
Abstract
Objective
Aimed to investigate the effectiveness of body acupuncture on motor function of the upper limb in children with spastic hemiplegic cerebral palsy (CP) conjunction with rehabilitation program.
Design
The study is a randomized controlled experimental trial. Children with CP were randomly divided into the acupuncture group (body acupuncture with rehabilitation) and the rehabilitation group. The muscle volume difference between the upper limbs, the fine motor scores of the Peabody developmental motor scale-2 (PDMS-FM) and the surface electromyography (SEMG) parameter-root mean square (RMS)-on upper limb muscles (biceps brachii, radial wrist extensors and pronator teres) of both groups were measured before and after a 12-week treatment.
Results
37 children completed the study. In the two groups, differences in muscle volume, PDMS-FM scores and RMS values (biceps brachii, radial wrist extensors and pronator teres) were significantly improved, except PDMS-FM score difference and difference of RMS values (biceps brachii, radial wrist extensors and pronator teres) between the upper limbs in the rehabilitation group. Comparison post-treatment/pre-treatment change for two groups showed significant difference in affected upper limb PDMS-FM total score, PDMS-FM score difference between the upper limbs, affected upper limb RMS values and RMS value difference between the upper limbs in favor of the acupuncture group.
Conclusion
Our preliminary research indicates that body acupuncture therapy combined with rehabilitation may be more effective than rehabilitation alone, further improving muscle strength of affected upper limb and possibility of bimanual coordination in children with spastic hemiplegic CP.
Introduction
Cerebral palsy (CP) is a disorder of movement and postural control with most being diagnosed in the first year of life. The primary symptoms include spasticity (most common), dyskinesias (such as dystonia, athetosis, chorea), ataxia, hyper-reflexia, and in rare cases hypotonia. 1 Although high-income countries such as Australia have reported a decreasing incidence of CP, it remains the most common physical disability in childhood globally, and its prevalence ranges from 1.5 per 1000 to 4 per 1000.2,3 In China, the prevalence of CP is 1.25 per 1000 children of 0–17 years of age. 4
According to the data collected from Norway, spastic hemiplegic CP is the dominating subtype, accounting for up to 42.3%–53.7% of all cases of CP. 5 Children with hemiplegia have mainly grades I/II in the Gross Motor Function Classification System (GMFCS), classified in GMFCS I can walk without limitations, and GMFCS II walk with limitations which may include balance or endurance, use of a hand-held mobility device prior to age 4, use of a railing on stairs, or an inability to run or jump, 6 they possess relatively good walking ability, and their major sequela is dysfunction unilateral upper limb.7–9 Moreover, children with hemiplegia tend to use the unaffected upper limb more frequently during activities of daily living, which could lead to disuse and neglect of the affected upper limb, thus further aggravating the dysfunction of the affected limb and bimanual coordination.10,11 Therefore, improving the upper limb functions of children with spastic hemiplegic CP is crucial as it also improves their capabilities in activities of daily living and social communication, educational outcomes, and future job selection.
Substantive clinical trial data have supported the efficacy of training-based interventions, including hand-arm bimanual intensive therapy (HABIT),12,13 action observation training, constraint-induced movement therapy (CIMT), environmental enrichment, goal-directed training, home programs using goal-directed training, and occupational therapy after botulinum toxin injection. 2 There are also several adjunctive interventions that, when combined with task-specific motor training, may augment the positive effects of training, such as electrical stimulation and virtual reality serious gaming. Systematic reviews also have suggested the efficacy of acupuncture in children with CP. 2 The efficacy of acupuncture, as part of traditional Chinese medicine (TCM) used for the rehabilitation therapy of various conditions in China,14–16 has been validated in clinical trials, and there has been a substantial increase in the number of systematic reviews published.17–20 However, data on acupuncture for improving upper limb functions of children with spastic hemiplegic CP are scarce. Therefore, this pilot study aimed to investigate the clinical efficacy of body acupuncture for the rehabilitation therapy of the upper limb functions of children with spastic hemiplegic CP.
