
Abstract
Background
Pain is the most common secondary condition in individuals with cerebral palsy (CP) 1 and the single most important factor associated with reduced health-related quality of life and participation.2-5 The most commonly reported pain sites are the lower extremities, the back, and the abdomen; however, pain in the upper extremities, headaches, and pain in the neck are also reported.6,7
Pain is a subjective experience and cannot be measured objectively. Self-reports can be prone to biases, such as social desirability bias and recollection bias, meaning that individuals might report what they believe the interviewer or provider wants to hear or that they simply do not recall their pain experience given the often shifting nature of pain. In the case of chronic pain (ie, pain lasting longer than 3 months), the individual might have grown accustomed to being in pain and does not reflect on it or assume that pain is normal. Nevertheless, self-reports are considered the gold standard, and the old tradition of having physicians report on their patients’ pain is no longer accepted. However, at times proxy reports are warranted. 8 In the context of CP, proxy-reports might be used at young biological or developmental ages, if the individuals have comorbid intellectual disabilities, or when the individuals are unable or not given the time to communicate. How accurately proxies identify pain is not well established, and both overestimations and underestimations have been reported.9-11 Although proxies oftentimes can identify that pain is present it might be more challenging to accurately report on how severe the pain is, or what the ramifications are of being in pain.10-12
Several studies have shown that the prevalence of pain increases with age and that pain is more often reported among females with CP. The proportions of reported pain vary depending on the inclusion criteria, the make-up of the study sample and how well it corresponds to the distribution of the total population, the time period considered, the study instrument used, and generally ranges between 50% and 75%.4,13-15
The Swedish Cerebral Palsy Follow-Up Program (CPUP) has been a multidisciplinary surveillance program for over 2 decades. The registry has a coverage rate of over 95%, and thereby includes almost all children with CP in Sweden. 16 Since 2011, adults with CP in Sweden are also followed in the program. The aims of CPUP are to prevent hip dislocations, contractures, and other secondary complications in individuals with CP.17,18 Pain information is reported regularly and since 2018 it is also recorded if the pain item is self or proxy reported.
In this study, we investigated the prevalence of pain reported by the children themselves or by proxies after adjusting for age, sex, communication ability, and gross motor function level.
Methods
Procedure and Measures
This was a cross-sectional registry study based on data from the CPUP. In CPUP, pediatric neurologists confirm or rule out the CP diagnosis according to the definitions set by the Surveillance of Cerebral Palsy Network in Europe, 19 generally by the age of 4 years. Gross motor function is classified with the Gross Motor Function Classification System (GMFCS) 20 and communication with the Communication Function Classification System (CFCS), 21 both with level I describing the highest level of function and level V the lowest.
The assessment schedules in CPUP for physical and occupational therapies are based on GMFCS level and age. Children at GMFCS-level I are examined annually up to 6 years of age and then every second year, whereas children at GMFCS-levels II to V are examined twice a year up to 6 years, then once a year. In addition to physical examinations, the therapists query, for instance, if the children are in pain. When possible, the children are supposed to report on their pain. If a child is unable to report, for some reason, the caregiver/s report on the child’s pain. The physical therapist report on who answered the pain item (self or proxy). In this study, CPUP data from the most recent visits of all children born between January 1, 2000 and December 31, 2016 who reported to the registry in 2017-2018 were included.
Age was calculated based on the date of visit and was recorded as a continuous variable in years. Sex was recorded as a dichotomous variable. The screening item on pain (“Does the child, or the parent, state that the child is in pain?”; yes or no) was either self- or, as needed, proxy-reported by the caregiver.
Statistical Analysis
Raw numbers and percentages were calculated for all categorical variables and means and standard deviations were calculated for continuous variables. Chi-square tests were used to compare differences between groups. Statistical significance was considered at 0.05% level.
