
Abstract
Introduction:
Children and adolescents with cerebral palsy (CP) demonstrate proficient function if they can perform all tasks required for daily living. Telerehabilitation (TR) and monitoring can facilitate the execution of home-based (HB) therapies. This systematic review aimed to assess the scientific evidence regarding the effects of TR-monitored HB therapies on outcomes related to upper extremity function in children and adolescents with unilateral cerebral palsy (UCP).
Methods
Comprehensive searches were conducted across online databases, including the Cochrane Library, EMBASE, PubMed, Web of Science, and PEDro, as well as additional sources, from inception to October 2025. The inclusion criteria encompassed randomized controlled trials, whose risk of bias and methodological quality were evaluated using the Cochrane Risk-of-Bias Tool and the PEDro scale, respectively. A narrative synthesis approach was employed for data analysis.
Results
TR-monitored HB therapies showed positive improvements in hand coordination, dexterity, bimanual hand function, ADL motor and processing skills, occupational performance, and execution of functional goals in children and adolescents with UCP (predominantly spastic UCP studies) compared with the control interventions.
Conclusions
Telerehabilitation-monitored HB therapies showed potential to improve upper extremity function-related outcomes in children and adolescents with unilateral cerebral palsy (predominantly spastic UCP studies).
Keywords
Introduction
Spastic hemiparetic cerebral palsy (CP) primarily occurs due to unilateral injury to the motor cortex and/or pyramidal tract, causing hypertonia in certain antagonist muscles contralateral to the injury. 1 Unilateral spastic CP occurs due to damage to one brain hemisphere, causing functional impairments with spasticity in the flexor muscles, range of motion limitations, and low muscular strength. 2 Diminished upper extremity (UE) movements due to spasticity, weakness, and lack of selective muscle activation affect numerous children with CP, and these impairments with sensory deficits restrict synchronized and smooth movements needed for activities of daily living (ADL). 3 Upper extremity impairments impair function and restrict motor independence in ADL. 4 Sensory and motor impairments contribute to the functional limitations of the affected UE in children with unilateral spastic CP, with unimanual ability determined by these limitations and impaired unimanual ability affecting bimanual performance. 2
Traditionally, UE management focused on decreasing motor impairments and enhancing the quality of movement in children with unilateral CP. 5 Throughout the years, the model has transformed from an isolated therapy for impairments, such as spasticity and strength, to methods focusing on enhancing ADL and motor function. 6 Recent advances in computer technology have enabled the online administration and monitoring of training, permitting therapist-participant interaction, which gives participants the feeling of having a personal instructor. 7 Technological developments provide an option to paper-based home programs in the form of applications and websites for online exercise prescription. 8
Numerous healthcare professionals widely utilize telerehabilitation as part of a multidisciplinary team. 9 Telerehabilitation is defined as the use of information and communication technologies to deliver rehabilitation services. 10 Despite its importance, complying with exercise is difficult as individuals are unable to attend a gym or clinic for exercise; thus, studies on tele-exercise interventions using direct or indirect supervision have produced results comparable to in-person, clinic-based interventions. 11 Physical exercise can be conducted in different settings, such as gyms, rehabilitation centers, home, or public parks. 12 Under conditions of impaired mobility that might hamper participation in exercise programs, individuals may perform the exercise at home. 11 Moreover, teaching exercises at home may be easier, as it provides an opportunity to establish where the exercise can be safely performed with resultant higher confidence and thus more demanding exercise. 13
Given the aforementioned context and to the best of our knowledge, no systematic review has examined the effects of TR-monitored HB therapies on UE function-related outcomes in children and adolescents with UCP. Therefore, this systematic review aimed to assess the scientific evidence regarding the effects of TR-monitored HB therapies on UE function-related outcomes in this population.
Methodology
This review has the PROSPERO Registration number CRD420251045310. The review was conducted using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist. The PICOS framework was applied to develop the research question: what are the effects of TR-monitored HB therapies (I = intervention) on UE function (O = outcome) in children and adolescents with UCP (P = population) compared with standard, conventional, usual, or other therapies (C = comparison) in randomized controlled trials (RCTs) (S = study design)? The search procedure, appraisal of methodological quality, study selection, evaluation of risk of bias, and data extraction were conducted as outlined in our previous reviews,14–16 with adjustments to the databases searched, the dates of the searches, the search strategy, the selection criteria, and the data extracted to align with the objectives of this review.
