
Abstract
Objective
To determine the effects of motor and intellectual functions on the effectiveness of comprehensive rehabilitation (CR) in young children with cerebral palsy (CP).
Methods
This longitudinal cohort study recruited paediatric patients with a confirmed diagnosis of CP. Baseline gross motor function was classified using the Gross Motor Function Classification System. Baseline intellectual level was evaluated using the Developmental Quotient (DQ) via the Gesell Development Scale. Children underwent CR for 3 months and then their motor and intellectual functions were assessed using the Gross Motor Function Measure, Fine Motor Function Measure and DQ. The changes from baseline were calculated.
Results
Forty-eight children with CP were recruited to this study. Greater improvements in motor function were associated with a lower baseline level of intellectual impairment. Motor and intellectual function in children with CP was significantly improved when treatment was started before 12 months of age.
Conclusion
There might be a close and reciprocal relationship between the baseline levels of impairment of motor and intellectual function with regard to the effectiveness of CR. Early intervention is important to gain a good outcome in children with CP.
Introduction
Cerebral palsy (CP) is one of the major diseases seen in children (2.0–3.5 cases per 1000 live births). 1 It describes a group of permanent disorders of the development of movement and posture, causing activity limitation, which are attributed to nonprogressive disturbances that occurred in the developing fetal or infant brain. The motor disorders of cerebral palsy are often accompanied by disturbances of sensation, perception, cognition, communication and behaviour, by epilepsy, and by secondary musculoskeletal problems. 1 The motor disability of CP varies according to the degree of brain damage, ranging from minor dysfunction to the severe impairment. Based on impairment of spontaneous movement, trunk control and walking ability, the Gross Motor Function Classification System (GMFCS) has been developed and widely used for evaluating the severity of age-specific gross motor dysfunction in CP cases.2–4 GMFCS grading has been shown to be reliable across observers and invariant with increasing age. 5 The GMFCS classifies gross motor function on a five-degree ordinal scale (level I represents the best gross motor abilities; level V the least function), with descriptions of skills provided for five age bands for each level: before the second birthday; age 2–4 years; age 4–6 years; age 6–12 years; adolescence. However, for quantitative evaluation of motor function, the Gross Motor Function Measure (GMFM) is used the most frequently, globally, to assess the effectiveness of interventions in children with CP. 6
Cerebral palsy is usually accompanied by intellectual impairment, with rates of affected children varying between 40% and 65%.7–9 Intellectual capacity is defined as the general mental ability to adapt to the living environment, including logical reasoning, problem solving and abstract thinking. Intellectual impairment in children with CP commonly implicates phonological awareness, verbal working memory skills, arithmetic skills, literacy skills and functional skills in the domains of mobility, self-care or social functioning. 10 The Gesell Development Scale (GDS) was firstly described by American psychologist Arnold Gesell (1880–1961). It is widely used to assess mental development via a Developmental Quotient (DQ) value at specific ages.11–13 As the level of intellectual capacity is pivotal for daily-life functioning and life expectancy, it has attracted growing interest in CP studies. Abundant evidence is available concerning the relationship between intelligence and motor function; and it is widely accepted that intelligence is important for both learning and completing a complex motor task.14,15 The combination of severe motor impairment with severe learning disability is defined as ‘severe CP’ in Europe. 16 Moreover, children with CP who have severe motor impairment commonly present with salient intellectual disability. 17 Accordingly, both gross motor function and intellectual capacity might implicate mechanisms underlying experience-dependent information processing, initiated by external stimuli from the environment and related to active formation and optimization of synaptic connections. 18 A longitudinal study showed that the GMFCS level was a negative predictor for change of language, social function, and self-help. 19 A cross-sectional study demonstrated that the level of motor impairment was strongly correlated with the intellectual level in children with CP. 15
In the past decade, many physical therapies have become available, but little evidence exists on which to choose. Although different rehabilitation centres using slightly different approaches, they all share similar core principles. 1 The key point and optimal management for CP is to minimize the effect of medical difficulties while maximizing physical ability, environmental adjustment, child and family choice, and social support. Traditional physiotherapy and occupational therapy are widely used interventions and have been shown to be of benefit in the treatment of CP. 20 In addition, various therapeutic interventions have been used for CP therapy, including speech therapy, 20 deep brain stimulation, 21 botulinum toxin A injection, 22 sensory integration, 20 body-weight support treadmill training, 20 conductive education, 20 constraint-induced therapy, 20 hyperbaric oxygen therapy, 20 and traditional Chinese therapy (TCT).20,23–25 A meta-analysis in 3286 children that systematically evaluated the effects of TCT (including massage, oral herbal medicine, herbal bathing and acupuncture) demonstrated that TCT may have benefit in children with CP. 26 However, the effectiveness of these interventions still needs to be validated in controlled trials. Moreover, the optimal time to initiate treatment remains unknown, although it is often thought that early treatment would be of more benefit to the recovery of motor function and intelligence, in children with CP.19,27
This present study examined the hypothesis that baseline motor and intellectual impairments may have an important role to play in determining the outcome of treatment interventions. It also evaluated when is the best time to initiate treatment is in children with CP. To date, whether the level of motor impairment and intellectual disability affect the efficacy of comprehensive rehabilitation (CR), including some items of TCT, in young children with CP has not been reported. This present study analysed clinical data from children with CP to determine the effects of baseline motor and intellectual functions on the effectiveness of 3 months’ treatment with CR.