A logistic regression was used to regress source of report on pain adjusted for age, sex, GMFCS level, and CFCS level. Because the effects of any one of the independent variables on the dependent variable (pain) might differ in a non-additive manner depending on the levels of the other independent variables, we were also interested in potential interaction effects. To avoid the difficult interpretation of “ratios of odds ratio” for the interaction terms, and to get a clear understanding of the effect for each group, we used predictive margins and average marginal effects to present the results. Predictive margin of a covariate level/value is the probability of the outcome given everyone in the study would have this level/value for the covariate with all other covariates remaining the same, that is, they are not set at their mean values but represent the actual study sample distribution. Average marginal effects were tested for sex, age, GMFCS, and CFCS with source of report. These effects can be thought of as the average effect of changes in independent variables on the change in the probability of outcomes (ie, the average change in probability when X increases by 1 unit) in nonlinear models, and is presented as a number between −1 and 1. Given that our model included interactions of source of report with all other covariates, the marginal effects can differ for each level of CFCS, GMFCS, age, and sex depending on the source of report and express change in the outcome more accurately. We used 95% confidence intervals (CI) to assess statistical significance. 22
The analyses were performed using Stata (IC v.15.1 StataCorp LP).
Results
In total, 3783 children (2202 males, 1581 females), 1 to 18 years of age, reported in 2017-2018 and were included in the study. The characteristics of the study sample are presented in Table 1.
Characteristics of the Study Sample by Source of Report.
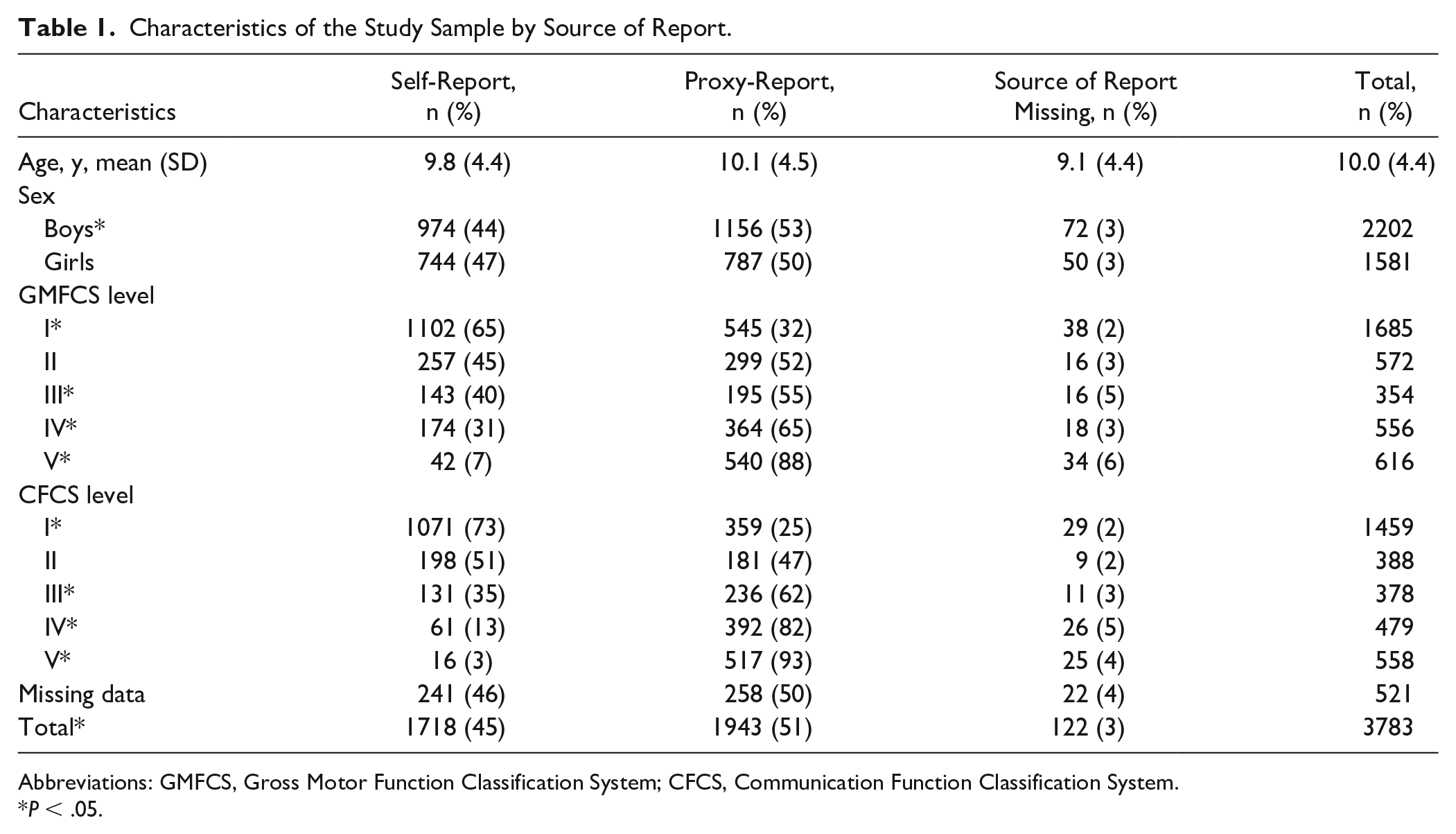
Abbreviations: GMFCS, Gross Motor Function Classification System; CFCS, Communication Function Classification System.
P < .05.
The pain item was self-reported in 1718 reports (45.4%), by proxy in 1943 (51.4%), and information on who report-ed was missing in 122 reports (3.2%). The proportion of self-reports increased steeply with age up to 10 years, followed by a minor increase up to 17 years of age, at which age 68% self-reported on pain (Figure 1). The proportion of children who self-reported decreased by GMFCS level from 65% at GMFCS I to 7% at level V, and by CFCS level from 73% at CFCS I to 3% at level V (Table 1).

