
Abstract
Objective
Assessing pain in individuals with neurological conditions like cerebral palsy is challenging due to limited self-reporting and expression abilities. Current methods lack sensitivity and specificity, underlining the need for a reliable evaluation protocol. An automated facial recognition system could revolutionize pain assessment for such patients.
The research focuses on two primary goals: developing a dataset of facial pain expressions for individuals with cerebral palsy and creating a deep learning-based automated system for pain assessment tailored to this group.
Methods
The study trained ten neural networks using three pain image databases and a newly curated CP-PAIN Dataset of 109 images from cerebral palsy patients, classified by experts using the Facial Action Coding System.
Results
The InceptionV3 model demonstrated promising results, achieving 62.67% accuracy and a 61.12% F1 score on the CP-PAIN dataset. Explainable AI techniques confirmed the consistency of crucial features for pain identification across models.
Conclusion
The study underscores the potential of deep learning in developing reliable pain detection systems using facial recognition for individuals with communication impairments due to neurological conditions. A more extensive and diverse dataset could further enhance the models’ sensitivity to subtle pain expressions in cerebral palsy patients and possibly extend to other complex neurological disorders. This research marks a significant step toward more empathetic and accurate pain management for vulnerable populations.
Keywords
Highlights
We construct a pioneering dataset of facial images illustrating pain in cerebral palsy.
Our automated facial recognition system can enhance pain assessment in cerebral palsy.
This novel system may be extrapolated to other complex neurological conditions.
Introduction
Pain assessment is exceedingly challenging in individuals who, in addition to lacking self-report capabilities, present complex neurological conditions that impact both facial and bodily expressions. Cerebral palsy (CP) stands as a group of enduring neurological disorders impacting motor function, ranking among the most prevalent lifetime medical conditions.1,2 Its prevalence, estimated at 2–3 per 1000 live births in developed countries, 3 highlights its significant impact. Due to disruptions in brain development, individuals with CP often manifest a range of non-motor comorbidities, notably pain (74%–82%), intellectual disability (50%), speech impairment (25%), epilepsy (25%), urinary/fecal incontinence (25%), and behavioral or sleep disorders (20% to 25%).4,5
This chronic condition, spanning from birth throughout one's lifespan, requires ongoing therapy services. 6 This demand places substantial financial burdens on families and healthcare systems and leads to extended inpatient stays.7,8 Given its chronic nature, cognitive and speech-related comorbidities, and the unique motor impairments that can affect non-verbal communication, CP serves as a valuable model for investigating complex chronic pathologies.
Pain, with its exceedingly high prevalence, emerges as one of the main limitations to carrying out activities of daily living for individuals with CP. 9 The complexity of accurately diagnosing pain in those with cognitive or communication impairments 10 has led to a historical pattern of underestimation and inadequate treatment of pain in these individuals.11–14 It is posited that the self-reports from individuals with CP regarding their pain should be considered paramount in identifying the presence, intensity, and the overall effect this pain has on their daily lives. 15 Consequently, initiating the pain assessment process with efforts to obtain either verbal or non-verbal self-reports of pain—utilizing alternative and augmentative communication systems, deliberate hand gestures, or nodding, for example—is recommended, even for those with cognitive impairments. 16 Given that, as mentioned previously, an estimated 50% of individuals with CP are affected by intellectual disabilities, 4 which may hinder self-reporting abilities, coupled with evidence indicating that the majority of adults with CP experience various communication disorders, 10 the challenge of pain assessment becomes markedly pronounced. This difficulty in pain identification poses a substantial challenge not only for clinical and socio-health institutions tasked with caring for these individuals but also for their families, who frequently describe pain identification as a particularly daunting task.17–20 Both stakeholders underscore the critical need for the development and implementation of reliable and accurate methods for evaluating pain in those unable to self-communicate their pain experiences. 21 However, the scientific community has yet to establish a standard for pain assessment in this demographic, 22 pointing out an area that urgently needs attention and improvement.
Recent years have seen various approaches to address pain assessment in non-communicative populations. These range from methods based on physiological signs to proxy observation of painful behaviors. Research has explored the utility of specific pain biomarkers such as salivary metabolites,23,24 brain activity,25,26 cardiorespiratory vital signs, skin conductance, muscle tension, or heart rate variability27–29 for identifying the presence of acute or chronic pain.
Observational behavioral scales are the most used tools to assess pain in this population. 30 However, their use is not without controversy, as they can yield subjective, observer-dependent data,31–33 and some may lack specificity or sensitivity. 34 Observers might also confuse other emotions, such as fear or stress, for pain. 31 Further, studies comparing pain assessments in children with CP by their parents have uncovered both overestimations and underestimations of pain by parents.35,36 This disparity in pain assessment extends to healthcare professionals as well. 37
In this context, the Facial Action Coding System (FACS), 38 initially designed to reduce subjectivity and provide objective descriptions of facial expressions for basic emotions, can be employed to categorize pain more objectively. 39 However, mastering this system requires significant effort, and its microanalytic methods can be challenging to apply in routine clinical pain evaluations. 40
In order to automate the facial expression recognition, systems using deep learning (DL) approaches have led to significant advancements, particularly in the context of emotions. DL has already shown successful results in other tasks related to the identification of patterns in image-related tasks such as segmentation in medical imaging. Traditionally, human experts in the field rely on their knowledge and prior experience to perform these tasks. However, the advent of deep learning has revolutionized this process by enabling automatic pattern learning. 41 Consequently, numerous studies have leveraged deep learning techniques across various tasks in medical imaging. For instance, deep learning has been applied to segmentation tasks in brain images,42,43 image registration, 44 and image fusion for Alzheimer's Disease/Mild Cognitive Impairment (AD/MCI) diagnosis. 45 Additionally, it has been utilized for image annotation in chest X-rays, 46 diagnosis of brain disorders, 47 segmentation of brain tumors, 48 and analysis of microscopic images. 49 These applications highlight the versatility and effectiveness of deep learning in addressing various challenges in medical image analysis, paving the way for improved diagnosis and treatment in healthcare.
In order to automate the facial expression recognition, systems using deep learning (DL) approaches have led to significant advancements, particularly in the context of emotions, and they rely on audiovisual databases containing emotional expressions. 50 Nowadays, we find multiple datasets housing collections of facial expressions depicting pain, both as standalone expressions and within broader emotional expression datasets.51,52 These datasets encompass images or videos capturing spontaneous pain, such as shoulder, neck, or lumbar pain, as well as pain induced by thermal or electrical stimuli. Some even include neonates or preschool-age children receiving injections. Within these repositories, one can find images portraying at least two levels of pain intensity, and they predominantly involve healthy individuals. 52 These datasets have paved the way for the application of artificial intelligence methods, resulting in impressive achievements in pain detection, even distinguishing between spontaneous and simulated facial pain expressions. 53
Automated systems grounded in the FACS, including FaceReader, 54 OpenFace, 55 AFAR toolbox, 56 or PainCheck®, 57 have been developed for pain assessment in diverse non-communicative populations, including infants, 58 and individuals with advanced dementia. 59 However, these solutions may lack the specificity required to assess pain in complex neurological pathologies, such as individuals with CP, who may exhibit motor dysfunctions affecting facial expressions of pain.
Further, to understand the decision-making processes of the AI system and explore the idiosyncrasies on how it operates with individuals with CP, eXplainable Artificial Intelligence (XAI) methods can be applied. 60 XAI techniques provide comprehensive explanations elucidating the decision-making processes and output generation of DL models. This facilitates the comprehension and interpretation of results by human users, enhances model trustworthiness, discerns causality among data variables, or informs decision taking.60,61 In the case of facial expression recognition, we find works applying XAI techniques to emotion recognition such as sadness or happiness62,63 or the work by Weitz et al. (2019), 64 whose research focused on the differences among facial expressions like anger or happiness, and pain.
The aim of this work is to improve pain assessment accuracy in individuals with complex neurological conditions, potentially revolutionizing the way we address their pain-related needs. In this research, our emphasis centers on deep neural networks trained using pain expression images. This focus stems from the inherent capability of these networks to adeptly handle the intricate challenges associated with recognition in real-world, or “in the wild”, scenarios, as evidenced by Li and Deng (2020). 65 Our study is confined to the analysis of static images, as opposed to dynamic sequences or video data. The current study sets out to pioneer an automated facial recognition system, grounded in DL, to evaluate pain in individuals with complex neurological pathologies, specifically adults with CP. The proposed DL system will undergo training using a variety of existing pain datasets that capture diverse pain conditions. Additionally, a built purpose-designed dataset tailored for individuals with CP, denoted as CP-PAIN, will be used to evaluate the system's effectiveness.