Patients and methods
Participants
This longitudinal cohort study recruited paediatric patients from the Paediatric Neurological Rehabilitation Department of the First Bethune Hospital of Jilin University, Changchun, Jilin Province, China between July 2010 and January 2011. Children with a confirmed diagnosis of CP were enrolled in this study. 28 In order to avoid the influence of progressive brain injury, and to be suitable to undergo the CR therapy programme, children were excluded from the study if they presented with additional disorders affecting motor function, including epilepsy, and severe auditory or visual impairments. Because of the difficulties associated with confirming a CP diagnosis in very young children, and in order to avoid a delay in the initiation of the correct treatment, CR therapy was initiated slightly prior to the establishment of a CP diagnosis (age range 4.6–22.3 months) in this study. Children who were lost to follow-up were excluded. To examine the effect of early initiation of CR therapy, participants were grouped according to their age at which CR treatment was initiated. CP subtypes were classified according to the quality and topographic pattern of motor impairment. 29 Written informed consent was obtained from all parents of the children at study entry. Ethical approval for the study was given by the Medical Ethics Committee of the First Bethune Hospital of Jilin University.
Measures of motor and intellectual function
The GMFCS was used to classify the gross motor impairment of children with CP in this study. 13 GMFCS levels for children aged <2 years were as follows: 30 (i) level I – infants move in and out of sitting and sit on the floor with both hands free to manipulate objects. Infants crawl on hands and knees, pull to stand, and take steps holding onto furniture. Infants walk between 18 months and 2 years of age without the need for any assistive mobility device; (ii) level II – infants maintain floor sitting but may need to use their hands for support, to maintain balance. Infants creep on their stomach or crawl on hands and knees. Infants may pull to stand and take steps holding onto furniture; (iii) level III – infants maintain floor sitting when the lower back is supported. Infants roll and creep forward on their stomachs; (iv) level IV – infants have head control but trunk support is required for floor sitting. Infants can roll to supine and may roll to prone; (v) level V – physical impairments limit voluntary control of movement. Infants are unable to maintain antigravity head and trunk postures in prone and sitting. Infants require adult assistance to roll.
The GMFM was used for the quantitative evaluation of the gross motor impairment. The version of the GMFM used was GMFM-88, which has been categorized into five dimensions of gross motor function: lying and rolling (17 items); sitting (20 items); crawling and kneeling (14 items); standing (13 items); walking, running and jumping (24 items). 31 The stability and reliability of GMFM-88 were well validated in this study and by other Chinese therapists. 32
The Fine Motor Function Measure (FMFM) is a scale developed by the Rehabilitation Centre of the Children’s Hospital of Fudan University in China, from Rasch analysis in children with CP, aged 0–3 years.33–35 The reliability, validity, and responsiveness of the FMFM have been well validated and evaluated by neurologists in several Chinese studies.34–36 The FMFM scale consists of five functional domains (69 items in total): visual pursuit (11 items); upper extremity joint motor activity (15 items); grasp ability (15 items); performance ability (12 items); hand–eye coordination (16 items). Each item ranges between 0 (lowest motor function) and 4 (highest motor function), and the sum total score is calculated to indicate fine motor function.