Patients and Methods
Study Design and Patients
The study was conducted as a randomized controlled experimental trial. Children with hemiplegic spastic cerebral palsy were selected from the pediatric rehabilitation outpatient clinic, from June 2023 to September 2023. The inclusion criteria were: 1) meeting the diagnostic and classification criteria for hemiplegic CP in the “Chinese rehabilitation guidelines for cerebral palsy (2022)” issued by the Chinese Association of Rehabilitation Medicine Pediatric Rehabilitation Committee; 2) age between 1–3 years; 3) Mini-Manual Ability Classification System (Mini-MACS) 21 level ranging from I to III; and 4) the parents or guardians signed the informed consent forms, and they could cooperate with evaluation and interventions in hospital, understand and execute the home exercise program. The exclusion criteria were: 1) joint and muscle fixed contracture or malformation; 2) uncontrolled epileptic seizure; 3) the affected upper limb had received botulinum toxin A injection within the past 6 months, or was scheduled to receive botulinum toxin A injection during the study period; 4) the affected upper limb had previously received orthopedic surgery; 5) the children had received prior acupuncture treatment; or 6) the child had visual or hearing or cognitive impairments that could affect the interventions and assessments for the rehabilitation.
The parents or guardians of all the included children signed the informed consent forms.
Grouping
The children were randomly divided into the acupuncture group and the rehabilitation group. Randomization was performed using a random number table prepared by a third-party statistician. Because of the nature of the interventions, the parents and investigators could not be blinded to treatments. Only the rehabilitation evaluator was blinded to grouping.
Interventions
All acupuncture sessions were conducted by the same experienced attending TCM physician. In brief, acupuncture was performed at the following major acupoints for the upper limb paralysis: Jianyu (LI 15), Binao (LI 14), Jianliao (TE14), Jianzhen (SI 9), Quchi (LI 11), Waiguan (TE 5), Neiguan (PC 6), and Hegu (LI 4). The assistant acupoints were: Jianjing (GB 21) and Tianzong (SI 11) for dysfunctions in shoulder adduction, Shouwuli (LI 13) and Shousanli (LI 10) for dysfunctions in elbow flexion, Yangxi (LI 5), Yanggu (SI 5), and Yangchi (TE 4) for carpoptosia, Sanjian (LI 3) and Houxi (SI 3) for dysfunctions in making a fist, and Yangxi (LI 5) for dysfunctions in thumb adduction (Table 1). The corresponding acupoints on the affected side were treated with acupuncture needles of 0.3 × 25 mm or 0.3 × 40 mm. The needles were perpendicularly inserted for 0.3 to 1.5 Cun (according to the depth of the corresponding acupoint), and manipulating the needle was allowed. According to the disease conditions, different manipulations, including reinforcing and reducing methods, were conducted. Static retaining of the needles or connecting 4–6 acupoints (4 major acupoints: Jianyu (LI 15), Quchi (LI 11), Waiguan (TE 5), Hegu (LI 4)), and 0–2 assistant acupoints for main dysfuntion) to a G-6905 multi-functional therapeutic instrument was performed as necessary. When the instrument was used, the acupoints were stimulated with moderate dilatational waves for 20 min, with a frequency tolerable to the children. The acupuncture therapy was conducted every other day for 3 consecutive weeks, which was considered as one cycle. There was a 1-week pause between each cycle, and the treatments were conducted for 3 cycles (12 weeks).
Acupuncture Acupoints in the Upper Limb.

Rehabilitation therapy was conducted by rehabilitation therapists with over 5 years of experience. The rehabilitation therapy protocols included traction and extension of the affected upper limb, strength training, and motor learning; and coordination training of the two hands and specific task training. Tasks were listed according to the children's abilities. Prior to the training, information was given to parents or caregivers on how to prevent compensatory behavior, such as performing a task with only the unaffected hand. Tasks were divided into full tasks and partial tasks. In full tasks, the unaffected hand was the hand that mainly completed the task, and the affected hand was the hand that assisted in completing the task. For example, in painting activities, it was necessary to place and stabilize the drawing paper with the affected hand, and draw on the paper with the unaffected hand. In partial tasks, some tasks were designed with symmetrical hand movements to trigger the target action, such as pick up a block of wood from the table with each hand and put it back into the box, the faster the better. All treatments were conducted at the hospital, once per day, 5 times per week, and 0.5–1 h each session. The therapists also taught the parents or caregivers to conduct home occupational therapy correctly. The children were asked to conduct the home occupational therapy for an additional 0.5–1 h every day after the hospital treatment as consolidation therapy. The treatments were conducted for 12 consecutive weeks. Electrostimulation was also conducted for the radial hand extensor muscle and extensor muscles of the fingers on the affected side once per day in addition to 0.5–1 h occupational therapy, 5 times per week, for 12 consecutive weeks, with 20 min each time. The parameters for the treatment were: frequency of 50 Hz, pulse width of 0.3 ms, current of 0–100 mA, and the ratio of power on/off time of 1:1, power-on time of 12 s, time for wave increase/wave decrease of 1 s, and power-off time of 12 s. The output intensity of the current was gradually adjusted to avoid the discomfort of the children. The current intensity was adjusted to the lowest current intensity that could induce evident contraction of the muscles in the children.