Search strategy
Comprehensive searches were performed across online databases, including the Cochrane Library, EMBASE, PubMed, Web of Science, and PEDro, covering the period from their inception until October 2025. Utilizing the PICOS framework, the search methodology was designed to align with the specific requirements of each database. Detailed information on the search methodology is provided in Supplementary Material 1. A comprehensive manual literature search was conducted, encompassing searches through various search engines, citation searches and cross-referencing. This included examining the reference lists of the identified studies and employing forward citation tracking. Following the export of the identified studies to Endnote Reference Manager and the subsequent removal of duplicates, the remaining studies underwent additional screening. The search was independently conducted by one author (JSU) and subsequently validated by the other two authors (TWLW and SSMN).
Selection criteria
The review involved studies that met the following inclusion criteria: studies (i) involving children and adolescents with unilateral/hemiplegic CP (UCP), (ii) describing the effects of TR-monitored HB therapies, including HB therapies with remote components such as telephone support/follow-up (iii) conducted in humans and published in peer-reviewed journals in English, and (iv) with an RCT design and accessible full text. The exclusion criteria were as follows:
Abstracts of theses, conference papers, review studies, and unpublished works. Studies involving interventions administered solely in clinical or hospital environments. Studies without any telerehabilitation component, such as the use of technology, remote/tele monitoring/supervision, remote/tele coaching, remote/tele support, remote feedback, or telecommunication. Studies that included a mixed population (cerebral palsy and other conditions) without separate data on the cerebral palsy population.
Eligibility assessment and data abstraction
After duplicate records were eliminated, two authors (JSU and TWLW) independently evaluated the titles and abstracts of the studies. During the screening process, the review eligibility criteria were applied, and any disagreements between the two authors regarding the inclusion of a study were resolved through consultation with a third author (SSMN). In the course of the full-text screening phase, the complete texts of studies deemed eligible were retained, and the following pertinent information was systematically extracted from these studies: author, year of publication, design, sample size, sex and age, types of UCP, population, clinical characteristics of the population, intervention(s) groups and treatment protocol, telerehabilitation components involved, type of technology involved, details of monitoring/delivery, outcomes, assessment period, adverse events, results, and conclusions. The extracted data and characteristics of the eligible studies were entered into a Microsoft Excel spreadsheet.
Methodological quality appraisal and evaluation risk of bias
The methodological quality (MQ) of the eligible studies was assessed using the PEDro scale. The scale comprise of 11-itmes designed to evaluate the MQ of the studies. 17 The 11 items encompass the internal validity of the study and statistical reporting. Notably, the first item on the eligibility criteria was excluded from the computation of the overall score. 18 Each of the ten internal validity items was assigned a score of 1 or 0, indicating the presence or absence of the item. 18 The overall score was categorized into four quality levels: excellent (9–10), good (6–8), fair (4–5), and poor (0–3).19,20
The Cochrane ROB tool was utilised to determine the risk of bias (ROB) in the eligible studies. Three evaluative decisions categorized as unclear, high, or low were applied to evaluate the ROB for particular items across the domains of attrition, reporting, performance, blinding, selection, detection, and other biases. 21 Two authors (JSU and TWLW) independently performed these assessments. Any discrepancies were addressed by seeking input from the third author (SSMN).
Synthesis and analysis
The extracted data were analysed using narrative synthesis. The risk of bias (ROB), methodological quality (MQ), findings, and characteristics of the eligible studies were summarized descriptively.
Results
Study selection
A total of 420 pertinent records were retrieved from the databases and additional source searches. After removing 76 duplicate records, 344 records remained. A total of 292 records were disqualified for failing to meet the eligibility requirements in the course of title and abstract screening. Subsequently, the full texts of the remaining 52 reports were retrieved and evaluated in accordance with the review eligibility criteria. The review involved nine studies comprising ten reports. All included studies were RCTs employing a parallel design. Figure 1 presents the methodology for study selection, guided by PRISMA guidelines.