As for the evaluation of intellectual function, a revised GDS was established in 1984, based on the original version of the GDS, which was revised in 1994 by Chinese scholars to assess the DQ value. 37 The revised GDS includes five areas: cognitive function; use of language; motor functioning; ability to adapt; individual social behaviours. The revised GDS has 50 items covering five functional areas; each item has four questions and five degrees of score.38,39 The intellectual impairment was assessed using the DQ value via the revised GDS, involving the adaptive area, language area and social area. Children were graded accordingly: normal, DQ > 84; borderline, 75–84; mild disability, 55–74; moderate disability, 40–54; severe disability, 25–39; profound disability, < 25.
Study procedures
Gross motor impairment of children with CP was classified using the GMFCS at study entry (baseline). Baseline gross and fine motor functions were assessed using the GMFM and FMFM, respectively. Baseline intellectual level was evaluated using the DQ score via the revised GDS. After the baseline evaluation using the GMFM, FMFM and revised GDS was undertaken, all subjects underwent CR treatment 6 days per week for 3 months in the Daytime Ward of the Rehabilitation Centre, First Bethune Hospital of Jilin University. CR consisted of physical therapy (PT), occupational therapy (OT), language therapy (LT), hyperbaric oxygen (HO), herbal steaming (HS), Chinese massage (CM), meridian mediation (MM), muscle stimulation (MS), and cerebral circulation replenishment (CCR). Depending on age and status of the children with CP, PT was performed individually and the therapist usually chose the Bobath or Vojta methods, according to the primary manifestation of muscle strength and muscle tonus. 40 Treatment was conducted for 30–60 min per day. Based on fine motor impairment, CP children accepted individualized OT therapy for 30–60 min per day, to train their fine motor functions. LT included training for articulation, comprehension, performance and cognition; it was undertaken for 30 min per day. HO was used to ameliorate brain oxygen supply and was conducted for 60 min per day for a period of 10 days, followed by a 10-day treatment-free interval; this cycle was repeated for 3 months. HS was used to promote meridian and blood circulation, and was performed for 45 min per day. CM was used to benefit the blood circulation and was performed for 30–60 min per day. MM, MS and CCR were conducted using corresponding instruments for 30 min per day. They were used to provide improvements to the meridian and circulation, muscle strength and brain–blood circulation, respectively. After 3 months of CR, the GMFM, FMFM and revised GDS were re-evaluated and changes from baseline were calculated.
Statistical analyses
All statistical analyses were performed using the SPSS® statistical package, version 17.0 (SPSS Inc., Chicago, IL, USA) for Windows®. To enhance statistical power, GMFCS levels were stratified into three subgroups: G1: levels I–II; G2: level III; G3: levels IV–V. Similarly, the baseline intellectual impairments were stratified into three subgroups based on the DQ value: D1: borderline and mild disability; D2: moderate disability; D3: severe and profound disability. For statistical analysis of the effect of age at the start of CR on therapeutic efficacy, based on the age at initiation of CR therapy, subjects were divided into three age subgroups: A1: 4.6–6.0 months; A2: >6.0–12.0 months; A3: >12.0–22.3 months. Changes from baseline in the GMFM, FMFM and DQ scores in children with CP were calculated and presented as mean ± SD. The changes from baseline of the three scores were compared between different subgroups using one-way analysis of variance. A P-value < 0.05 was considered statistically significant.
To establish whether CR therapy had any effect on CP, it was not sufficient to consider just the mean differences; measuring the ‘effect size’ was needed, to determine the difference between treatment and baseline scores and to identify the extent of any variance. Cohen's d effect size was used to quantify the treatment effect, which is probably the most common ‘effect size’ measure due to its computational simplicity and intuitive benchmark. The empirical benchmarks of Cohen's d effect size for operationally defining small, medium and large effects are 0.2, 0.5 and 0.8, respectively. 41 As an experiment with insufficient power (because of the small number of samples) will not be able to validate negative results, to test whether an experiment has sufficient samples to unravel a true difference, given an effect size and threshold (usually 0.05 is used), the power of the sample size was computed by G*Power, with a bivariate normal model. 42 Generally, an experiment with power 0.8 would be considered as reasonable and acceptable.