Proportion of children self-reporting pain related to age. Six children 1 year of age and 144 children 18 years of age were not included in the figure.
Overall pain was reported as present in 1537 of 3624 children (42.4%). Information on pain was missing in 159 reports (4.2%) (Table 2). Of those who self-reported, 43.8% reported pain compared with 40.3% of those where pain was proxy reported (P = .04). Pain was reported more often in girls (45.7%) than boys (40.0%) (P < .001). Reports of pain increased with age from 23% in 2- to 3-year-olds to about 50% in those 11 to 18 years old. At each GMFCS level and at each CFCS level, children who self-reported were more likely to report pain than were proxies (Table 2).
Prevalence of Pain in Children with Cerebral Palsy Related to Sex, GMFCS Level, and CFCS Level, by Source of Report.

Abbreviations: GMFCS Gross Motor Function Classification System; CFCS Communication Function Classification System.
A total of 159 reports with missing information excluded.
Results from the logistic regression showed that the probability of reporting pain in children who self-reported was 42.5%, which was slightly lower than for children where pain was proxy-reported (43.5%); however, the difference was not statistically significant. There were no statistically significant differences in reporting pain between self- and proxy-reported cases based on sex. Proxies reported pain significantly more often in children at GMFCS level IV and at CFCS level I, and less often in children at CFCS level III. At all other GMFCS and CFCS levels, there were no statistically significant differences in reported pain between self and proxy reports (Table 3). Table 4 and Figure 2 present predictive margins of reporting being in pain for each covariate. Overall, boys had a slightly lower probability of pain (39.9%, CI 37.7-42.1) compared with girls (44.6%, CI 42.0-47.3), which is a statistically significant difference (4.7%, CI 1.3-8.2). Furthermore, the probability of pain increased gradually with age (on average by 1.8% per year, CI 1.3-2.2) from 27% at age 1 year to 57% probability of pain at age 18 years. There was also a significantly higher probability of pain for GMFCS level V (58%, CI 49.8-66.4) compared with GMFCS levels I to IV, where probability of pain varied between 36% and 41%. Children at CFCS levels IV/V had a lower probability of pain (37.7%) than children at CFCS level I (47.8%). The differences are summarized in Supplementary Table 1. Results calculated as odds ratios are presented in Supplementary Table 2.