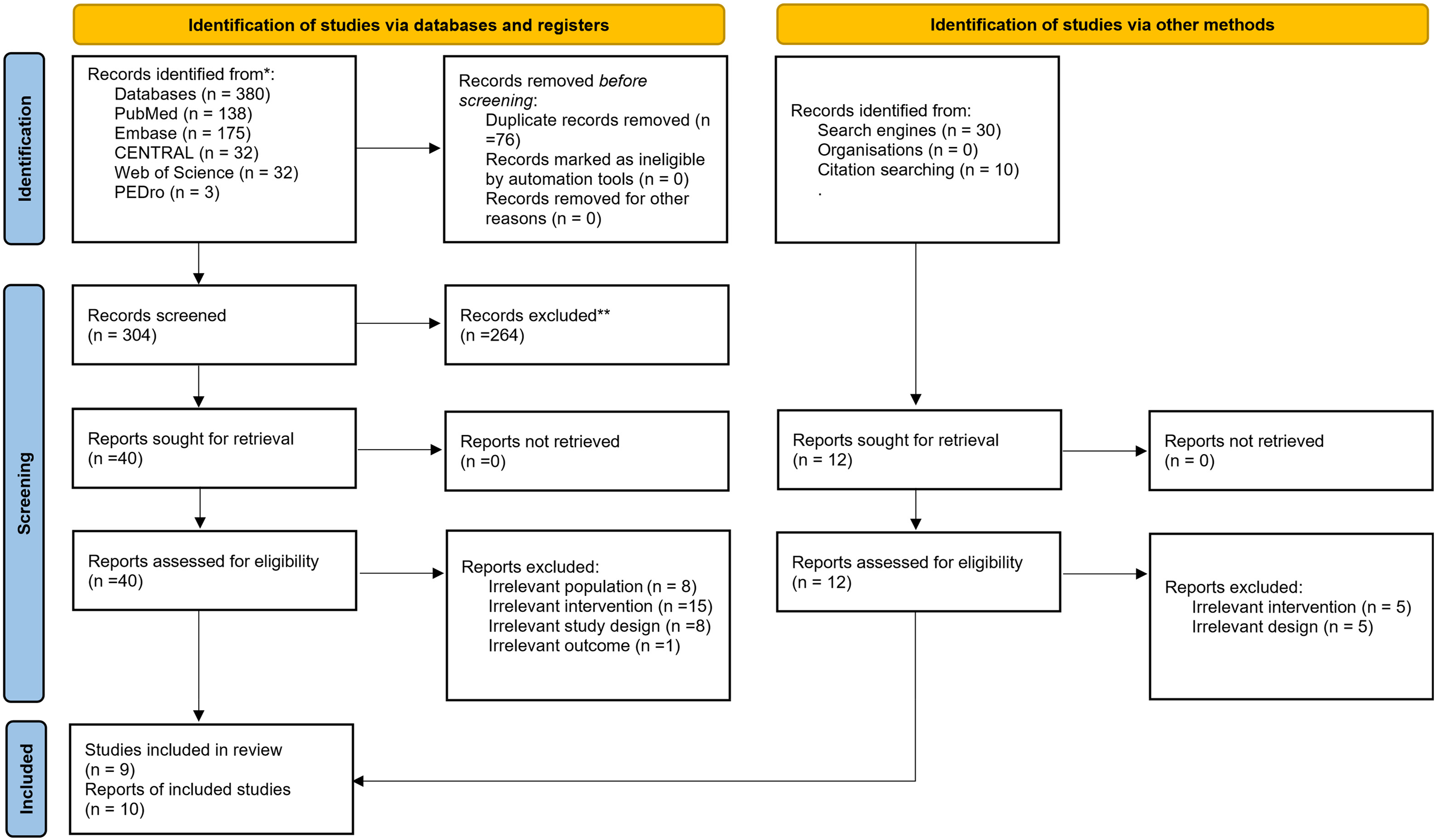
PRISMA 2020 flowchart
MQ assessment
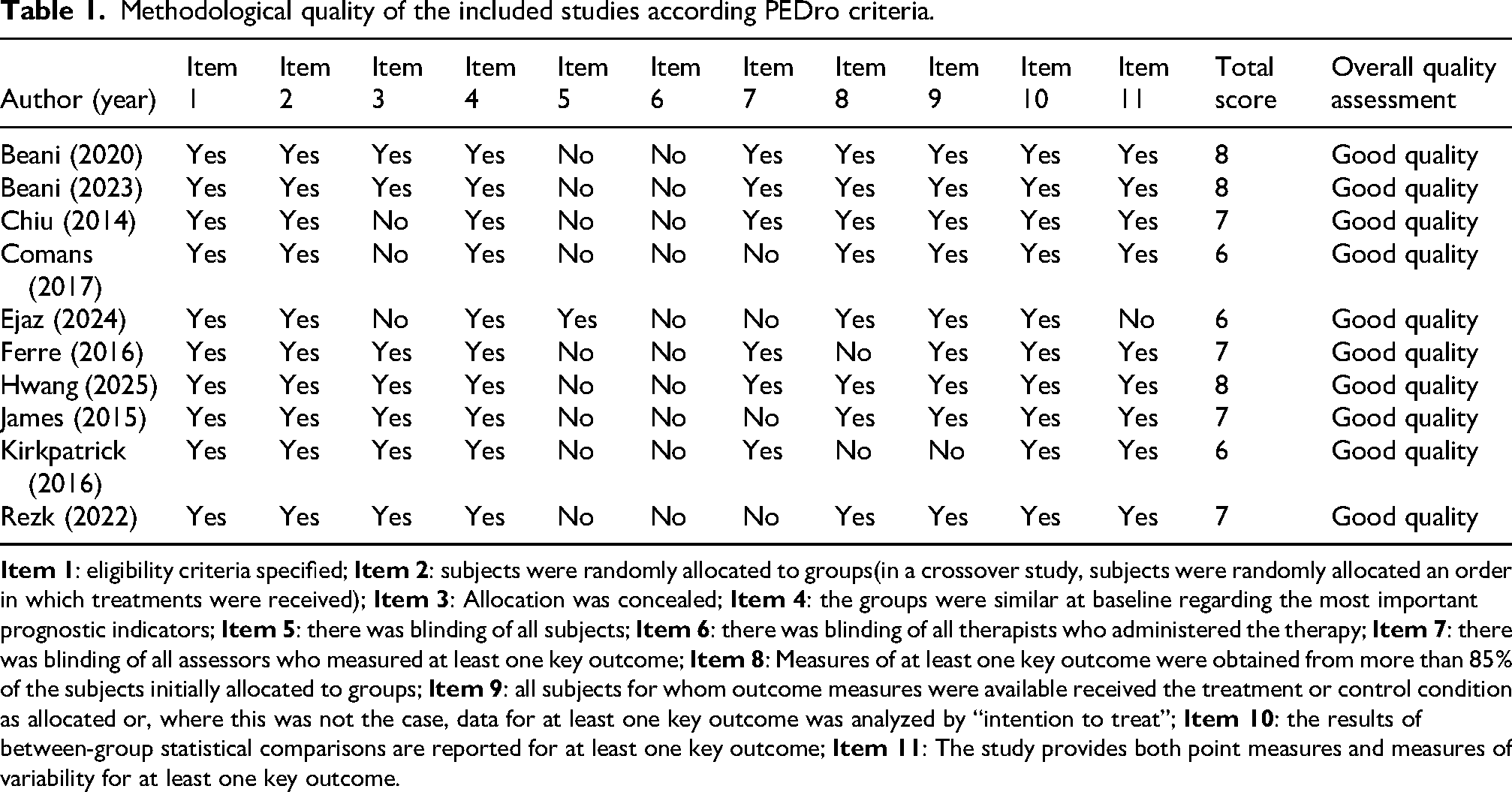
All of the included studies had a good MQ. In all studies included in the analysis of the PEDro scale domains, the following elements were consistently present: specification of eligibility criteria, random allocation, baseline similarity among groups concerning key prognostic indicators, absence of experimenter blinding, and description of between-group comparisons. The majority of the studies demonstrated allocation concealment, lacked participant blinding, included outcome assessor blinding, measured main outcomes for most participants originally allocated to groups, ensured that all subjects for whom outcome measures were available received the treatment or control condition as allocated, and provided point measures and measures of variability for main outcomes. Table 1 presents a detailed account of the methodological quality of the studies.
Methodological quality of the included studies according PEDro criteria.
ROB assessment
All studies exhibited a low risk of bias (ROB) in other bias, reporting bias, and attrition bias domains. Most studies demonstrated a low ROB for allocation concealment (selection bias), random sequence generation (selection bias), and detection bias. However, nearly all studies showed a high ROB in performance bias. Figures 2A and 2B present detailed information on the ROB in the included studies.