The association between the changes from baseline in FMFM and GMFM was calculated by Pearson’s correlation coefficient (rPearson). The rPearson values defining small, medium and large correlations are 0.1, 0.3 and 0.5, respectively. 41
Results
Demographic and clinical characteristics of young children with cerebral palsy (CP; n = 48) who participated in a study to determine the effects of motor and intellectual functions on the effectiveness of comprehensive rehabilitation (CR).
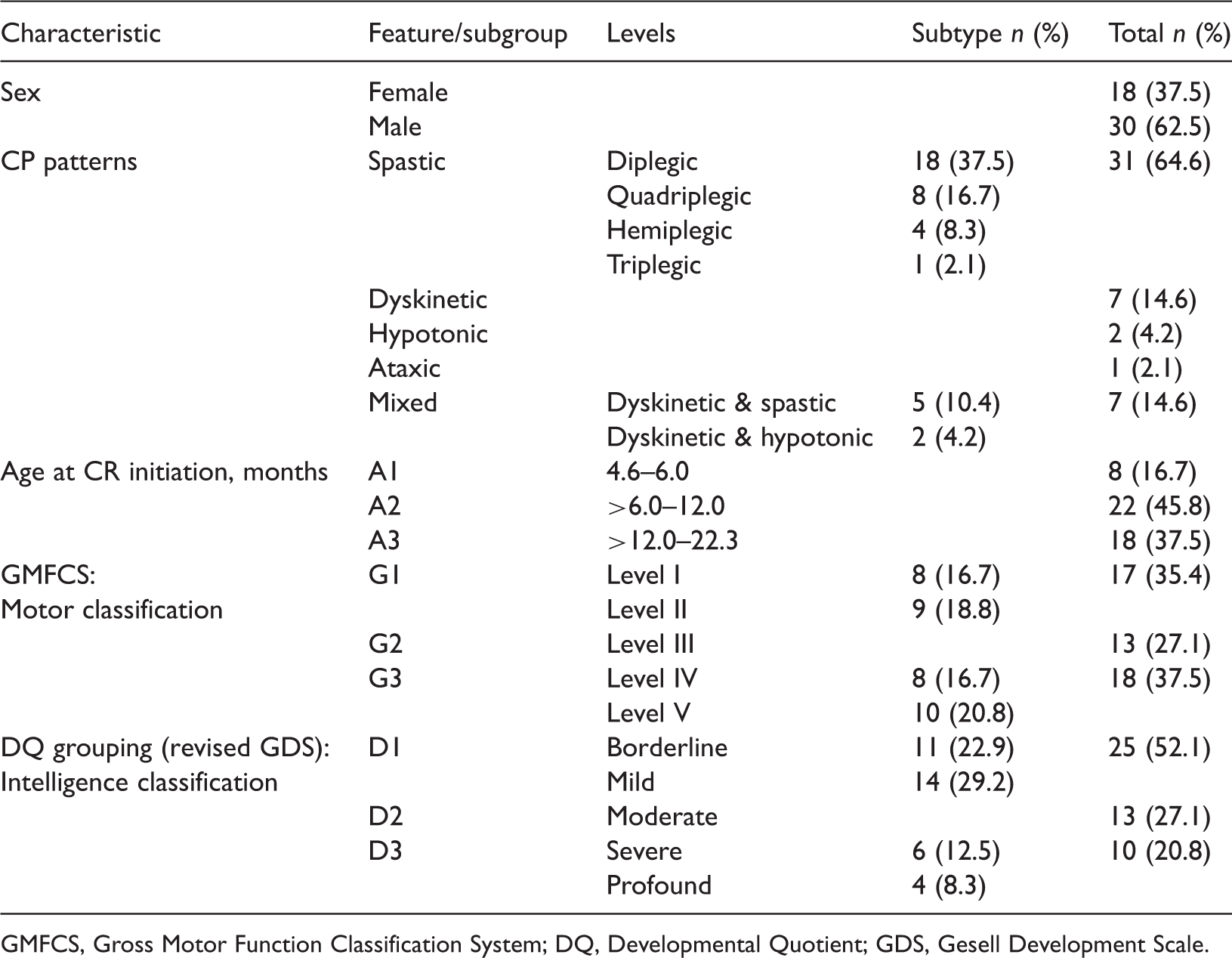
GMFCS, Gross Motor Function Classification System; DQ, Developmental Quotient; GDS, Gesell Development Scale.