Subsequently, the automated system's pain scores will be compared with evaluations by clinicians employing three commonly used observational scales within the CP population: The Wong Baker FACES® Pain Rating Scale, 66 the Facial Action Coding System (FACS), and The Non-Communicating Adults Pain Checklist (NCAPC). 67
Finally, to delve deeper into the mechanisms underlying DL techniques, we include eXplainable Artificial Intelligence (XAI) techniques to understand the rationale behind the outcomes of the pain perception mechanisms employed by DL models and explore potential commonalities among diverse trained DL models, especially when used with people with CP.
The work is organized as follows. Section 2 describes the methods used to build the dataset of pain expressions in individuals with CP and the automated pain recognition system. Section 3 describes the results achieved and the last Section discusses the main findings and concludes the work.
Methods
Within this section, we describe the methodology encompassing the construction, labelling, and evaluation of a dataset of pain expressions in individuals with CP (CP-PAIN), as well as the training phases of the pain recognition artificial intelligence (AI) system.
Constructing and assessing the CP-PAIN database
Prior to the construction of the CP-PAIN database, we adhered to a robust ethical framework. Written informed consent, encompassing the use of images for informative purposes, was obtained. This process involved participants with CP who had the legal capacity to provide consent (n = 10), as well as legal representatives of remaining participants (n = 43). The documentation was thoughtfully written in standard form and an accessible easy-to-read format to ensure its comprehension by as many participants as possible.
Ethical compliance and approvals
This research meticulously adhered to the principles outlined in the Declaration of Helsinki (1991). The research protocol received approval from both the ASPACE Foundation's ethics committee and the Research Ethics Commission of the Balearic Islands (protocol number IB4046/19), affirming its ethical rigor.
Participants
The study extended invitations to all users diagnosed with CP, or their legal representatives, affiliated with the Adult Life Promotion Services of the Cerebral Palsy Association (ASPACE) in the Balearic Islands (Majorca, Spain) and Toledo (Castilla-La Mancha, Spain). Participants were exclusively selected based on two criteria: a diagnosis of CP and being over 18 years old. The only exclusion criterion was the lack of consent for the use of personal images by the institutions involved. A total of 53 individuals (mean age = 37.57 (9.88) years, age range = 21–69 years, including 19 females) agreed to participate. Subsequently, they or their respective legal representatives formally filled in the informed consent.
Table 1 displays the clinical characteristics of the 53 participants with CP.
Clinical characteristics of participants.

Measures
In addition to gathering sociodemographic and clinical data (e.g., age, sex, type of CP, level of motor, and communication impairment) from medical records, the study implemented the following measures:
Observational scales
1. The Facial Action Coding System (FACS): Designed to minimize subjective judgments in assessing facial activity, FACS is a widely employed system for coding emotional facial expressions in scientific studies. 70 It has been successfully applied to individuals with communication disorders and CP, 71 and a recent systematic review and meta-analysis concluded that it is the preferred scale for individuals with CP who have communication impairments. 30
FACS dissects facial expressions into 44 individual components of muscle movement, known as Action Units (AUs), rating them on a 6-point scale (0 = no expression, 5 = extreme expression). Pain is identified through six specific AUs: lowering of the eyebrows (AU4), elevation of the cheeks and compression of the eyelids and/or contraction of the cheekbones (AU6/AU7), wrinkling of the nose and/or raising the upper lip (AU9/AU10), and closing the eyes (AU43).40,72
The total pain score is calculated as follows: Pain score = AU4 + (AU6AU7) + (AU9AU10) + AU43, yielding a 20-point scale.
2. The Non-Communicating Adults Pain Checklist (NCAPC): This 18-item scale assesses pain behaviors through six components: vocal response, emotional response, facial expression, body language, protective responses, and physiological responses. Derived from the Non-Communicating Children Pain Checklist (NCCPC), the NCAPC offers optimal utility irrespective of the evaluator's familiarity with the individual. 73 The NCAPC has demonstrated strong psychometric properties and the capacity to identify pain and its intensity in adults with intellectual and developmental disabilities. 67 Evidence points to this scale, along with FACS, as the optimal ones for assessing pain in adults with CP. 74
3. The Wong Baker FACES® Pain Rating Scale: This scale rates pain on a scale from 0 (no pain) to 10 (worst possible pain) by comparing the patient's facial expression to the provided scale images. While commonly used in pediatric populations, it has also found utility applied to individuals with disabilities and communication disorders. 75
As depicted, these scales, especially FACS and NCAPC, were selected over others due to their specific relevance, applicability, and proven ability to address the unique challenges of assessing pain in adults with CP, particularly those facing communication barriers. The selection of the Wong Baker FACES® Pain Rating Scale was primarily driven by its ease of use and the consideration that it is a tool for individuals with CP and cognitive impairment could utilize to rate their level of pain. This combination of scales allows for a comprehensive and nuanced approach to pain evaluation in this specific population, leveraging the strengths of each tool and addressing the particular needs of our study cohort.
Procedure for data collection
Video recordings capturing facial and body expressions were conducted in situations where participants with CP either underwent potential painful procedures or when caregivers identified signs of pain in other care procedures (e. g. feeding, personal hygiene, assistive…). For scheduled painful procedures such as therapies or intramuscular injections, the video recording initiated 2 min prior to the potentially painful stimuli and continued for 2 min thereafter. In cases where participants had the cognitive capacity (n = 24, resulting in a total of 43 recorded expressions), they were kindly asked to self-rate their pain on a scale of 1 to 10 using the Wong-Baker Faces pain rating scale.
Efforts to reduce potential biases in the video recordings were meticulously implemented. Standardized protocols, with instructions for camera placement, lighting, and the duration of the recordings were stablished to minimize variation in recording conditions. Moreover, observers involved in the video recording underwent training including pain recognition, and the recording equipment and protocol, in order to homogenize the observers’ understanding and approach. In addition, observers were blinded (when possible) to the participants’ medical histories to avoid preconceived notions influencing the recording process. Finally, video recordings were independently review by evaluators who were not involved in the recording sessions.
Throughout the study duration, a comprehensive total of 127 recordings were successfully acquired. These recordings depicted various sources of pain in the painful images, which were classified as follows:
- Intramuscular injection: 77 images (60.6%) - Muscular stretching: 32 images (25.2%) - Other sources of pain: 18 images (14.2%)
Expert evaluation of video recordings
All video recordings underwent meticulous offline evaluation by two highly experienced physiotherapists, with more than 10 years of expertise in treating individuals with CP. These evaluators independently applied the three observation scales: the Wong-Baker Faces pain rating scale, NCAPC, and FACS.
In this study, efforts to reduce potential biases in the physiotherapists’ evaluations were meticulously implemented. Recognizing the inherent subjective biases in traditional observational scales, thorough training was provided to the two clinicians involved to standardize their application of these scales, aiming for a consensus in their evaluations to minimize individual subjective interpretations. Furthermore, by using three different observational scales we aim to provide a comprehensive view of pain assessment and to mitigate the limitations inherent in any single scale. Additionally, to further prevent bias, the design of the study ensured that evaluators using traditional scales were blinded to each other's results, promoting independent evaluations free from preconceived expectations about the pain scores. Rigorous statistical analysis, specifically using the Intraclass Correlation Coefficient (ICC) model 2,k, was conducted to assess inter-rater reliability among the clinicians (MSP, MSR, MSE k, and n used in the equation to refer, respectively, Mean Square Persons, Mean Square Raters, Mean Square Error [from a two-way ANOVA], and number of persons).
76

The interpretation of the ICC scores followed the categories proposed by Fleiss (1986): 77 low agreement (ICC < 0.40), fair/good agreement (ICC 0.41 to 0.75), and excellent agreement (ICC > 0.75).
For a precise comparison with the AI system's assessments, we rigorously applied a mathematical process to reclassify the mean scores from each observational scale into binary outcomes. Specifically, a “0” score was designated to signify “no pain”, whereas any score above 0 denoted the detection of pain. Consequently, an image was categorized as “no pain” only if there was a unanimous ‘0’ score consensus among all evaluators. For any deviation from this consensus, the image was systematically labelled as “pain”. This systematic categorization facilitated a clear and unbiased distinction between pain and no pain expressions based on quantifiable measures.