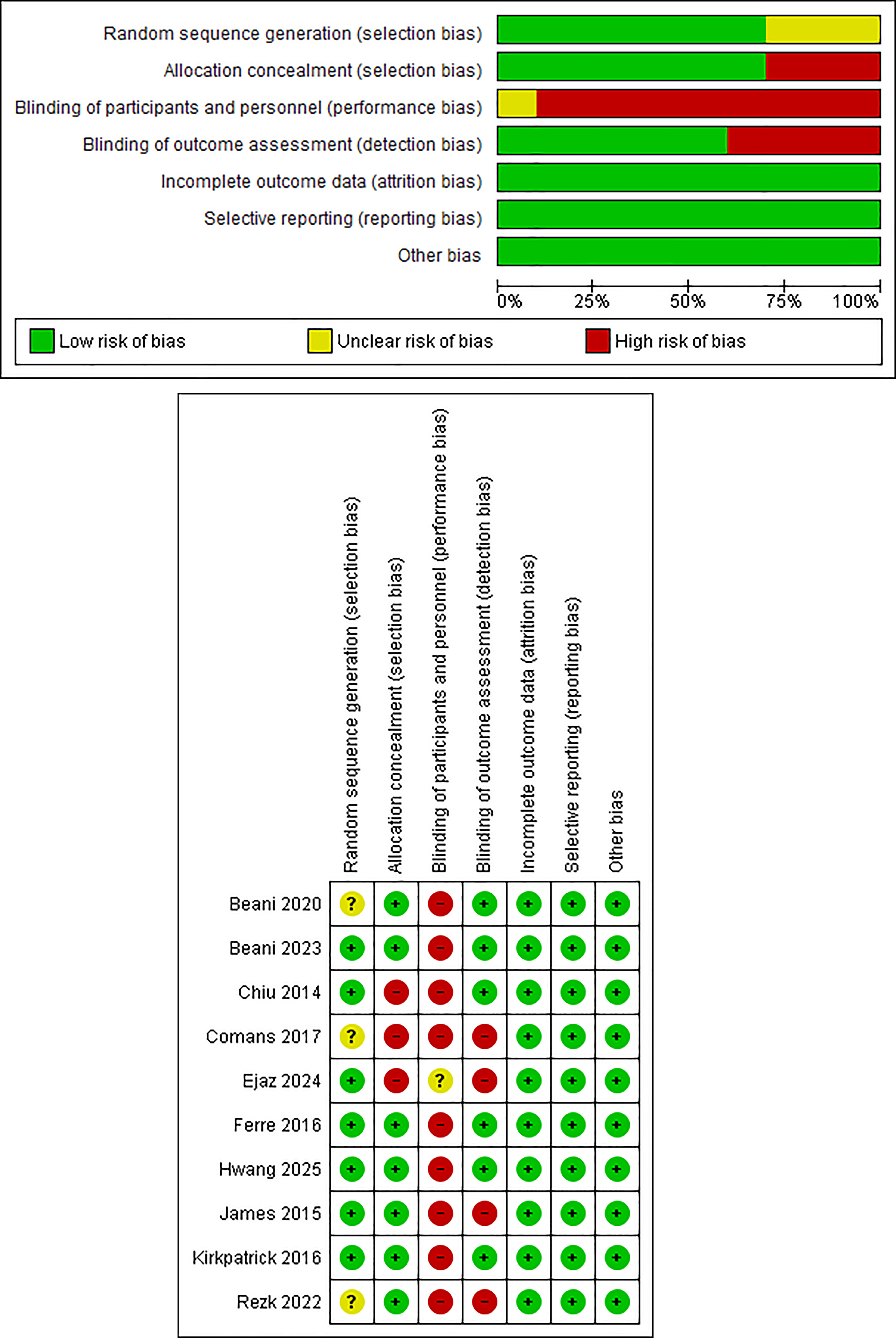
A. Risk of bias graph. B. Risk of bias summary.
Study characteristics
In total, 481 children and adolescents with UCP participated in the included studies, with an overall mean age ranging from 4.83 to 12.1 years. All studies used a parallel RCT design. Seven studies reported the affected side,22–28 and three reported GMFCS levels.23,24,26 Five studies reported MACS.23,24,26,28,29 However, HFCS has been reported in a few studies. In the majority of the studies, the participants were children and adolescents with spastic UCP (seven out of nine studies explicitly stated this, while one study implied it), and one study did not specify the type of UCP involved. UCP and home-based therapies/training were reported in all the studies. In terms of the types of therapies/training, one study each administered Wii Sports Resort™ training 26 and modified constraint-induced movement therapy. 30 Two studies applied a web-based multimodal therapy program (MitiiTM therapy),23,29 while three reports each used action observation training (AOT)22,25,27 and bimanual training/therapy.24,28,31 The studies described various telerehabilitation components, technologies, and monitoring methods used. Regarding outcome assessment, all included studies conducted before and after intervention outcome assessments, with some including follow-up assessments. Information regarding adverse events associated with the studies was also reported. Table 2 presents the detailed characteristics of the included studies.
Characteristics of included studies.