Average Marginal Effects of Being in Pain for Proxy- Versus Self-Report.
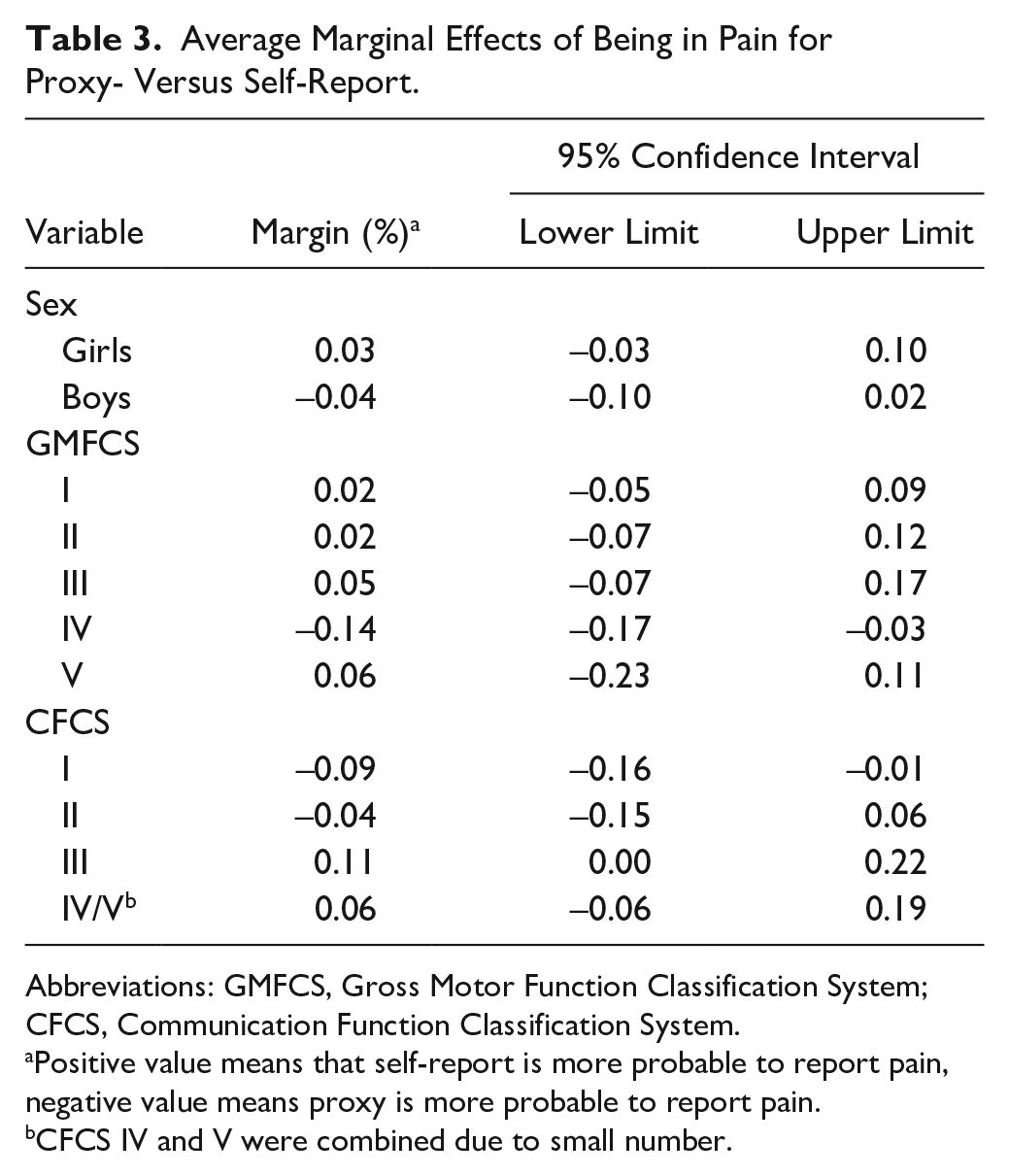
Abbreviations: GMFCS, Gross Motor Function Classification System; CFCS, Communication Function Classification System.