Challenges with self-reports
Despite our initial efforts to collect retrospective self-reports from participants following the video recordings, we encountered notable challenges, primarily due to cognitive and attentional issues experienced by the participants. Consequently, only a limited number of self-reports, totaling 10, could be successfully gathered. The challenge of obtaining only 10 self-reports, however, significantly impacted our methodology, compelling us to abandon the initially proposed comparative approach. This adjustment underscores the broader difficulties inherent in pain assessment for individuals with CP, and reflects the critical need to adapt research methodologies to effectively address these complexities.
Deep learning pain recognition
Datasets
Aiming at building a pain recognition system applicable to images of individuals with CP, we merge three extensively used databases: the UNBC-McMaster Shoulder Pain Expression Archive Database, 78 the Multimodal Intensity Pain dataset (MInt PAIN), 79 and the Delaware Pain Database. 51 For the sake of brevity, we will subsequently denote this merged dataset as PAIN-DB.
The UNBC-McMaster Shoulder Pain Expression Archive Database comprises 25 adult patients afflicted with shoulder pain. It features a collection of 200 distinct range of motion tests, encompassing both affected and unaffected limbs. Data acquisition involves videos capturing facial expressions, albeit in low resolution, which also include social interaction and verbal communication. Annotations include self-report measurements via Visual Analog Scales (VAS) encompassing sensory and affective aspects, along with pain intensity assessed by both self-report and observer (Observer-Assessed Pain Intensity, OPI). Moreover, annotations encompass limb information (affected/unaffected) and FACS coding.
The MInt PAIN Database presents a collection of images obtained through electrical muscle pain stimulation, involving 20 subjects. Each subject participated in two trials during data acquisition, with each trial encompassing 40 pain stimulation sweeps. Within these sweeps, two types of data were captured: one representing the absence of pain, and the other portraying pain at four varying intensities.
The Delaware Pain Database is an extensive compilation of fully characterized photographs featuring 127 female and 113 male subjects, with an emphasis on painful and neutral expressions. The dataset's primary hallmark lies in its remarkable diversity across dimensions of race, gender, and expression intensity.
Upon the integration of the three datasets, a relabeling into two classes was performed: images featuring pain and images devoid of pain. Consequently, images encompassing varying degrees of pain were grouped within the first class, while the remaining images were categorized under the second class. This reduction served two primary objectives: foremost, the normalization of data across the datasets, aligned with the two-class structure in the Delaware Pain Database; and secondly, the transformation of the task into a binary classification problem.
Furthermore, we did not use all available frames from UNBC-McMaster and MInt PAIN to avoid overfitting on the users they contain. Since there is little variation in consecutive frames, instead of using them all, a sample of twenty frames per user and class was taken. The final PAIN-DB dataset, composed by images from the three described databases, is summarized in Table 2. Figure 1 depicts some example images from each database.
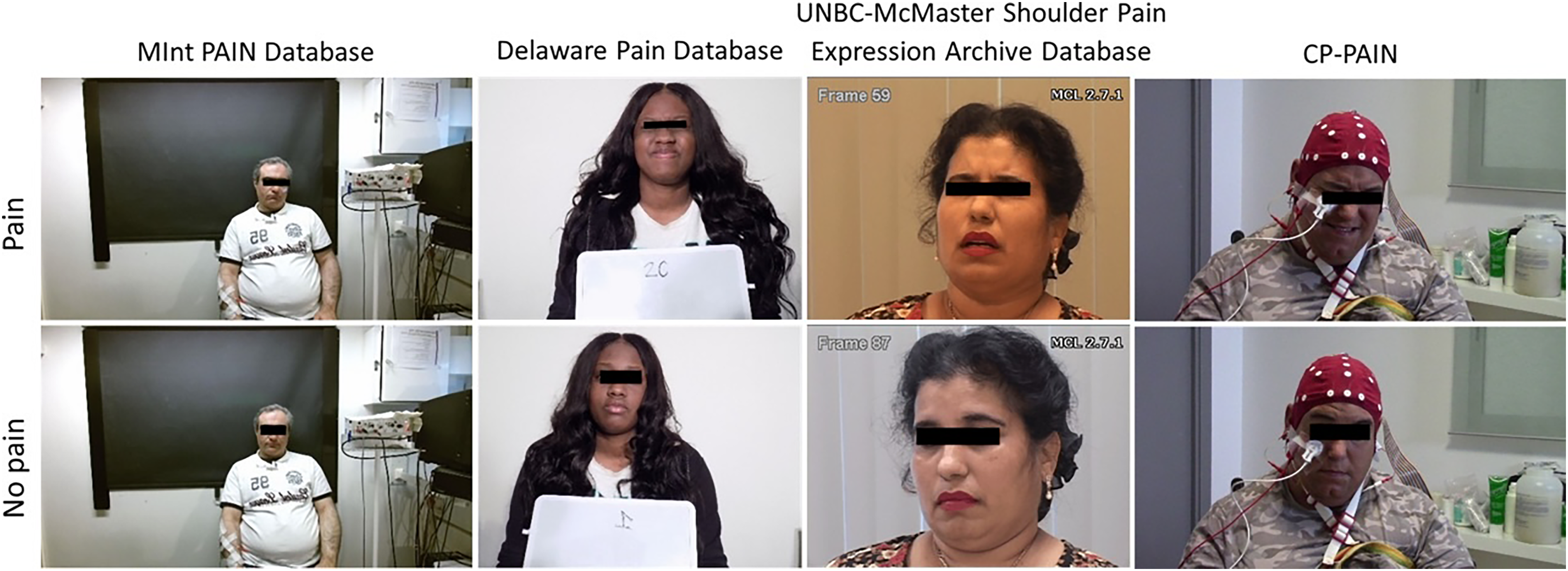
Example of images with and without pain, from the four datasets employed in this study.
Breakdown of PAIN-DB dataset into the datasets forming it.
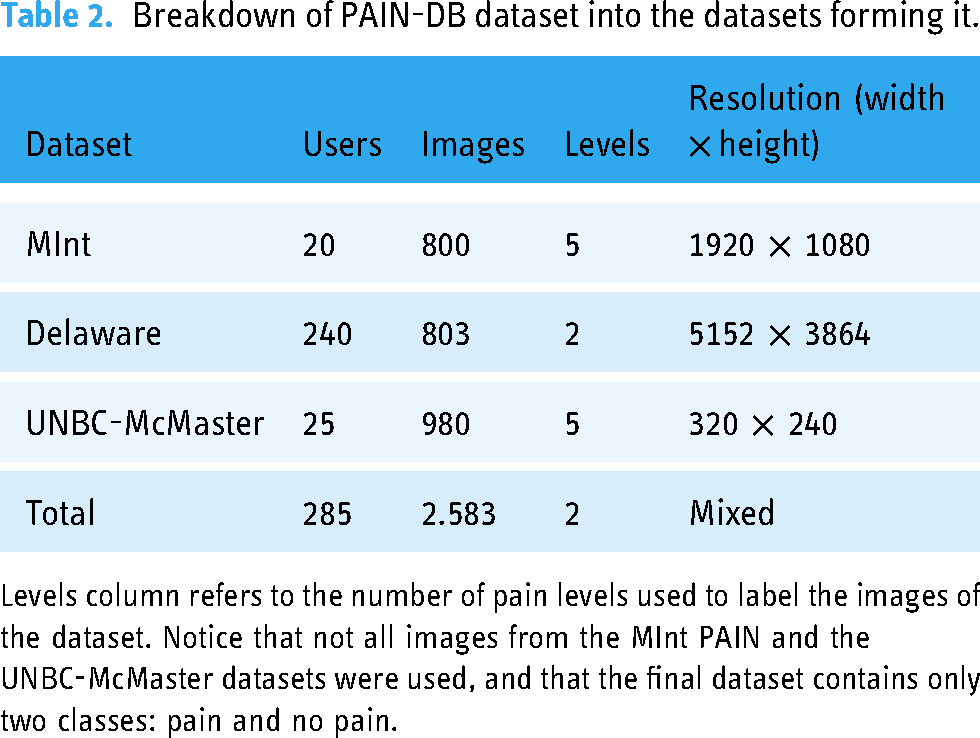
Levels column refers to the number of pain levels used to label the images of the dataset. Notice that not all images from the MInt PAIN and the UNBC-McMaster datasets were used, and that the final dataset contains only two classes: pain and no pain.