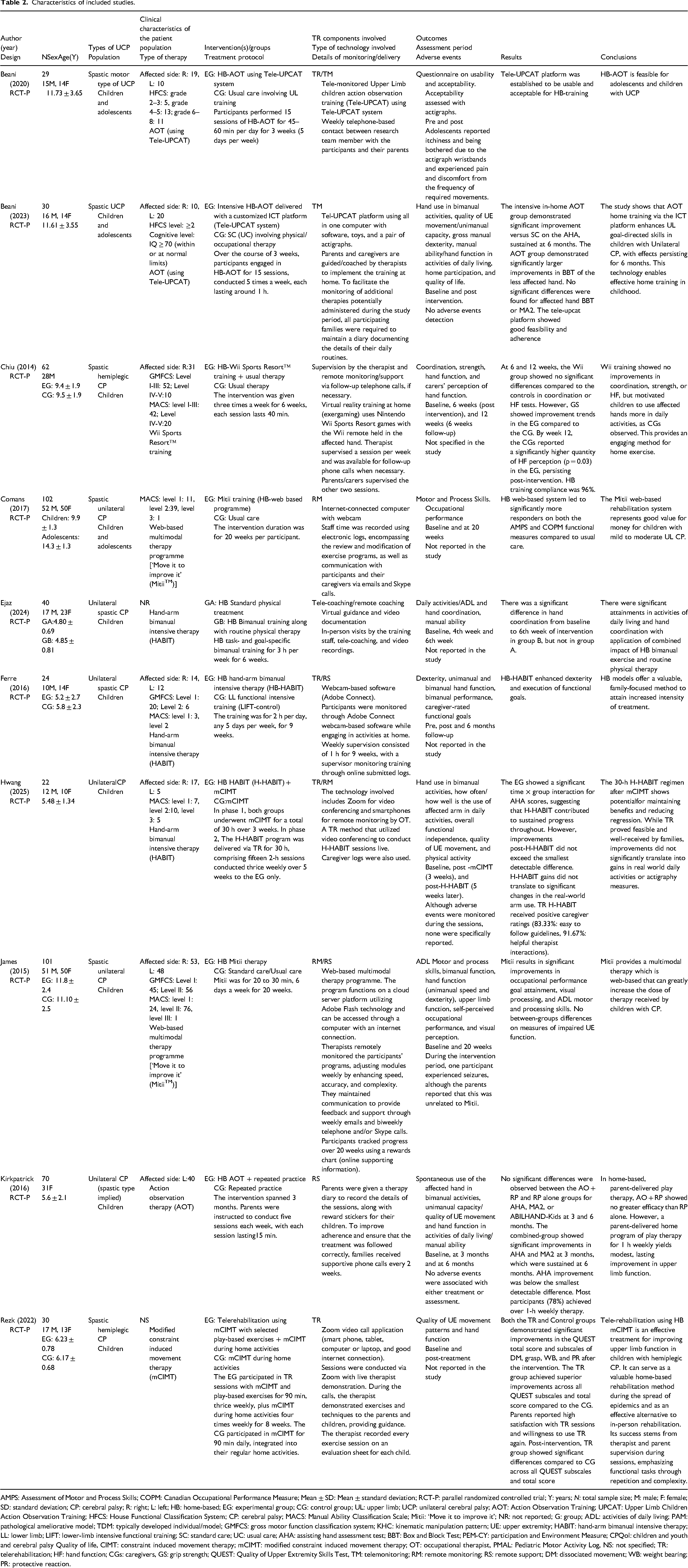
AMPS: Assessment of Motor and Process Skills; COPM: Canadian Occupational Performance Measure; Mean ± SD: Mean ± standard deviation; RCT-P: parallel randomized controlled trial; Y: years; N: total sample size; M: male; F: female; SD: standard deviation; CP: cerebral palsy; R: right; L: left; HB: home-based; EG: experimental group; CG: control group; UL: upper limb; UCP: unilateral cerebral palsy; AOT: Action Observation Training; UPCAT: Upper Limb Children Action Observation Training; HFCS: House Functional Classification System; CP: cerebral palsy; MACS: Manual Ability Classification Scale; Mitii: ‘Move it to improve it’; NR: not reported; G: group; ADL: activities of daily living; PAM: pathological ameliorative model; TDM: typically developed individual/model; GMFCS: gross motor function classification system; KHC: kinematic manipulation pattern; UE: upper extremity; HABIT: hand-arm bimanual intensive therapy; LL: lower limb; LIFT: lower-limb intensive functional training; SC: standard care; UC: usual care; AHA: assisting hand assessment test; BBT: Box and Block Test; PEM-CY: participation and Environment Measure; CPQol: children and youth and cerebral palsy Quality of life, CIMT: constraint induced movement therapy; mCIMT: modified constraint induced movement therapy; OT: occupational therapist, PMAL: Pediatric Motor Activity Log, NS: not specified; TR: telerehabilitation; HF: hand function; CGs: caregivers, GS: grip strength; QUEST: Quality of Upper Extremity Skills Test, TM: telemonitoring; RM: remote monitoring; RS: remote support; DM: dissociated movement; WB: weight bearing; PR: protective reaction.
Outcomes reported
Narrative synthesis
Effects of the interventions
Telerehabilitation-monitored HB therapies demonstrated consistent positive improvements in UE function-related outcomes across the majority of studies in children and adolescents with UCP (predominantly spastic UCP studies) (low certainty of evidence due to high ROB and imprecision).