Comparison of the mean change from baseline in the Gross Motor Function Measure (GMFM) and Fine Motor Function Measure (FMFM) scores after 3 months’ comprehensive rehabilitation therapy in young children with cerebral palsy, stratified according to baseline levels of intellectual impairment.
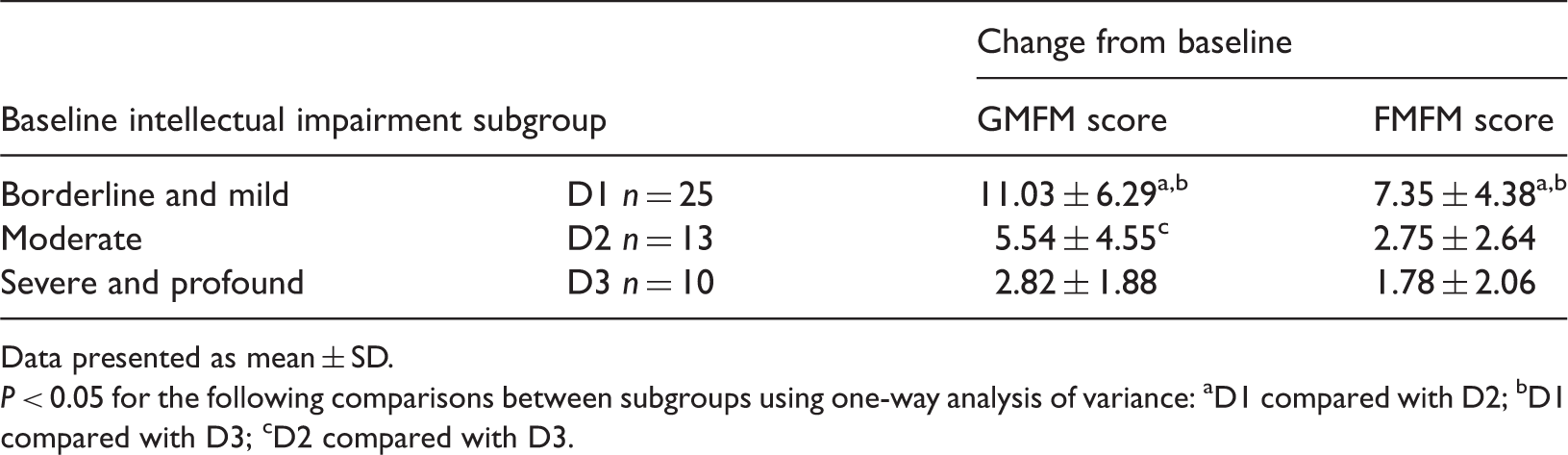
Data presented as mean ± SD.
P < 0.05 for the following comparisons between subgroups using one-way analysis of variance: aD1 compared with D2; bD1 compared with D3; cD2 compared with D3.
Cohen's d effect size analyses, undertaken to quantify the treatment effect on Gross Motor Function Measure (GMFM) and Fine Motor Function Measure (FMFM) scores after 3 months’ comprehensive rehabilitation therapy in young children with cerebral palsy, stratified according to baseline levels of intellectual impairment and G*Power calculations of sample size power for each group.