To assess the efficacy of the PAIN-DB-trained pain recognition system on individuals with CP, a testing dataset was curated from video recordings of study participants with CP, designated as CP-PAIN. By using pin-pointed moments of pain expression as determined by one physiotherapist specialized in neurological rehabilitation, two frames were extracted from each video: one capturing the moment of pain manifestation and another from a non-pain moment, thus ensuring a balanced dataset composition. Regrettably, a subset of videos proved unsuitable for inclusion due to two primary reasons: substantial occlusions obscuring facial features during pain instances, and participants wearing surgical masks that obscured half of the face. Although human observers can bypass these occlusions to discern pain expressions, our automated system lacked training for such scenarios, which could introduce unpredictable outcomes. Consequently, these videos were omitted. The resulting CP-PAIN dataset comprised 109 images, representing a dataset suitable for evaluation. Two example images from this dataset can be found on Figure 1, in the rightmost column.
Image preprocessing
We conducted a pre-processing phase to enhance the performance of the neural networks, which comprised cropping and background subtraction.
Images were cropped into a squared region containing the face (similar to Haque et al. (2018) approach 79 ). This was achieved through the application of the well-established multitask cascaded convolutional networks for face detection. 80
Furthermore, the background subtraction was accomplished through the integration of U2-Net, 81 which facilitates precise object segmentation. In our case, we used their pretrained weights that had been fine-tuned for human segmentation. Following the extraction of a binary mask outlining the background pixels, these regions were replaced with white color, thereby retaining only the human subject within the image frame.
The combined cropping and background subtraction procedures were devised to streamline the pain recognition task for the neural networks. This dual process serves both to eliminate any interference introduced by factors other than the person's facial features and to standardize the images. This standardization ensures that the facial attributes consistently occupy an approximate spatial alignment. Finally, the resultant images were resized to the input dimensions required by the distinct network architectures utilized in our study. Examples of the preprocessed images for each class and dataset are shown in Figure 2.

Resulting images after the pre-processing performed before any training or testing on the four databases, featuring a face crop and background subtraction.
Models
We built ten neural networks aiming at recognizing pain from images (see Table 3). For the sake of simplicity, we denoted the models introduced in Song et al. (2014), 82 Li et al. (2015), 83 and Ramis et al. (2022), 63 as SongNet, WeiNet, and SilNet, respectively.
List of network architectures used in this study for pain recognition.
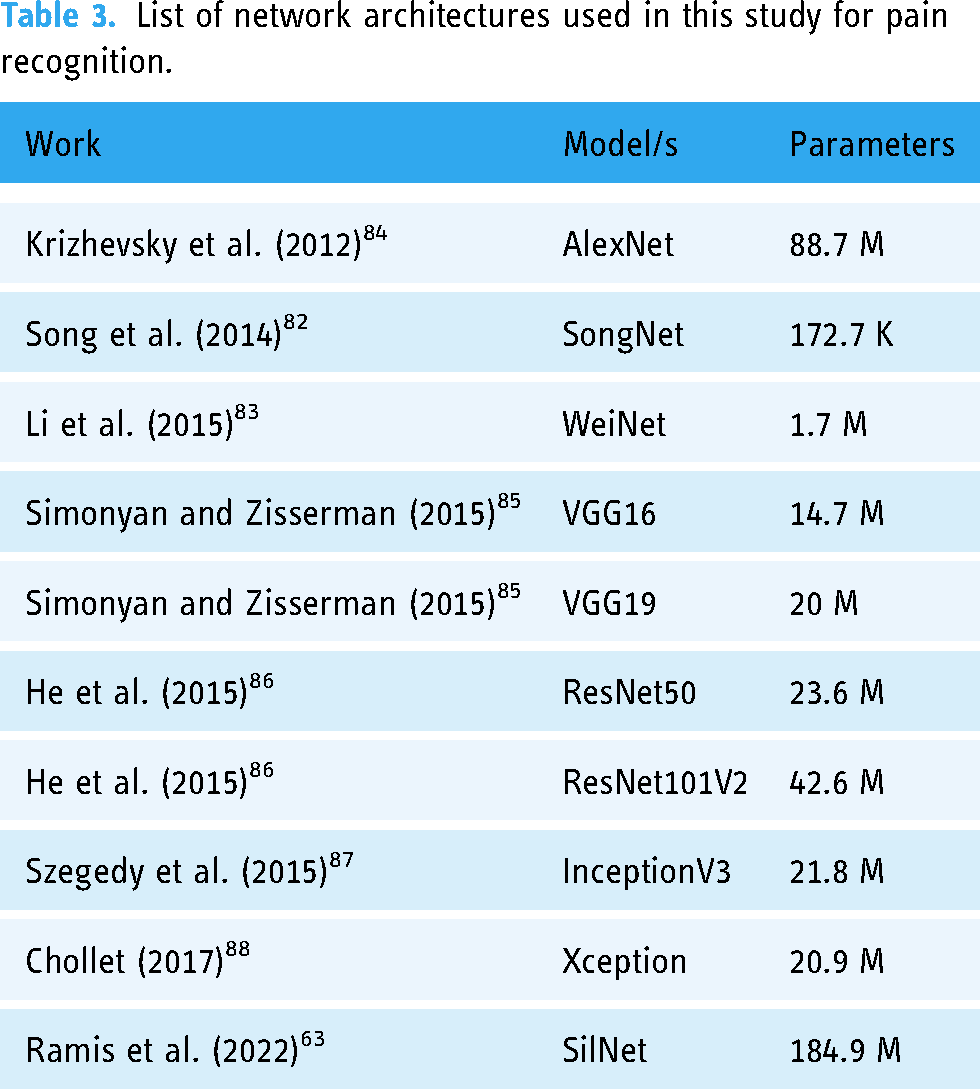
All the employed networks share a foundation in convolutional architecture; however, they diverge in terms of architectural constituents, including the arrangement of convolutional layers, pooling layers, fully connected layers, and other elements. This architectural disparity is reflected in the count of parameters employed by each network. The input size of the networks is 224 × 224, with the exception of WeiNet and SilNet, which is 64 × 64 and 150 × 150 respectively.
Six out of the ten models—VGG16, VGG19, ResNet50, ResNet101V2, Xception, and InceptionV3—were initialized with pre-trained weights sourced from the ImageNet dataset. 89 For these models, final fully connected layers were replaced with an average 2D pooling layer and a new fully connected layer with the appropriate number of outputs: two, pain and no pain. The remaining models—AlexNet, SongNet, WeiNet, and SilNet—were trained from scratch.
By integrating these varied architectures, we can compare their performance and analyze the impact of architectural selections concerning tasks related to pain recognition.
The models were implemented using the Python programming language, harnessing the capabilities of the Keras library. In the case of the AlexNet, WeiNet, SongNet, and SilNet models, we constructed each layer sequentially within the Keras framework. Conversely, the remaining models were conveniently available through the Keras API, inclusive of their pre-trained weights sourced from the ImageNet dataset.
Metrics
To assess the performance of the different models, common metrics used when evaluating classification tasks, namely accuracy, precision, recall, and F1-score, were used (TP, TN, FP, and FN used in the equations to refer, respectively, to the number of true positives, true negatives, false positives, and false negatives): Accuracy (equation (1)): it measures the proportion of correctly classified instances among the total instances in the dataset. It provides an overall view of the model's correctness. However, it might not be suitable when dealing with imbalanced datasets where one class dominates, as it can be misleading. Precision (eq. (2)): it is a measure of how many of the instances predicted as positive by the model are actually true positives. It focuses on the correctness of positive predictions. High precision indicates that the model is careful in labeling instances as positive. Recall (eq. (3)): it quantifies how many of the actual positive instances were correctly predicted by the model. It emphasizes the model's capability to capture all positive instances. F1-Score (eq. (4)): it is the harmonic mean of precision and recall. It combines both precision and recall into a single value, providing a balanced assessment of a model's performance. It is particularly useful when dealing with imbalanced datasets or situations where both false positives and false negatives are of concern.



When evaluating a model's performance in image classification, these metrics collectively provide a comprehensive understanding of its strengths and weaknesses. Accuracy gives a global view of performance, precision focuses on correct positive predictions, recall emphasizes capturing all true positives, and F1-score offers a balanced perspective considering both precision and recall. Using this set of metrics ensures a nuanced assessment of a model's effectiveness in classifying images accurately and reliably, even in scenarios where data distribution might be uneven or where the cost of false positives and false negatives differs significantly.
Models’ explanation
We applied the model-agnostic XAI technique known as Local Interpretable Model-agnostic Explanations (LIME). 90 LIME operates by introducing perturbations to the image under examination, thereby generating multiple modified versions of the image. These perturbed samples are subsequently processed through the model, and the resulting prediction outcomes are employed to establish the relevance of each region within the image with respect to a specific class. To further understand the classification processes employed by the models, we generalized the local explanations derived from a subset of samples to formulate global explanations for each class. This approach followed the methodology introduced in Manresa-Yee et al. (2023), 91 where local explanation masks are transformed into a normalized space and then averaged to produce a comprehensive heatmap that delineates the significance of individual facial features in the classification process. For a better comprehension of the explanation process, Figure 3 provides a visual representation of the distinct steps involved.