For the children in the rehabilitation group, rehabilitation therapy was conducted as above. For the children in the acupuncture group, both the acupuncture therapy and rehabilitation therapy were conducted as above, when both rehabilitation and acupuncture therapy were conducted at the same days, each rehabilitation therapy session followed by an acupuncture treatment. Side effects were observed in two hours after children finishing acupuncture therapy.
Assessments
All children were assessed by the same rehabilitation evaluator with over 3 years of experience before and after 12 weeks of therapy. For the assessment of the muscle volume difference between the unaffected and affected upper limbs, the maximal circumferences of the unaffected and affected forearms (the site with the largest bulging at the proximal forearm) were measured, and the difference was calculated. The fine motor scores of the Peabody developmental motor scale-2 (PDMS-FM)22,23 were used to measure the ability to grasp, use the hand, and hand–eye coordination. Operational flexibility was composed of grasping and visual–motor integration. The grasping points test comprised 26 projects, and the visual–motor integration points test comprised 72 projects. The score for each item ranged from 0 to 2, and therefore, the scores can be classified into three degrees for each item. The affected and unaffected upper limbs were assessed separately, then we get the affected upper limb PDMS-FM total scores, the unaffected upper limb PDMS-FM total scores, and the score difference between the two upper limbs were calculated (the unaffected upper limb PDMS-FM total scores- the affected upper limb PDMS-FM total scores).
The surface electromyography (SEMG) signals were collected by UMI-SE-I SEMG analysis feedback instrument at room temperature of 25°C, and disposable Ag-AgCL electrodes with diameter of 2 cm were used. The muscle to be tested was completely exposed in sitting position, and the local skin was wiped with 75% medical ethanol. The electrodes were placed at the fullness of the biceps brachii, radial wrist extensors and pronator teres and marked with marker pen. The distance between the two recording electrodes was 2 cm, paralleled to the long axis of the muscle fibers, and the SEMG signals of the corresponding muscle resistance were collected. During the test, the child should be encouraged to keep quiet, relax and cooperated as much as possible. The representative muscles such as biceps brachii (elbow flexion), radial wrist extensors (wrist extension), and pronator teres (elbow pronation) were selected as target muscles for testing. The SEMG parameter-root mean square (RMS)-value in the stationary signal segment was calculated as the represent of muscle strength. The increase in RMS values before and after treatment indicated an improvement in muscle strength. 24
Statistical Analysis
SPSS 20.0 (IBM, Armonk, NY, USA) was used for statistical analysis. The normality test was conducted for continuous data. Continuous data with a normal distribution are presented as means ± standard deviations and were analyzed using the student t-test and the paired t-test for comparison before and after treatment. Continuous data with a skewed distribution are described with medians (ranges) and were analyzed using the Mann–Whitney test for comparison between the two groups and the Wilcoxon test for comparison before and after treatment. P-values <0.05 were considered significant.
Results
Baseline Characteristics of the Patients
According to inclusion and exclusion criteria, 40 children were enrolled in the study, 20 in acupuncture group and 20 in rehabilitation group. However, two children in the acupuncture group and one child in the rehabilitation group did not complete the treatment duration. Finally, 37 children with spastic hemiplegic CP completed the study, who were grouped as follows: 19 in the rehabilitation group and 18 in the acupuncture group, Figure 1 presented the patient flowchart. During the study, we found that children older than 3 years mostly had received acupuncture before. In order to better observe the effect of acupuncture therapy, the mean age in our pilot study was 2.23 ± 0.50 years (range: 1 year to 2 years 11 months). Table 2 shows that the age, the differences in muscle volume, and PDMS-FM scores (unaffected upper limb total score, affected upper limb total score, and score difference between the upper limbs) were not significantly different among the groups at baseline (P > 0.05).