Positive value means that self-report is more probable to report pain, negative value means proxy is more probable to report pain.
CFCS IV and V were combined due to small number.
Predictive Margins of Reporting Pain for Each Covariate.
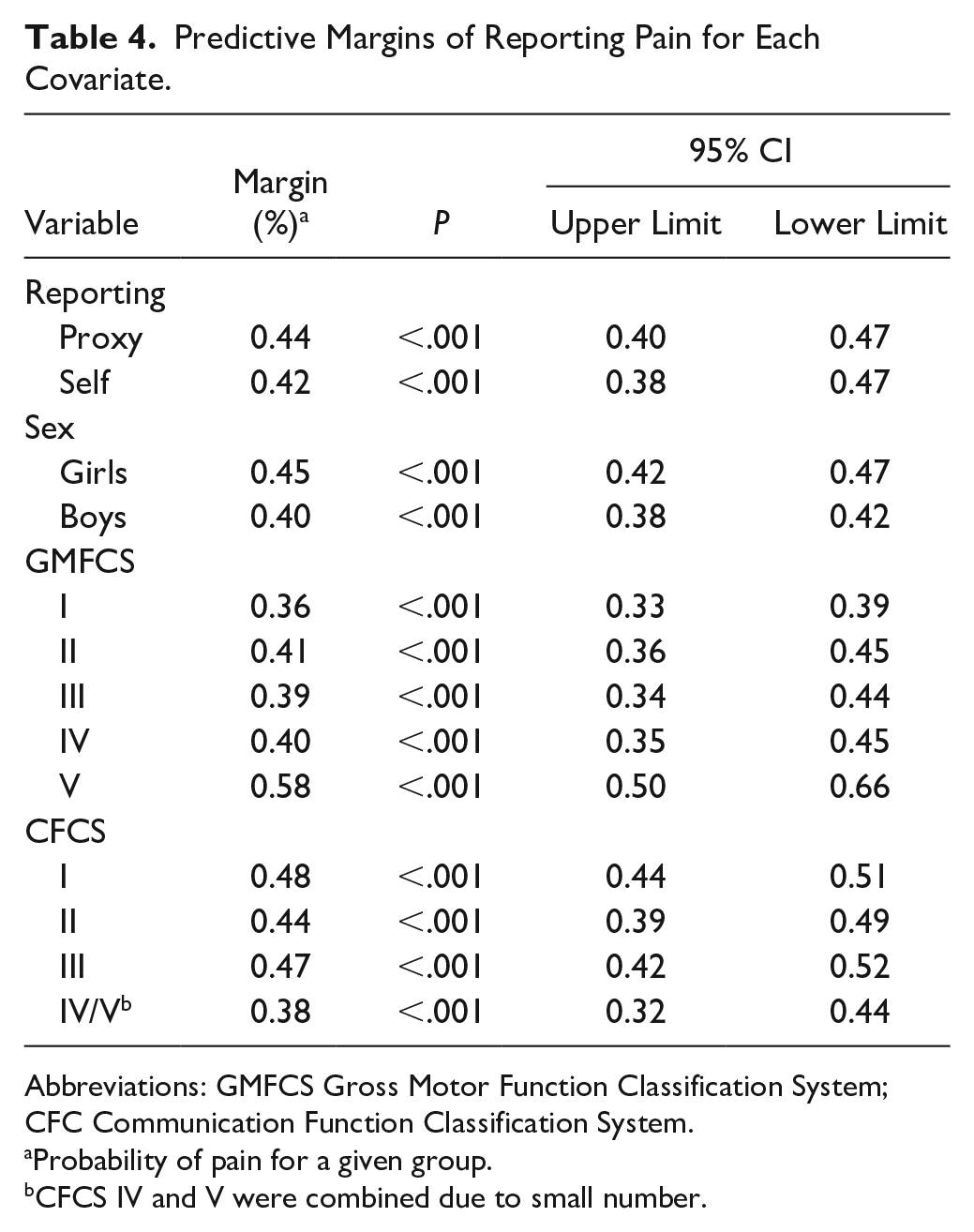
Abbreviations: GMFCS Gross Motor Function Classification System; CFC Communication Function Classification System.