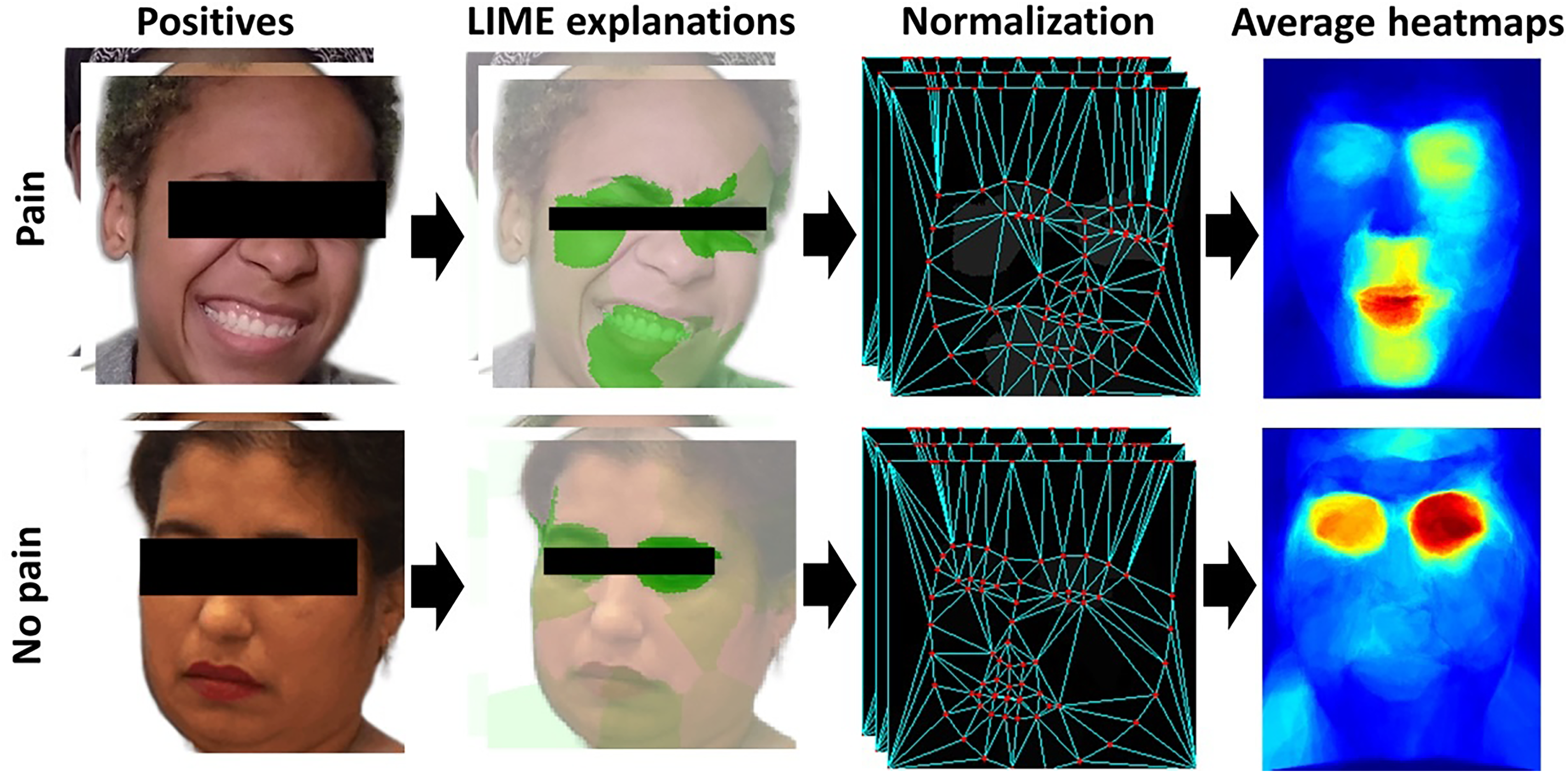
Visualization of the explanation process followed for the identification of the important regions for a specific model to classify into a class.
Procedure
All trainings for the ten networks were performed on a computer featuring an NVIDIA 4090 GPU and an i9 9900KF CPU, generously supplied by the Universitat de les Illes Balears. This same hardware configuration was consistently employed for the evaluation phase. Overall, we did not encounter any notable challenges or limitations with the selected hardware configuration. It adequately supported the execution of our experiments without impeding our ability to achieve meaningful results.
Following a series of preliminary experimental iterations, we conducted several training sessions, each comprising 50 epochs, on a training–validation partition of the dataset. Through this process, we systematically varied the learning rate across three orders of magnitude (0.01, 0.001, and 0.0001) and assessed the resulting performance on the validation set. Based on these evaluations, we determined that a learning rate of 0.001 yielded the highest accuracy. Similarly, we monitored the training and validation loss curves across epochs to gauge the model's convergence and generalization capabilities. After observing diminishing returns beyond 30 epochs, we determined that this value struck a favorable balance between performance and training time. Additionally, continuing training beyond this point did not yield significant improvements in validation loss, indicating the risk of overfitting. Additionally, data augmentation layers were incorporated into the training pipeline, encompassing randomized processes such as rotation, mirroring, and contrast adjustment. This integration aimed at introducing invariance to these intrinsic properties while concurrently augmenting the spectrum of image variations during training.
Regarding the utilization of pretrained weights, we adopted a cautious approach to mitigate the risk of overfitting, given the relatively small size of our training dataset. We experimented with various fine-tuning strategies, including freezing lower blocks of the models and training only the last layers, training the entire model, and a combination of both. Surprisingly, freezing the lower blocks did not yield performance improvements in our case; instead, it hindered the convergence speed during training. As a result, we opted to fine-tune the entire model on our dataset and task, with no frozen layers left.
The experimental design comprised a total of three training scenarios for each of the ten models detailed in the Models Section. Further, we employed K-cross validation with K = 5 to ensure more stable and reliable results, for each of the three training scenarios, 150 trainings were performed in total. Regarding the choice of K = 5 in the K-cross validation, this decision was made to strike a balance between the number of training iterations and the reliability of the results, providing a reasonable approximation of model performance while avoiding excessive computational overhead. Overall, the K-cross validation approach enhanced the stability and reliability of our results by mitigating the variability that can arise from different data partitions or training iterations.
Initially, the merged PAIN-DB dataset was partitioned into training and testing subsets, maintaining an 80%–20% and with varying test subsets, according to the K-cross validation procedure. This training phase involved models being trained on nearly all users’ data, thereby assessing their performance in predicting pain based on images from users they had previously encountered. This training configuration aimed to yield the most optimal outcomes among the three.
The second training iteration closely resembled the initial one, using the PAIN-DB dataset. However, in this iteration, the partitioning was user-centric rather than image-centric, while preserving the same train-test ratio. Here, models were trained using images from a subset of users, with the remaining users reserved for the testing phase. This approach sought to evaluate the models’ ability to accurately perceive pain within images of users unseen during training.
Finally, a training with the entire PAIN-DB dataset was conducted, testing on the pain images collected from individuals of the CP-PAIN dataset. The primary distinction here was that models were evaluated on users external to the PAIN-DB dataset. For this particular training scenario, there was no K-cross validation, but rather five different trainings on the same data, since the testing set is external to the PAIN-DB dataset. This third scenario aimed to validate the extrapolation of knowledge gained from the PAIN-DB dataset to the CP-PAIN dataset, which presented additional challenges due to its external nature and inclusion of users with cerebral palsy. The main challenge with the CP-PAIN dataset was its limited size, which precluded direct training on it. Instead, we sought to generalize the models trained on the PAIN-DB dataset to the CP-PAIN dataset.
The three-tiered approach to experimentation was devised to sequentially validate network performance on well-established pain recognition datasets. This stratification allowed for enhanced assessment of model effectiveness on a novel dataset, the size of which precluded fine-tuning strategies.
Results
Inter-rater agreement among physiotherapists
In the course of the study, both physiotherapists conducted a grand total of 762 assessments, all stemming from the scrutiny of 127 video recordings. The inter-rater agreement, measured through the ICC, exhibited the following hierarchy of agreement levels for the observational measures:
FACS = 0.751 (excellent) Wong-Baker Faces pain rating scale = 0.639 (fair/good) NCAPC = 0.551 (fair/good)
For a more comprehensive understanding of the inter-rater agreement contingent on the type of painful stimulus, refer to Table 4.