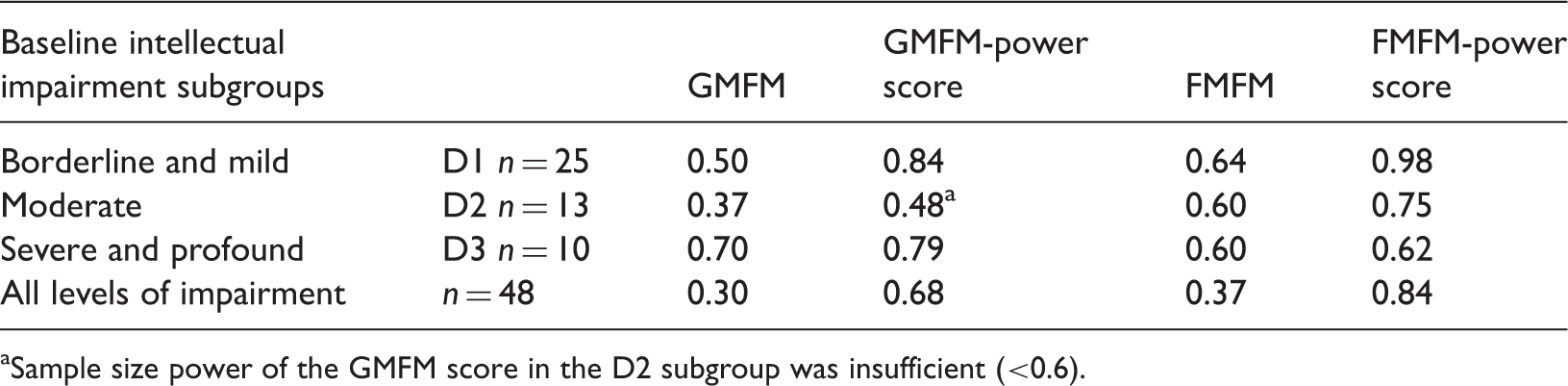
Sample size power of the GMFM score in the D2 subgroup was insufficient (<0.6).
Comparison of mean ± SD change from baseline in developmental quotient scores after 3 months’ comprehensive rehabilitation therapy in children with cerebral palsy, stratified according to baseline levels of gross motor impairment (measured using the Gross Motor Function Classification System).

P < 0.05 for the following comparisons between subgroups using one-way analysis of variance: aG1 compared with G2; bG1 compared with G3; cG2 compared with G3.
Association between baseline gross motor impairment level and intellectual impairment among young children with cerebral palsy (n = 48).

Data presented as n of patients.
GMFCS, Gross Motor Function Classification System; DQ, Developmental Quotient.
Comparison of the mean change from baseline in Gross Motor Function Measure (GMFM), Fine Motor Function Measure (FMFM) and Developmental Quotient (DQ) scores after 3 months’ comprehensive rehabilitation (CR) therapy among young children with cerebral palsy, stratified according to their age at therapy initiation.
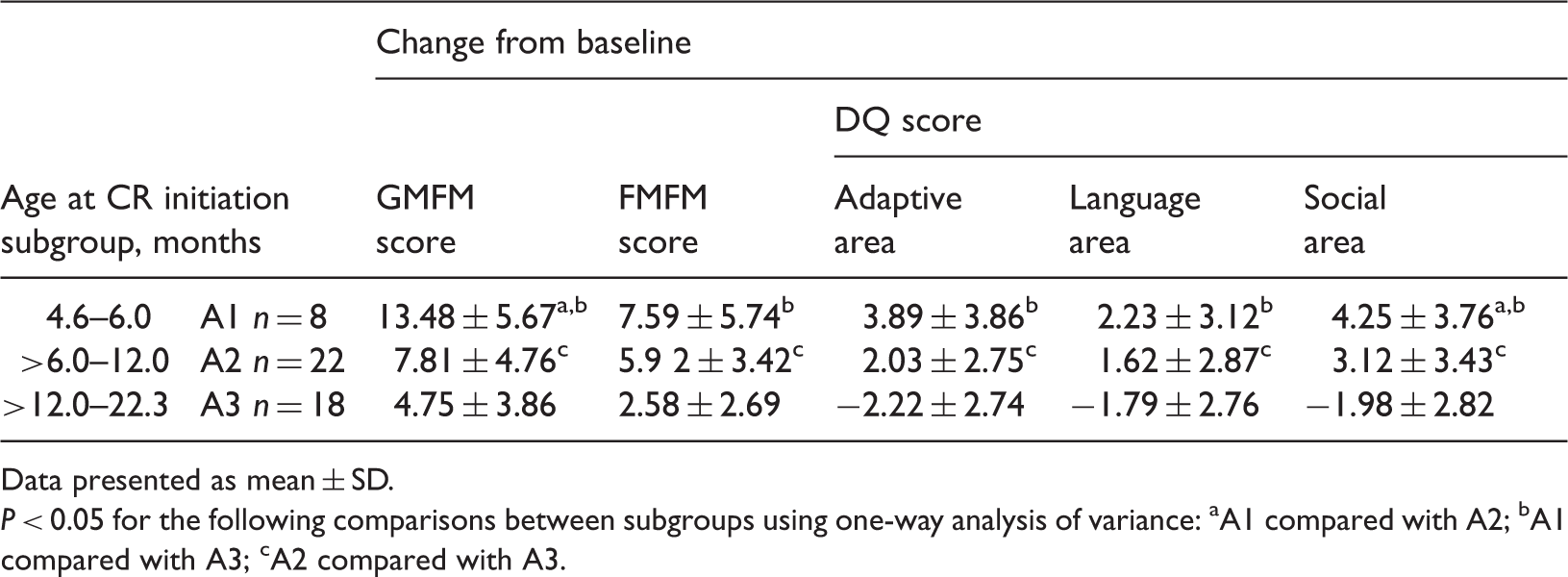
Data presented as mean ± SD.