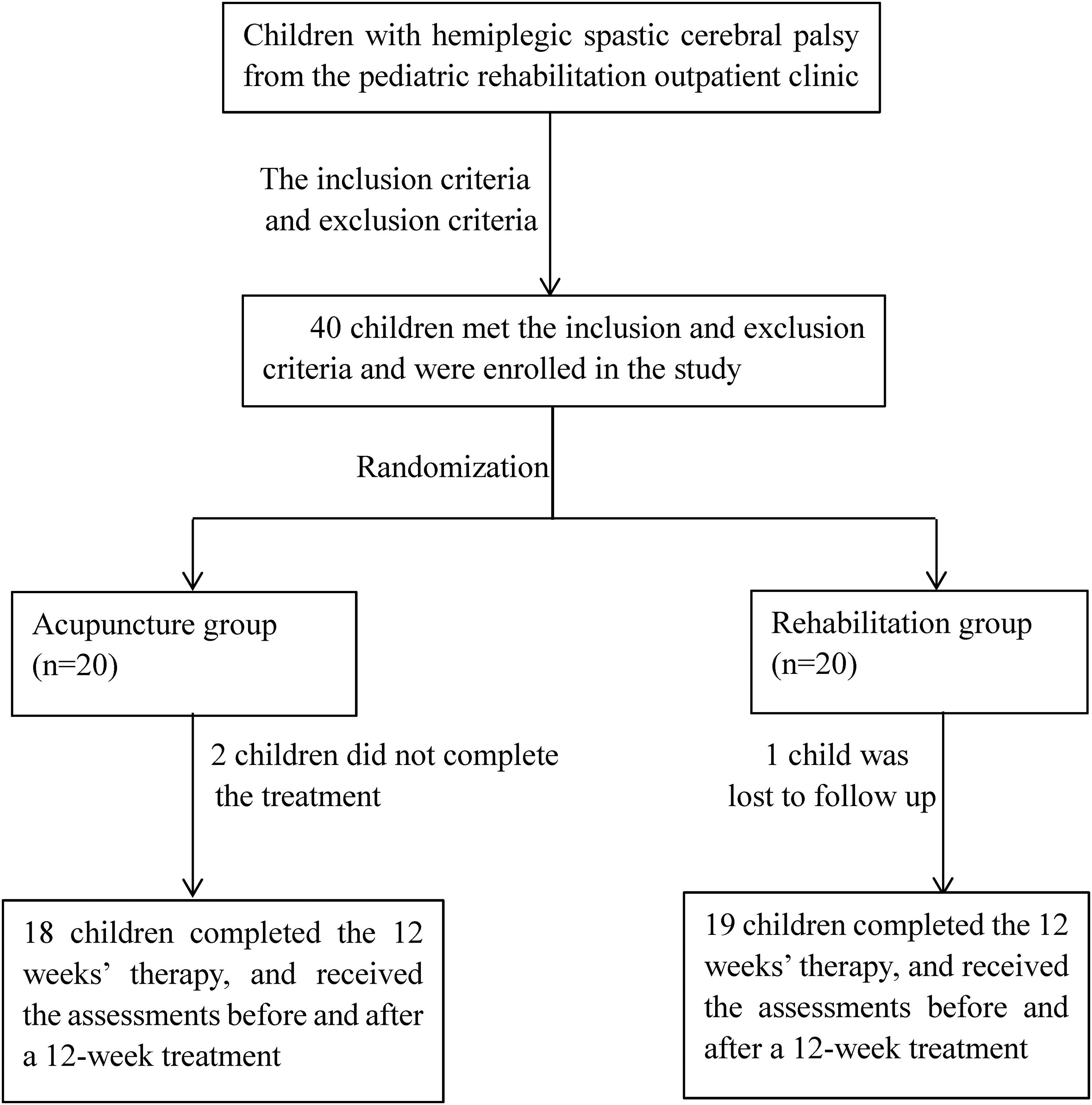
Patient flowchart.
Characteristics of the Patients.