ICC of observational measures and pain/no pain measurement proportion.
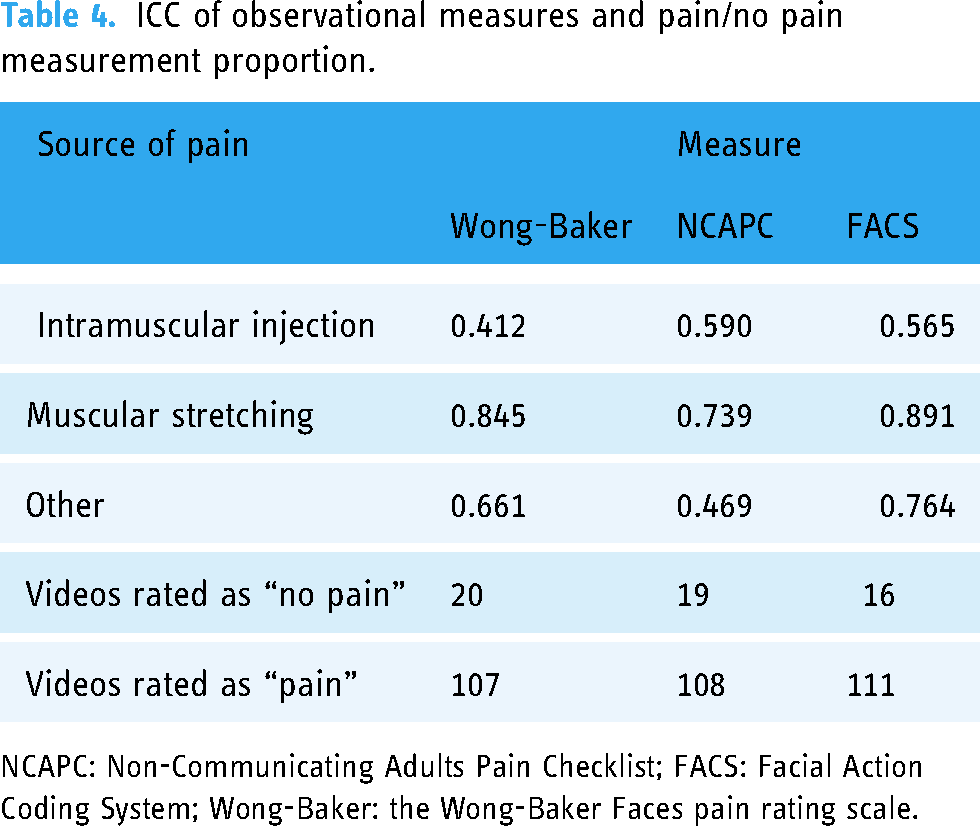
NCAPC: Non-Communicating Adults Pain Checklist; FACS: Facial Action Coding System; Wong-Baker: the Wong-Baker Faces pain rating scale.
These findings show a higher ICC across all scales when pain was induced by muscular stretching (mean of 3 scales = .825, excellent ICC), followed by an unknown source of pain (mean of 3 scales = .632, fair ICC), and lastly, intramuscular injection (mean of 3 scales = .522, fair ICC). Given that FACS exhibited the highest level of agreement, it was employed to label the image into the “pain”/”no pain” classes.
Deep learning pain recognition
The outcomes derived from the three distinct training scenarios are presented in Figure 4. As expected, the initial scenario, where networks were evaluated on users they had encountered during training, yielded the most favorable results overall. Notably, upon assessment with previously unencountered users, a marginal reduction was observed in both accuracy and F1 score across most networks. The third scenario, involving testing on users from the distinct CP-PAIN dataset, led to slightly diminished metrics. Among the models assessed, merely three attained performance levels surpassing 70%: InceptionV3, ResNet101V2, and Xception. Remarkably, InceptionV3 exhibited the most promising outcomes on the CP-PAIN dataset, attaining an accuracy of 62.67% alongside an F1 score of 61.12%. Examples of the pain recognition task of this model on the different datasets, including true positives and false negatives, can be found in the appendix section. We expect these examples to provide a more tangible understanding of the model's capabilities.

Accuracy (top) and F1 score (bottom) of the pain prediction results of the three different trainings performed, displayed by network. The values correspond to the average between the five validation splits, for each training scenario.
Figure 5 illustrates precision and recall values for each class (pain and no pain) on the CP-PAIN dataset. The precision values across networks display a relatively balanced distribution between classes. Interestingly, the recall values, which highlight the model's aptitude for identifying specific classes, underscore a consistent trend toward pain prediction over no pain prediction for all networks. This trend is particularly pronounced in certain models such as AlexNet, VGG19, ResNet50, and Xception, which achieve a recall of 80% or higher for pain but exhibit figures of 20% or lower for no pain instances. In contrast, InceptionV3, ResNet101V2, and SilNet exhibit more balanced recall values. This balance is further translated into higher F1 scores, as depicted in the lower chart of Figure 4.

Precision (top) and recall (bottom) of the pain prediction results by class on the CP-PAIN dataset, displayed by network. The values correspond to the average between the five validation splits, for each training scenario.
Figure 6 presents heatmaps that illustrate the significance of distinct facial regions in predicting a specific class for each of the trained models. Evidently, there exists subtle divergence among the models regarding the specific facial regions they emphasize when discerning the presence or absence of pain. However, noticeably, the heatmaps from models with pre-training and those without pre-training appear to segregate into two distinct clusters. This observation suggests a proclivity for models within each category to prioritize particular facial regions to a greater or lesser extent during the classification process.
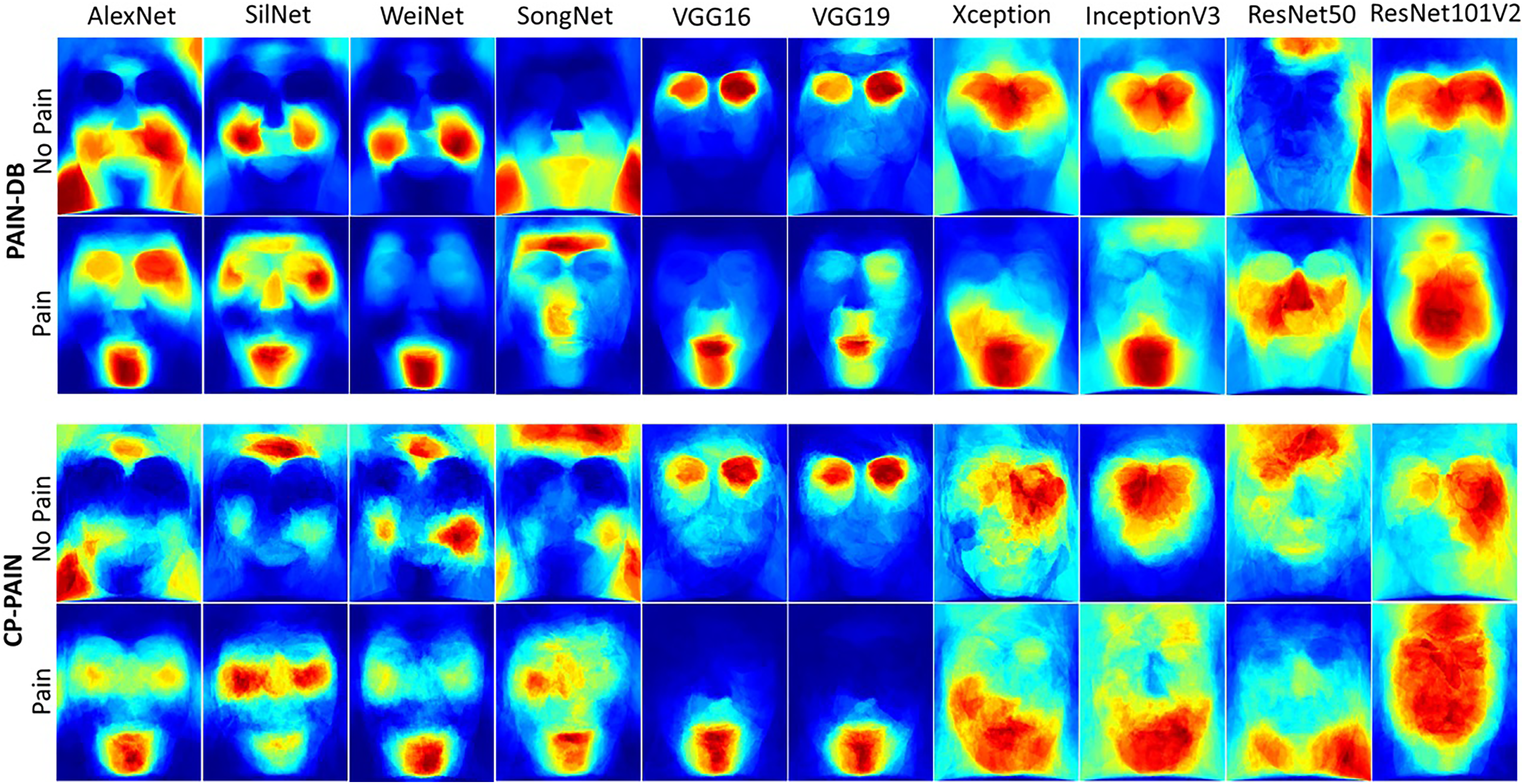
Heatmaps representing face regions importance for the different models, classes, and databases.