P < 0.05 for the following comparisons between subgroups using one-way analysis of variance: aA1 compared with A2; bA1 compared with A3; cA2 compared with A3.
Discussion
Despite the progression of perinatology, the incidence of CP has not decreased. 43 CP not only affects motor function but also, in a high proportion of cases, it is accompanied by intellectual disability.7–9 Although it is well established that the level of motor impairment is positively correlated with the severity of intellectual disability,10,15,18,44,45 theories regarding the mechanisms of this phenomenon are lacking. Moreover, it is unclear if the level of motor impairment and intellectual disability in children with CP could influence each other, and in doing so subsequently affect the efficacy of clinical interventions.
Many assessment tools are available to test the severity of motor and intellectual impairment in children with CP. The GMFCS has been validated as a reliable instrument to classify the severity of gross motor dysfunction in CP cases across different age bands.2–4 In this present study, the cohort was aged <2 years, therefore, the criteria of the GMFCS for this age band were used. The GMFM is a reliable scale for the quantitative evaluation of gross motor function and is widely used to assess the effectiveness of interventions in children with CP.6,43 The FMFM scale was developed to assess the fine motor functions of young children with CP.33–35 As for intellectual evaluation, a revised GDS (covering adaptive, language and social areas) was used in this present study. The reliability, validity and responsiveness of the FMFM and GDS have been established in many studies, including some conducted in Chinese populations.2–5,11–13,33–39 Recently, the new version of the Bayley scales (Bayley III) has been used in some studies to measure neurodevelopment.27,46,47 Bayley III is an individually administered instrument designed to assess the developmental functioning of infants, toddlers and young children aged 1–42 months, which includes five domains: cognitive, language, motor, adaptive and social-emotional development. 27 However, Bayley III is prone to enlarge the severity of impairments, including the mental domains, and its reliability remains to be validated in clinical practice. 47 In the present study, the gross and fine motor impairments of children with CP were evaluated using the GMFM and FMFM scales, respectively; and the intellectual impairments were evaluated using the DQ score via the revised GDS.
In the past decade, various therapeutic interventions have been used for CP. These include physical, occupational, and speech therapy, deep brain stimulation, 21 and TCT; therapies are often used in combination with other medical management regimens.20,23–25 Consistent guidelines are lacking and the effectiveness of these therapeutic interventions remains to be validated in controlled trials. TCT has been demonstrated, to some degree, to benefit children with CP. 26 Appropriate interventions for CP are usually determined by the patient’s functional ability, severity of their impairments, pattern of motor disorder, associated pain and discomfort, and age. In this present study, CR including some items of TCT was the treatment intervention for children with CP. Data from the present study showed that children with a lower degree of motor and intellectual impairment (GMFCS levels I–II, combined with borderline and mild intellectual disability) at baseline present significantly greater improvements in FMFM, GMFM and DQ scores after 3 months’ CR therapy compared with the more severely impaired children. Both the FMFM and GMFM scores were positively correlated in children with CP, especially in the D1 subgroup.
When comparing improvements in the mean GMFM and FMFM scores among children with CP with different levels of intellectual disability at baseline, the present results demonstrated that after 3 months’ CR therapy, the improvement in motor function was positively correlated with the baseline level of intellectual function. To elucidate whether the CR therapy had any effect on CP, the variance should also be considered. The present data showed that the CR therapy had positive effects on GMFM and FMFM, especially for GMFM in the D1 and D3 subgroups, and for FMFM in all three subgroups (D1, D2, D3), although the treatment effects were not of very large magnitude when considered in the overall study cohort.