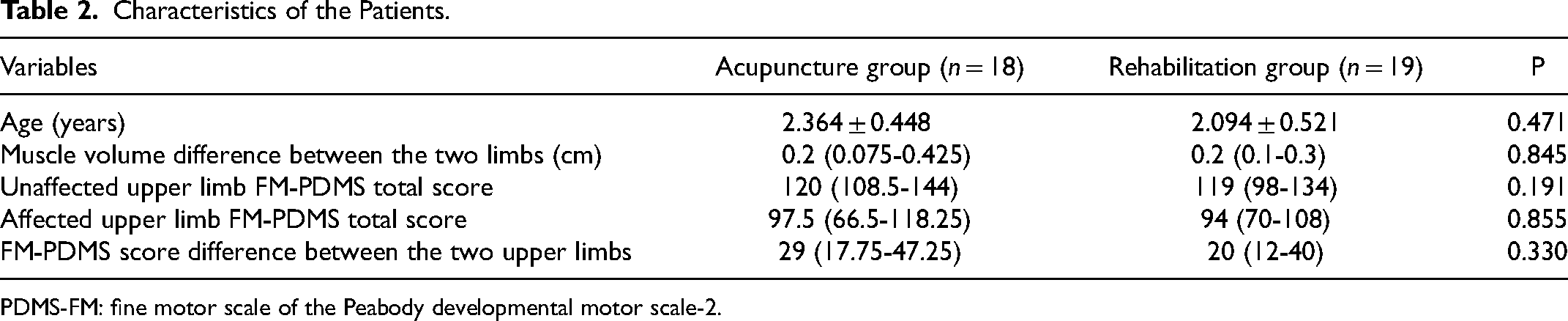
PDMS-FM: fine motor scale of the Peabody developmental motor scale-2.
Changes Before and After Treatment
Table 3 shows the differences in muscle volume, and PDMS-FM scores (unaffected upper limb total score, affected upper limb total score, and score difference between the upper limbs) in the groups before and after treatment. For the children in the acupuncture group, the differences in muscle volume (P = 0.030) and unaffected upper limb PDMS-FM total score (P < 0.001), affected upper limb PDMS-FM total score (P < 0.001), and PDMS-FM score difference between the two upper limbs (P < 0.001) improved significantly after treatment. For the children in the rehabilitation group the differences in muscle volume (P = 0.002), unaffected upper limb PDMS-FM total score (P = 0.001), and affected upper limb PDMS-FM total score (P = 0.001) improved significantly after treatment. The PDMS-FM score difference between the upper limbs in the rehabilitation group did not change significantly after the treatment (P = 0.058).
Comparison of the Parameters Before and After the Treatment Within the Same Groups.

PDMS-FM: fine motor scale of the Peabody developmental motor scale-2.
Table 4 shows the post-treatment/pre-treatment change in acupuncture group and rehabilitation group. In acupuncture group, the changes are positive except two cases of the muscle volume differences and one case of the PDMS-FM score difference between the upper limbs. While in rehabilitation group, the changes are not positive in one case of the muscle volume differences, one case of the unaffected upper limb PDMS-FM total score, two cases of the affected upper limb PDMS-FM total score and eight cases of the PDMS-FM score difference between the upper limbs. Compared rehabilitation group, the acupuncture group showed greater improvement in the affected upper limb PDMS-FM total score and PDMS-FM score difference between the upper limbs (P = 0.001 and P = 0.000, respectively).
Comparison of the Post-Treatment/pre-Treatment Change Between the Two Groups.

PDMS-FM: fine motor scale of the Peabody developmental motor scale-2; N: the number cases in which the post-treatment/pre-treatment change is positive and the percent; P: comparison of the post-treatment/pre-treatment change between the two groups.
