Vital Sign in electronic health records increases screening rates, 3 but challenges remain: limited resources, competing priorities and weak referral pathways. Potential approaches to mitigating these challenges include improving clinical workflow, adopting team-based models, and strengthening partnerships with community organizations. Implementation studies show that workflow redesign and collaboration with social workers, care coordinators, and community health workers can address these barriers. 6 From an implementation science perspective, patient receptivity provides a critical foundation for designing interventions that are feasible, acceptable, and sustainable within primary care workflows. Incorporating patient perspectives, as shown in our survey, supports developing patient-centered frameworks that balance feasibility for clinicians with acceptability to patients. 11
This study also has implications for family medicine education. Training physicians to recognize and address social determinants, including FI, is increasingly emphasized in competency frameworks. Patient support for physician involvement suggests curricular efforts to normalize these conversations will be well received. 11 These curricular efforts may include incorporating standardized patient encounters on FI screening and counseling and integrating education on community resources into a longitudinal curriculum for trainees. Addressing FI also aligns with family medicine’s mission of holistic, community-oriented care. 9
Limitations include the cross-sectional design and reliance on self-reported data, which may introduce recall and social desirability bias. Conducting the study in 2 clinics within 1 region limits generalizability. Self-selection bias is also of concern as subjects were aware of the subject matter prior to opting in to complete the survey and may have been more comfortable discussing FI compared to the broader clinic population. While our survey assessed comfort and expectations, qualitative methods could have offered deeper insights. Future studies should include more diverse populations and mixed methods to better capture patient perspectives on physicians’ roles in addressing FI.
Conclusion
FI remains a significant concern among family medicine patients, with clear associations to socioeconomic disadvantages and poor health status. Despite patient comfort and endorsement of physician involvement, screening and referral rates remain low. These findings suggest that opportunities exist to strengthen the role of family medicine practices in addressing FI by incorporating patient perspectives into screening protocols and care workflows. Efforts to expand training, integrate validated tools such as the Hunger Vital Sign into electronic medical records, and establish sustainable referral pathways may enhance the capacity of family physicians to address this critical social determinant of health.3,6 Ultimately, aligning patient expectations with clinical practice can help advance holistic, equitable care in family medicine. 10
All authors provided substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; All authors drafted the article or revised it critically for important intellectual content; All authors gave final approval of the version of the article to be published; and All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Footnotes
Author Contributions
All authors provided substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; All authors drafted the article or revised it critically for important intellectual content; All authors gave final approval of the version of the article to be published; and All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.