Discussion
This systematic review aimed to assess the scientific evidence on the effects of TR-monitored HB therapies on UE function-related outcomes in children and adolescents with CP. The major findings of this systematic review indicated that TR-monitored HB therapies showed consistent positive improvements in UE function-related outcomes. These improvements include hand coordination, dexterity, bimanual hand function, ADL motor and processing skills, occupational performance, and the execution of functional goals in children with UCP (predominantly spastic UCP studies).
The results showed that HB UE bimanual training/therapy improved hand coordination, dexterity, and execution of functional goals. Such improvements could enable children with UCP to perform everyday tasks requiring UE function more efficiently. This is crucial because mobility difficulties are defining features of Children with CP and are the focus of extensive therapeutic interventions. 32 It is noteworthy that the observed positive impact may not solely result from bimanual training or therapy. Instead, this may be attributed to the emphasis on and integration of tele-coaching/remote monitoring and telerehabilitation in home-based training. This suggests that the combination of monitored home-based training and telerehabilitation is advantageous in assisting children with UCP in the effective performance of UE-related activities. This is significant because most ADLs require the coordinated use of both hands, and enhancing the functionality of the more affected UE to improve daily activities, including grooming, eating, and dressing, is important. 33 In addition, the findings are important because good UE coordination is crucial for the required functioning in everyday life. 34
The improvements due to H-HABIT can be attributed to various reasons: intensive rehabilitation interventions, rooted in the principles of motor learning, involve children in the practice of skillful movements, with enhancements in UE function posited to be linked to neuroplastic adaptations. 35 The HABIT process emphasizes bimanual coordination skills in the hands while preserving the intensive characteristics of constraint therapy. 36 In addition, the intervention incorporates a structured approach to practicing bimanual hand function through activities that are both child-friendly and selected by the children themselves based on their personal objectives and preferences. 36 This is supported by the statement that HABIT enhances UE function in children with CP and extends beyond typical bilateral coupling or mirror movements, integrating asymmetrical hand movements, and employing neuroplasticity and motor learning principles. 37 Furthermore, the implementation of synchronous telerehabilitation or telemonitoring in two studies on H-HABIT may have contributed to the favorable outcomes. These approaches potentially facilitate error-free exercises, enhance motivation, and promote increased practice and repetition.
The findings of a study indicated that Tele-UPCAT delivered HB AOT was feasible, and the Tele-UPCAT system showed usability and acceptability for HB training in children and adolescents with spastic UCP. In another study, AOT also demonstrated a significant improvement in bimanual hand function in children and adolescents with spastic UCP after treatment. These positive effects underscore the crucial role of HB AOT when combined with telerehabilitation and monitoring on these parameters in children and adolescents with UCP. This finding is advantageous because the premotor cortex serves as an alternative target due to its greater chances of survival and extensive connections within the motor network. 38 Additionally, improved bimanual function may facilitate more effective execution of activities using the UE. Hence, administering HB AOT alongside telerehabilitation and monitoring in children with UCP will be beneficial for their rehabilitation process.
The positive effects of AOT may stem from the fact that it holds significant promise for promoting motor recovery by activating the mirror neuron system through the observation and imitation of actions, and may enhance the effects of conventional therapies, and offers a novel mechanism to facilitate neuroplasticity. 39 This can be supported by the statement that AOT involves watching others’ actions and aligning them to internal representations, and observing the actions creates an internal representation of movement in the brain, enhancing motor memory and performance. 40 Additionally, another reason may be that AOT leverages the mirror mechanism in a more direct manner than mirror therapy, as it involves patients observing everyday activities carried out by other healthy individuals. 41 Moreover, the implementation of the Tele-UPCAT system in certain studies may have influenced the effects of the interventions.