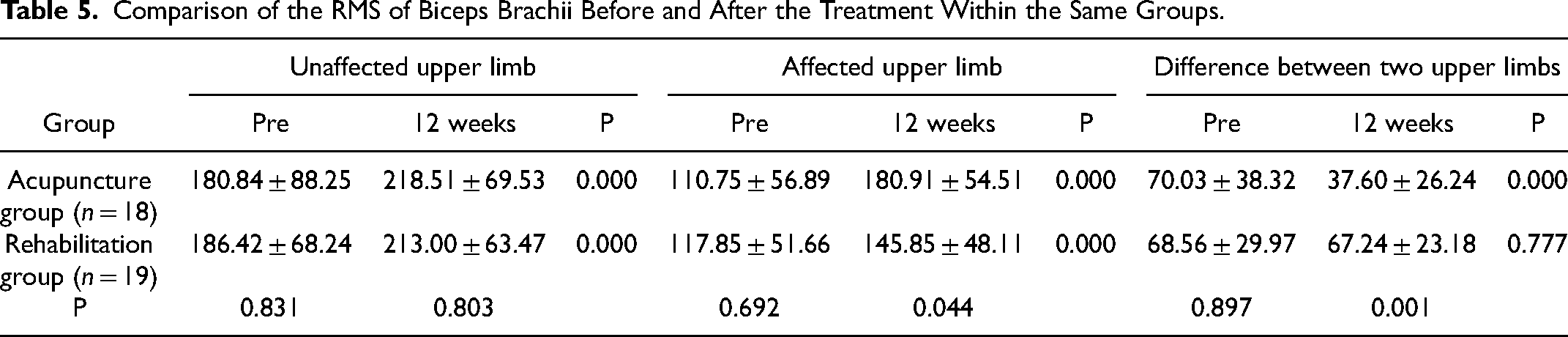
Tables 5–7 shows the RMS value of biceps brachii, radial wrist extensors and pronator teres (unaffected upper limb, affected upper limb, and difference between the upper limbs) in the groups before and after treatment. For the children in the acupuncture group, the RMS value of biceps brachii, radial wrist extensors and pronator teres in affected and unaffected upper limb (all P < 0.001) and difference between the two upper limbs (P = 0.000, P = 0.006, P = 0.036) improved significantly after treatment. For the children in the rehabilitation group the RMS value of biceps brachii, radial wrist extensors and pronator teres in affected and unaffected upper limb (all P < 0.001) improved significantly after treatment. The difference RMS value of biceps brachii, radial wrist extensors and pronator teres between the upper limbs in the rehabilitation group did not change significantly after the treatment (P = 0.777, P = 0.445, P = 0.085).
Comparison of the RMS of Biceps Brachii Before and After the Treatment Within the Same Groups.
Comparison of the RMS of Radial Wrist Extensors Before and After the Treatment Within the Same Groups.

Comparison of the RMS of Pronator teres Before and After the Treatment Within the Same Groups.

Our findings showed the improvement of RMS values on muscles of biceps brachii, radial wrist extensors and pronator teres and PDMS-FM score in the affected upper limb was significant both in acupuncture group and rehabilitation group, and the acupuncture group improved more than rehabilitation group significantly, especially narrowed the gap between the affected upper limb and the unaffected upper limb.
No side effects were observed in any of the children throughout the study period.
Discussion
The similar characteristic features of the patients in both groups showed that the children in the experimental and control groups had similar descriptive characteristics, which increased the reliability of the research by reducing bias. In this study, homogeneity was ensured between the groups and the results of the research were not affected. Our findings indicated that rehabilitation significantly improved muscle volume, PDMS-FM score and RMS value of both the affected and unaffected upper limbs in children with spastic hemiplegic CP. When combined with acupuncture therapy, it could better improve the affected upper limb PDMS-FM total score, RMS value, PDMS-FM score difference and RMS value difference between the upper limbs. Thus, body acupuncture may augment the positive effects of training, and it is an effective adjunctive intervention when combined with rehabilitation therapy.
Children with spastic hemiplegic CP are generally capable of studying in regular schools with their peers, 5 although their upper limb dysfunctions severely influence their daily lives and study activities.7–9 Therefore, rehabilitation of the upper limb functions of children with spastic hemiplegia has very important clinical significance. Several rehabilitation therapies, including HABIT, CIMT, and goal-directed training have been acknowledged as effective treatment methods.2,12,13,25 Thus, combined application of several rehabilitation methods could effectively improve the upper limb functions of children with spastic hemiplegic CP. This multi-modal therapy uses the advantages of multiple methods that have been shown to benefit children with CP, and each method may complement the limitations of the other methods.