When comparing improvements in the mean DQ scores after 3 months’ CR therapy among children with different baseline GMFCS levels, the present results demonstrated that improvements in DQ scores also correlated positively with the baseline level of gross motor function. The present findings indicated that the improvement of motor impairment worked in parallel with intellectual disability to influence each other positively during CR therapy. A possible explanation for the relationship between gross motor function and intellectual level might be the requirement to be able to receive external stimuli from the environment via complex motor or intellectual activities. The lack of necessary sensory and motor stimuli during critical periods of brain development may lead to motor dysfunction and intellectual disability. 15 Exercise or training intervention during the brain’s developmental period is known to induce a cascade of molecular and cellular processes that support brain plasticity. 48 In this present cohort, children with less baseline gross motor impairment usually had higher baseline DQ scores. Moreover, the present study also found that the improvement of motor skills and intelligence was closely and reciprocally linked in children with CP during treatment. These present data indicated that children with CP with baseline gross motor impairments at GMFCS levels III–V might have limited self-mobility, due to severe motor impairment and a restricted ability to retrieve information from their environment. These present data may suggest that functional status related to ambulation is a powerful predictor for the potency of intellectual improvement, in children with CP. Meanwhile, cerebral lesions associated with intellectual disability are also useful for indicating the capacity for motor improvement. Therefore, these present findings suggest that it is critically important to evaluate motor function, combined with intellectual status, when developing suitable rehabilitation programmes for children with CP.
In children with CP, health-related quality-of-life is closely related to motor function and intellectual ability. Hence CP therapy should focus on the restoration of motor and intellectual function, especially with the goal of being able to live and work independently. It is well known that the early onset of long-term regular treatment is pivotal for children with CP, to obtain a desirable outcome. 49 It is particularly important to initiate treatment in early infancy when the brain is immature and exhibits significant plasticity, compensatory and recovery ability, as well as being when abnormal posture or movement have not been corrected. With treatment, children with mild CP may even recover to developmental levels close to those typical of their peers. 50 In contrast, with a lack of early treatment, many children with CP children may develop soft-tissue contracture, joint deformity and intellectual disability, which severely affect health-related quality-of-life. 51 However, the critical time for treatment intervention remains unclear. This present study compared the GMFM, FMFM, and DQ scores after 3 months’ CR therapy among subgroups of children with CP, stratified according to their age at treatment initiation. Improvements in scores were significantly greater in children with CP when CR was initiated before 12 months of age, indicating that early initiation of CR therapy was associated with greater therapeutic effectiveness. These findings were consistent with other studies examining the effectiveness of early intervention in children with CP.49,51–53
The present study had a number of limitations. First, the lack of a control group for comparison makes it impossible to take account of the effects of childhood maturation, but it was difficult to enrol healthy control children in this study. Secondly, the sample size was small (D2 subgroup: GMFM effect size = 0.37, GMFM-power = 0.48) and the observation period was short. A study with a larger sample size, conducted over a longer duration, is required in order to confirm these present findings. Thirdly, the present data demonstrated that it was difficult to obtain desirable intellectual improvements in children with serious baseline motor impairments. Accordingly, it was also difficult to gain functional motor improvements in children with severe baseline intellectual disability. Therefore, the reliability of these data might have been affected by these confounding factors.
In conclusion, data from the present study indicate that improvements observed in motor and intellectual function following 3 months’ CR therapy were closely correlated with each other, and with baseline levels of impairment, in children with CP. Therefore, these present findings suggest that it is critically important to take into account the baseline gross motor function, combined with intellectual status and age, when developing suitable comprehensive rehabilitation programmes for children with CP.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This work was supported by the National Nature and Science Foundation of China (no. 81171220) and (no. 31371125), the Paediatric Development Fund from the First Bethune Hospital of Jilin University, the Scientific Research Foundation for returned overseas Chinese scholars from State Education Ministry, the Science and Technology Innovation Project for returned overseas Chinese scholars from Human Resources and Social Security Development of Jilin Province, the Science Frontier and Interdisciplinary Innovation Project from Jilin University, and the Nature and Science Foundation (no. 201015147) from the Science and Technology Department of Jilin Province.