In an ideal scenario, the models should exhibit similar heatmaps when applied to both the PAIN-DB and CP-PAIN datasets. However, as depicted in Figure 6, certain models deviate from this ideal alignment. SilNet, WeiNet, and SongNet prominently emphasize the forehead region when classifying instances as “Not pain” in the CP-PAIN dataset, a pattern not evident in the PAIN-DB dataset. This disparity underscores the substantial impact of database differences on model predictions. Similarly, ResNet50 also demonstrates distinct results by focusing on the lower facial region for pain recognition in CP-PAIN, while primarily centering on the central facial area in the case of the PAIN-DB dataset. In contrast, the remaining models appear to exhibit relatively consistent reliance on the same facial regions, irrespective of the database under consideration. Another noteworthy observation pertains to the importance of the lower portion of the face, particularly encompassing the mouth and its vicinity, which emerges as a pivotal factor in pain recognition. Conversely, the absence of pain is predominantly associated with the upper facial region, particularly focusing on the eyes and their surroundings.
Discussion
The primary objective of this study was to develop an automated facial recognition system based on DL for the assessment of pain in adults with CP. To achieve this goal, we developed and trained this system using a specific dataset of images of individuals with CP (CP-PAIN) curated for this very purpose and three existing well-known pain databases. Subsequently, we compared pain scores obtained from the automated facial recognition system with the pain scores provided for each image of the CP-PAIN dataset, obtained by consensus by two independent physiotherapists experienced in caring for individuals with CP. Our findings revealed a 60% accuracy rate for the facial recognition system, thus confirming the feasibility of adapting pain detection from images for patients with CP.
To the best of our knowledge, this study marks a pioneering initiative introducing pain detection through image analysis for individuals with CP. This innovation has the potential to offer valuable solutions for evaluating pain within this population, a challenge often noted by clinicians and family members alike. 21 Beyond addressing this pressing need, the application of image-based pain detection has the added advantage of mitigating the intrinsic subjectivity inherent in human pain assessments,31–33 thereby reducing associated inaccuracies. Our findings reflect a noteworthy aspect of this subjectivity. Even in cases where the evaluator has a deep familiarity with the individual with CP under assessment, our results revealed the presence of a subjective bias that depends on the evaluator's level of familiarity with the specific painful procedure being evaluated. To this regard, physiotherapists exhibited a higher level of agreement when assessing pain induced by muscle stretching compared to pain resulting from intramuscular injection or an unknown source of pain. This subjectivity in pain assessment has been demonstrated in other studies that measured the degree of agreement between individuals with cerebral palsy and their parents,35,36 as well as with healthcare professionals. 37 This highlights the importance of objective, technology-assisted approaches in enhancing the precision and objectivity of pain assessment in individuals with CP.
Given the scarcity of relevant patient data for training, we devised a strategy involving the training of pain detection models on established datasets tailored for this task. Subsequently, the models’ performance was evaluated on a minimal test set, CP-PAIN, constructed specifically for this study, which comprises images of users with CP, both with and without pain. Despite the limited number of images contained in CP-PAIN, this dataset is the first of its kind. Cognitive factors and motor impairment may affect the gestures, body movement, and mimics in individuals with neuromotor disorders, such as individuals with CP, what could lead to idiosyncratic pain expressions or mask pain of low intensity.71,92–94 Our approach incorporates a specific dataset of pain in this population that may help enhance DL pain recognition. Further refinement and expansion of our dataset can harness the power of DL to create a more robust and reliable pain detection system. The need for a larger and more diverse image datset becomes evident as we strive to train our DL model to better recognize nuanced pain expressions in this unique population. Although limited and prone to expansion and quality improvement, the CP-PAIN database could be a first contribution to the DL analysis of pain expressions in complex populations with pain facial expressions diverse from those of the general population,71,92–94 collected in other existing databases.
Initially, the performance achieved on the training set reached a maximum of 70% for users unknown to the models. Consequently, this outcome can be considered an upper-bound estimation for the performance attainable on CP-PAIN. Acknowledging this modest performance, likely attributed to the limited training data, we plan to enhance these results in future work by diversifying the training datasets. Additionally, we emphasize the necessity for meticulous analysis of images from each database, particularly those extracted from video recordings, since the imprecision in annotations during video frame selection could introduce a significant number of erroneously labeled images, warranting careful consideration.
Our findings on the CP-PAIN dataset unveiled 60% accuracy, thereby establishing the viability of adapting pain detection from images to patients with CP. A noteworthy trend emerged where the models exhibited a pronounced trend towards detecting pain in images, surpassing instances of identifying no pain. This proclivity could be attributed to the frequent appearance of subjects in the test images exhibiting open mouths and exposed teeth, a phenomenon potentially associated by the networks with pain expressions seen during training. This accuracy in pain detection, while seemingly modest, marks a significant milestone in clinical research, as it underscores the potential for developing a specialized assessment model tailored to individuals with complex neuromotor conditions, a development that holds promise in reducing the inherent subjectivity and biases often associated with human evaluations of pain.20–22
Comparing the results obtained in this study with existing literature in terms of measurable performance is challenging due to several factors. 95 Firstly, different datasets were used, making direct comparison difficult. Secondly, this study does not exploit temporal information, which was considered in other works. Thirdly, many works aim for pain level classification, rather than solely classification between pain and no pain in images. No other work employing the same four datasets (UNBC-McMaster Shoulder Pain Expression Archive Database, Mint PAIN Database, Delaware Pain Database, and CP-PAIN) as this study has been found. Typically, existing studies focus on testing new models or strategies and optimizing performance on a single dataset rather than generalizing results to unseen datasets. For instance, many studies prefer using the UNBC dataset, with varying results over the years: 86.10% accuracy, 96 87.20%, 97 76.00%, 98 and 93.16%, 99 using the Leave-One-Subject-Out (LOSO) cross-validation method. It is worth noting that these results, while higher than those obtained in this study, were achieved on a single dataset using a different cross-validation method, making direct comparisons unfair. No other works utilizing the MInt pain database with solely 2D information were found, and no deep learning-based approaches were identified for the Delaware dataset, likely due to its reduced size. Therefore, while comparisons with existing literature may be challenging, this study contributes valuable insights by leveraging multiple datasets, which may enhance the generalizability and robustness of the findings. Furthermore, we were unable to find prior work that included users with CP, making direct comparisons with our results on the CP-PAIN dataset unfeasible. As pioneers in studying automatic pain recognition among individuals with cerebral CP, our study lays the foundation for future research in this area.
Given the focus on real-world applicability, the scalability of our automated facial recognition system is a critical consideration. While the system was not specifically trained on individuals with cerebral CP, the results obtained from the CP-PAIN dataset can reasonably generalize to other individuals within the CP population. This assumption is grounded in the understanding that the users in the CP-PAIN dataset represent a sample from the broader CP population and are likely to share common characteristics in their pain expressions. However, challenges may arise when deploying the system in diverse environments or when faced with varying degrees of pain expressions within the CP population. As the system is deployed in different settings, the availability of more data from individuals with CP will likely increase. This presents an opportunity for fine-tuning the models using CP-specific data, thereby enhancing the system's performance in pain recognition tailored to this population. Moreover, further exploration of the similarities in pain expression among individuals with CP can provide valuable insights for improving the system's accuracy and reliability in real-world scenarios.