Integrated TCM and Western medicine is the trend and a new field for the exploration of the rehabilitation therapies for children with CP in China. TCM categorizes CP in children into three groups: “Wuchi (five delays),” “Wuruan (five softs),” and “Wuying (five hards).” Wuchi refers to retardation of development of children (delay for standing, walking, speaking, growing hair and teeth), Wuruan refers to poor muscle strength (head, mouth, upper limbs, lower limbs and trunk), and Wuying describes the symptoms of spasticity caused by hypertonia (head, mouth, upper limbs, lower limbs and trunk). According to the clinical manifestations of increased muscle tone and poor muscle strength, spastic hemiplegia belongs to “Wuying” and “Wuruan”, both of which are impotence. TCM theories have suggested that this disease is caused by a congenital deficiency of qi and blood, bone marrow pool insufficiency, poor blood flow, and blood stasis obstructing the collaterals. For treatment, the TCM theories have suggested the principles of vitality recuperation, power and marrow nourishment, stasis removal, and dredging the collaterals.26,27 Acupuncture abides by the concept of comprehensive treatment and obeys the principle of syndrome differentiation and treatment. The treatment considers the meridians, organs, and the meridians and acupuncture points, then the acupoints are selected according to the channels, and distant or adjacent acupoints could be selected. Then, the acupoints are acupunctured to dredge the channels, regulate, and protect the qi and blood. 28 Previous studies have reported that acupuncture therapy alone and/or in combination with rehabilitation motor therapy could effectively improve the manual functions of children with CP, as reviewed by Li et al. 17 Modern medicine has proposed the fascial network throughout the human body is the anatomical basis for the acupoints and meridians of TCM. In fascial anatomy, human body is divided into the supporting-storing system of undifferentiated non-specific connective tissues and the differentiated functional system. The histological composition of meridians is non-specific connective tissues and acupoints are those sites that produce strong biological reactions when stimulated. Acupuncture promotes undifferentiated cells into functional cells by stimulating acupoints on meridians. 29
SEMG is a practical and effective assessment tool for measuring muscle activity and can be used during dynamic exercise. RMS values as SEMG parameters could represent overall muscle strength and muscle mass in individuals. 24 Fine motor scale of the PDMS-FM22,23 assessed children's level of participation in daily and social activities. Here, modern examination methods were used to assess differences of muscle volume and unaffected upper limb PDMS-FM score, affected upper limb PDMS-FM score and PDMS-FM score difference between the upper limbs, unaffected upper limb RMS value, affected upper limb RMS value and RMS value difference between the upper limbs which to some extent assessed the treatment effectiveness of acupuncture therapy for spastic hemiplegia in children with CP. The findings suggest that the treatment efficacy was more pronounced in the group where acupuncture and rehabilitation were combined in terms of improving the affected upper limb PDMS-FM score, RMS value and reducing the PDMS-FM score and RMS value difference between the upper limbs. By the concept of comprehensive treatment, acupuncture combined with rehabilitation narrowed the manual ability gap between the affected and unaffected upper limbs and improved possibility of their bimanual coordination, meeting the greatest rehabilitation needs for children with spastic hemiplegic-bilateral coordination. 30
This study has some limitations. Hemiplegic cerebral palsy can cause abnormal muscle tone. Tools that are more sensitive to changes in spasticity are required to verify the effect of acupuncture on muscle tone. The treatment lasting for 12 weeks, the assessment was performed only twice (before and after). It is worth considering to add one more assessment during the whole treatment period.
Conclusion
Nevertheless, our pilot study design was effective, 92.5% of participants completed the program, and we were able to maintain high fidelity to our design. Additionally, our findings suggest that acupuncture therapy combined with rehabilitation is effective in improving the muscle volume、PDMS-FM score and RMS value of the upper limbs of children with spastic hemiplegic CP. Compared with only rehabilitation intervention, rehabilitation combined with acupuncture therapy could better reduce the difference of manual ability between the affected and unaffected upper limb, improving possibility of bimanual coordination. Therefore, acupuncture combined with rehabilitation training can be considered an effective clinical rehabilitation program for children with hemiplegia. Our pilot study provides useful information for the application of acupuncture in the rehabilitation of the upper limb functions of children with spastic hemiplegic CP. Further research is also suggested with larger sample size and more accurate measurement.
Footnotes
Acknowledgments
We thank all the doctors, therapists, nurses, and other staff members at the Department of Rehabilitation, Children's Hospital, Zhejiang University School of Medicine for their cooperation in this study.
Author Contributions
Hui Wang: Writing – original draft, Writing – review & editing, Project administration, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. Yu Du, Zheng-huan Mao, Li Ding, and Jia-yu Xu: Writing – review & editing, Methodology, Investigation, Formal analysis, Data curation. Tong Chen and Wen-cong Ruan: Writing – review & editing, Review and supervising the part of traditional Chinese medicine, Data curation. Hai-feng Li: Writing – review & editing, Supervising the analysis of study data.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Ethics Committee of the Children's Hospital of Zhejiang University School of Medicine (2023-IRB-0163-P-01). The clinical trial number was ChiCTR2300073184.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Foundation of Science and Technology Program of Zhejiang Traditional Chinese Medicine Administration [2016ZB076].