Probability of pain for a given group.
CFCS IV and V were combined due to small number.
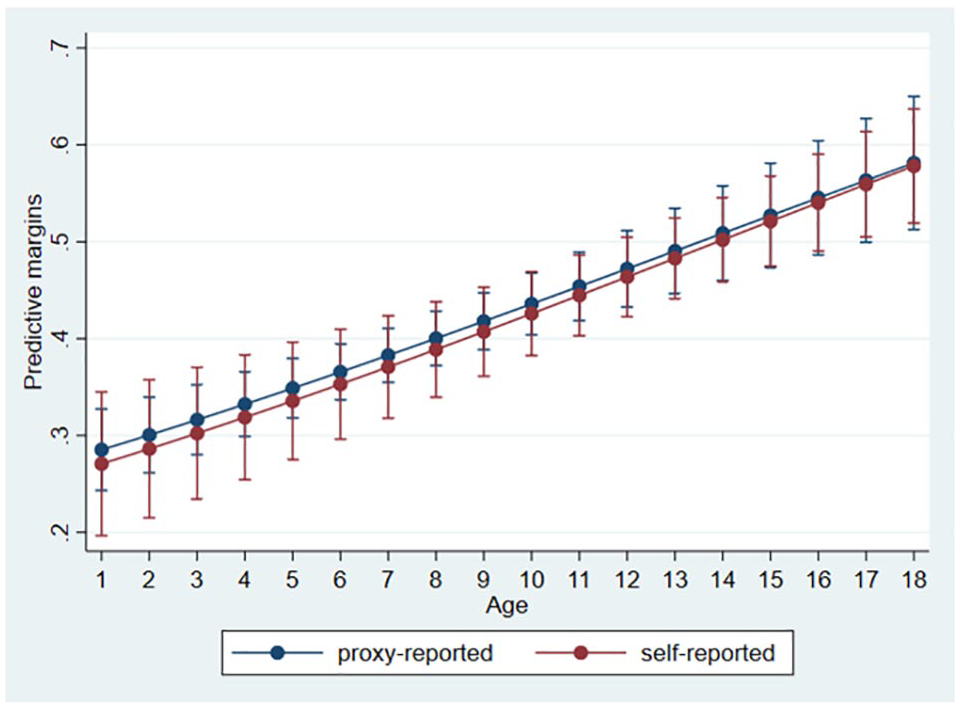
Predictive margins of reporting being in pain for proxy- versus self-reporting children related to age.
Discussion
Pain was more commonly reported in children who self-reported (43.8%) than in children where pain was proxy-reported (40.3%) both for the total number of children and for all GMFCS and CFCS levels separately. However, in the regression analysis, where adjustments were made for age, sex, GMFCS level, and CFCS level, the difference in pain between self- and proxy reporting was not statistically significant.
The overall prevalence of pain (41%) was higher than in a previous study from Sweden 6 (32%), probably explained by the 3-year higher mean age in the present cohort. The reported pain prevalence is still lower than the 50% to 75% reported in other studies on pain and CP4,13-15; however, this may also partly be due to different age ranges, inclusion criteria, and definitions of pain used in the different studies. The higher pain prevalence among girls and older children is in line with earlier studies.12,13 The lower prevalence of pain reported in children at CFCS levels IV and V is mostly driven by reduced pain reported by proxy and we see no clinical reasons as to why children with poorer communication abilities should experience less pain.