For the models exhibiting the highest performance, such as InceptionV3 and ResNet101V2, the application of XAI techniques have unveiled an interesting finding: when employing models trained on the PAIN-DB dataset on users with CP, the essential regions crucial for accurate pain identification remain largely unaffected. The consistent focus of these two models on identical facial regions for pain recognition both for users with CP and without suggests a noteworthy similarity in the expression of pain between these two distinct groups. However, it is essential to acknowledge that this finding does not consider potential idiosyncrasies in the facial expression of pain in subjects with complex neurological disorders, which may have led to the presence of false positives. It is important to note that some idiosyncratic behaviors, such as crying, moaning, flinching, having red cheeks, grunting, or sticking out the tongue can be misleadingly labeled as pain within the CP population, while they can express other physiological or emotional events. 93 On the contrary, other facial gestures, such as smiling or laughing, may be used to express pain in individuals with poorer communication or motor ability. 94 This underscores the need for further training of the system using a more diverse dataset of images of individuals with CP. We are committed to addressing potential variations in the expression of pain and enriching the robustness of our models for pain recognition across diverse user groups. This approach would ensure a more precise and reliable application of our technology in clinical and medical settings.
This study was not without limitations. In addition to the previously mentioned constraint of a limited number of images in our database, we also faced the unforeseen challenge of not being able to collect self-reports from most individuals with CP, as originally planned, what would have been valuable to evaluate the facial recognition system's measurements in a more accurate way. Another potential limitation was the unequal representation of different types of painful stimuli.
DL pain recognition allows envisioning the possibility of mitigating the limitations of human-based assessments of pain in complex conditions, such as CP, and achieving a level of objectivity and consistency that can significantly benefit the care and well-being of individuals with communication problems and cognitive and neuromotor disorders affecting pain expression. Therefore, our work not only showcases the potential of adapting technology for healthcare applications but also emphasizes the importance of ongoing research and data collection to advance and extrapolate the capabilities of our model in the future.
Conclusions
Our study addresses the profound challenges in pain assessment for individuals with CP, highlighting the limitations of existing methodologies and the need for approaches tailored to this unique population. Unlike conventional studies that often utilize datasets and models designed for neurotypical individuals, our research introduces an innovative approach by developing and employing the CP-PAIN dataset. This dataset is specifically designed to capture the diverse and often unique expressions of pain characteristic of individuals with CP, highlighting a significant departure from the broader application DL models prevalent in current research. Our efforts to customize DL models for the CP population underscore the complex nature of pain expressions in these individuals, which are not adequately addressed by standard facial recognition systems.
Despite showing promise, with an initial accuracy rate of 60%, our findings also signal the need for further enhancements and the expansion of the CP-PAIN database. A more comprehensive collection of data is essential for refining DL models to accurately identify the nuanced pain expressions of individuals with CP, a step towards developing a universally applicable pain assessment tool. Our study not only contributes to the specialized field of pain assessment in CP but also emphasizes the critical importance of ongoing research. By focusing on the unique needs of individuals with CP, we underscore the broader challenge of creating more inclusive and accessible pain assessment methodologies. This endeavor not only advances our understanding of pain assessment in the context of CP but also sets a precedent for the importance of tailoring research and technology to meet the specific needs of underserved populations.
Finally, in addressing the ethical and privacy implications of using automated facial recognition for pain assessment in clinical settings, it is crucial to obtain transparent informed consent, protect sensitive biometric data through strict adherence to data protection laws and advanced encryption, and prevent bias to ensure equitable patient assessments. Continuous stakeholder engagement and system evaluation are imperative for upholding ethical standards and patient privacy.
Supplemental Material
sj-png-1-dhj-10.1177_20552076241259664 - Supplemental material for Automated facial recognition system using deep learning for pain assessment in adults with cerebral palsy
Supplemental material, sj-png-1-dhj-10.1177_20552076241259664 for Automated facial recognition system using deep learning for pain assessment in adults with cerebral palsy by Álvaro Sabater-Gárriz, F Xavier Gaya-Morey, José María Buades-Rubio, Cristina Manresa-Yee, Pedro Montoya and Inmaculada Riquelme in DIGITAL HEALTH
Supplemental Material
sj-png-2-dhj-10.1177_20552076241259664 - Supplemental material for Automated facial recognition system using deep learning for pain assessment in adults with cerebral palsy
Supplemental material, sj-png-2-dhj-10.1177_20552076241259664 for Automated facial recognition system using deep learning for pain assessment in adults with cerebral palsy by Álvaro Sabater-Gárriz, F Xavier Gaya-Morey, José María Buades-Rubio, Cristina Manresa-Yee, Pedro Montoya and Inmaculada Riquelme in DIGITAL HEALTH
Supplemental Material
sj-png-3-dhj-10.1177_20552076241259664 - Supplemental material for Automated facial recognition system using deep learning for pain assessment in adults with cerebral palsy
Supplemental material, sj-png-3-dhj-10.1177_20552076241259664 for Automated facial recognition system using deep learning for pain assessment in adults with cerebral palsy by Álvaro Sabater-Gárriz, F Xavier Gaya-Morey, José María Buades-Rubio, Cristina Manresa-Yee, Pedro Montoya and Inmaculada Riquelme in DIGITAL HEALTH
Supplemental Material
sj-png-4-dhj-10.1177_20552076241259664 - Supplemental material for Automated facial recognition system using deep learning for pain assessment in adults with cerebral palsy
Supplemental material, sj-png-4-dhj-10.1177_20552076241259664 for Automated facial recognition system using deep learning for pain assessment in adults with cerebral palsy by Álvaro Sabater-Gárriz, F Xavier Gaya-Morey, José María Buades-Rubio, Cristina Manresa-Yee, Pedro Montoya and Inmaculada Riquelme in DIGITAL HEALTH
Supplemental Material
sj-docx-5-dhj-10.1177_20552076241259664 - Supplemental material for Automated facial recognition system using deep learning for pain assessment in adults with cerebral palsy
Supplemental material, sj-docx-5-dhj-10.1177_20552076241259664 for Automated facial recognition system using deep learning for pain assessment in adults with cerebral palsy by Álvaro Sabater-Gárriz, F Xavier Gaya-Morey, José María Buades-Rubio, Cristina Manresa-Yee, Pedro Montoya and Inmaculada Riquelme in DIGITAL HEALTH
Supplemental Material
sj-docx-6-dhj-10.1177_20552076241259664 - Supplemental material for Automated facial recognition system using deep learning for pain assessment in adults with cerebral palsy
Supplemental material, sj-docx-6-dhj-10.1177_20552076241259664 for Automated facial recognition system using deep learning for pain assessment in adults with cerebral palsy by Álvaro Sabater-Gárriz, F Xavier Gaya-Morey, José María Buades-Rubio, Cristina Manresa-Yee, Pedro Montoya and Inmaculada Riquelme in DIGITAL HEALTH
Supplemental Material
sj-docx-7-dhj-10.1177_20552076241259664 - Supplemental material for Automated facial recognition system using deep learning for pain assessment in adults with cerebral palsy
Supplemental material, sj-docx-7-dhj-10.1177_20552076241259664 for Automated facial recognition system using deep learning for pain assessment in adults with cerebral palsy by Álvaro Sabater-Gárriz, F Xavier Gaya-Morey, José María Buades-Rubio, Cristina Manresa-Yee, Pedro Montoya and Inmaculada Riquelme in DIGITAL HEALTH
Footnotes
Abbreviations
Acknowledgements
The authors would like to thank the healthcare staff of the ASPACE Balearic Foundation and APACE Toledo for their various contributions during the development of this study.
Contributorship
AS-G and IR researched the literature and conceived the study. AS-G, IR, and PM were involved in protocol development, gaining ethical approval, and recruiting patients. JMBR and CMY worked on the conceptualization of the experiment. FXGM and JMBR conducted the experiments. AS-G carried out the data analysis. AS-G, FXGM, and CMY wrote the initial draft of the manuscript. All authors reviewed, edited, and approved the final version of the manuscript.
Ethical approval
The research protocol received approval from both the ASPACE Foundation's ethics committee and the Research Ethics Commission of the Balearic Islands (protocol number IB4046/19), affirming its ethical rigor.
Guarantor
IR
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by MICIU/AEI/ 10.13039/501100011033 Spain, grants PID2020-114967GA-I00 (SENTS?) and PID2019-104829RA-I00, EXPLainable Artificial INtelligence systems for health and well-beING (EXPLAINING) and for the Ministry of Science and Technology of Spain /Spanish Foundation for Science and Technology (FECYT, grant FCT-20-16485). In addition, the authors also acknowledge the funding of the FPU scholarship from the Ministry of European Funds, University and Culture of the Government of the Balearic Islands.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.