The pain item was answered by proxies in 51% of all children. Proxy reports were more common in younger children and in children at higher GMFCS and CFCS levels. However, there were many children at CFCS levels I and II who, despite their good communication abilities, had pain reported by proxies. Some of these children might have had intellectual disability and therefore were considered unable to self-report, or possibly that their young age prevented them from self-reporting. In addition, 65% of the children at GMFCS I self-reported. Although there is not a perfect positive correlation between intellectual disability and GMFCS level, it seems unlikely that 35% of those at GMFCS level I would not be able to self-report. It seems feasible to assume that more children should have been able to self-report and children and adolescents should be encouraged to do so whenever possible, even if it takes more time in the clinical setting.
Previous studies comparing self and proxy reports of pain have shown various results. Penner et al, 9 in a cross-sectional study of 252 children with CP, 3 to 19 years old, found a good agreement between the children’s self-reports and parental reports. Physicians, however, under-reported pain, reporting pain in 39% of the children, compared with 55% in the children’s self-report. Hadden et al, 10 in a study of 63 children with CP, 5 to 18 years old, found that the caregivers tended to report lower pain intensity scores than both the children themselves and their physical therapists.
There were several limitations to our study. The reason for proxy reporting could not be obtained for the individual child, as this is not included in the report form. It would have been interesting to study how reports of pain intensity vary between self and proxy reports; however, pain intensity was not included in the data used in this study. Pain is subjective and self-report is the gold standard and as such the pain that an individual reports is “the truth.” It would have been informative to compare self and proxy report on pain for the same individual to assess the agreement. That was not possible in this study as either the individuals themselves or the caregivers reported on pain but not both. Still, there is the issue of communication. When children at GMFCS levels IV and V are able to communicate to their parents that they are in pain the parents can relay that information. When the children are not able to report on their pain such a comparison cannot be made. Furthermore, it is only possible to adjust analyses on factors that are measured. The children included in the proxy-reported group were, as expected, younger and had more severe CP in terms of GMFCS and CFCS levels. It is possible that the two groups were different in other ways too that were not measured in CPUP or were not included in the current study and therefore not adjusted for. Thus, we do not know how similar the self and proxy groups in the study were on other factors related to pain.
The strength of this study is that we analyzed the total population of children with CP minimizing the risk of selection bias and that it was possible to adjust the results for some of the factors that might have affected the results; age, sex, GMFCS level, and CFCS level.
In summary, this population-based study of children aged 1 to 18 years with CP showed that pain was reported by proxy in 50% and that pain was reported more frequently by those who self-reported, especially girls. However, after adjusting for age, sex, GMFCS level, and CFCS level, the differences in the proportion reported that they have pain were not statistically significant between self and proxy. Assuming that the self- and proxy-reported groups were not significantly different on relevant variables not controlled for the results indicate that presence of pain is equally reported by children and parents.
Supplemental Material
Supplementary_Table_1 – Supplemental material for Self-versus Proxy-Reported Pain in Children with Cerebral Palsy: A Population-Based Registry Study of 3783 Children
Supplemental material, Supplementary_Table_1 for Self-versus Proxy-Reported Pain in Children with Cerebral Palsy: A Population-Based Registry Study of 3783 Children by Gunnar Hägglund, Amanda Burman-Rimstedt, Tomasz Czuba and Ann I. Alriksson-Schmidt in Journal of Primary Care & Community Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Nordforsk grant number 82866, Forte and the Swedish Research Council grant number 218-01468, Linnea and Josef Carlsson Foundation, Norrbacka Eugenia-stiftelsen, Jerringfonden, and Stiftelsen för bistånd åt rörelsehindrade i Skåne. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the funders.
Ethical Approval
The study was approved by the Ethics Board at Lund University (LU-433-99).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.