Mitii therapy has a positive impact on occupational performance, goal attainment, visual processing, and ADL motor and processing skills. The improvements are possible because, in addition to the therapy being a web-based multimodal, there were live interactions and constant communication and monitoring through e-mails, telephone calls, and Skype calls. This highlights the crucial role of integrating telerehabilitation with monitoring. Improvement in ADL motor and processing skills, along with occupational and functional performance measures, is essential for enabling children with spastic UCP to perform daily tasks involving the UE with minimal difficulty. The positive effects of Mitti therapy may be due to certain factors: repetitive, intensive, and progressively demanding training is required to induce brain plasticity. 42 This is supported by the assertion that Mitii provides intensive and progressively challenging training in the cognitive, visual perceptual, and physical function domains. 43 In addition, web-based comprehensive training that enhances motor and cognitive skills through interdisciplinary virtual trainers may serve as a cost-efficient method for providing therapy and promoting skills translation into community and home environments. 42
The findings also revealed a trend of increased grip strength due to Wii Sports Resort Training in one study, while another study showed improved UE function due to mCIMT. The positive effect of Wii training could be due to certain factors. While mirror neurons contribute substantially owing to the multimodal stimulation offered by Nintendo Wii treatment (NWT), the advantages of NWT are mainly due to motor learning and neuroplasticity. 44 Additionally, it has been reported that considering the repeated practice, specific tasks, multisensory integration, and intensity that NWT facilitates, it is plausible to induce activity-dependent neuroplasticity. 44 These assertions are corroborated by prior suggestions indicating that, given the capacity of Wii Fit training to influence neural plasticity, such training could serve as a movement-priming adjunct to rehabilitation. 45 Other factors might be linked to HB and the adherence nature of the training, as research indicates that HB Wii Fit training is both safe and feasible, potentially offering benefits for children with CP, with the Wii Fit games suggested to offer both motivation and enjoyment, resulting in nearly complete adherence. 46 Moreover, it has been reported that a critical determinant of the efficacy of any intervention is the duration allocated to training and rehabilitation activities, a concept referred to as dosing. 47 Therefore, these factors likely contributed to the findings.
The observed effect of mCIMT can be attributed to the key principles of CIMT. They include counteracting maladaptive plasticity in patients with unilateral hemispheric damage (congenital or acquired), and constraining the nonparetic extremity while conducting an intensive motor activity training targeting the affected extremity with the goal of enhancing function. 48 Furthermore, it has been documented that activity-dependent cortical reorganization associated with CIMT may constitute the neural foundation for long-term enhancement in the utilization of the affected limb during daily activities post-treatment. 49 One significant limitation is that the findings on Wii training and mCIMT are each based on single studies, providing insufficient evidence for definitive conclusions to be drawn. Further research is needed in these areas.
Importantly, the positive effects of the therapies observed may be greatly attributed to the home-based nature of the training and the use of telerehabilitation or telemonitoring. The HB nature of the interventions is crucial, as research has reported that an essential advancement in rehabilitation practice is the sustained implementation of training within the child's everyday life and home environment, empowering the parents, and enhancing the autonomy of both the parents and the child from healthcare professionals. 50 Additionally, administering therapy in a home setting offers the benefit of being more resourceful, as it is more supportive, comfortable, meaningful, and welcoming for children compared to the daunting atmosphere of clinical or hospital facilities. 51 These assertions could be supported by the findings that home-based rehabilitation, whether face-to-face or via telerehabilitation, is regarded as more accessible and convenient than services in facility setting. 52 Furthermore, the success recorded with HB therapies may be attributed to its other unique characteristics, as HB training is recognized as a crucial intervention for the rehabilitation of children with CP, both currently and in the future, enabling parents to actively participate in their child's therapeutic regimen and allowing children to develop new skills within their familiar setting. 50
Furthermore, the implementation of telerehabilitation or tele/remote monitoring and supervision, whether conducted synchronously or asynchronously in the studies, may have positively influenced the outcomes, possibly due to various contributing factors. These include providing accessibility (removing barriers), and precision rehabilitation through telecommunication technologies. 53 There could also be improved treatment adherence through remote coaching/monitoring, as it has been reported that telemonitoring through a mobile application likely enhances adherence to exercise regimens. 54 Importantly, the successful implementation of this approach may demand critical consideration of various factors, as the effective deployment of remote patient monitoring necessitates addressing obstacles at the clinician, service, and patient levels, including considerations of technical quality, data governance, digital literacy, and reimbursement. 55 This aligns with a report that various factors affect the effective implementation of in-person home-based rehabilitation and telerehabilitation services, encompassing both facilitators and challenges. 52 In essence, telemonitored home-based therapies may ensure practice and learning in real-world environments, thereby enhancing treatment outcomes.
This systematic review highlighted the crucial role of TR-monitored HB therapies in positively enhancing UE function-related outcomes in children and adolescents with UCP (predominantly spastic UCP studies). These therapies may ensure task practice and learning by children and adolescents with CP in real-world settings, thereby enhancing the treatment outcomes. These findings are essential for achieving optimal functionality. However, since the findings were primarily based on narrative synthesis and involved a limited number of studies, some of which had small sample sizes and certain methodological limitations. These factors may have influenced the outcomes of this review. Currently, the studies included represent the available and accessible studies in the subject area based on the focus and criteria of this review. The synthesized results and evidence indicate a positive effect of TR-monitored HB therapies on the outcomes of interest based on these accessible studies. Consequently, as more studies become available, further research with a larger number of studies and meta-analyses is necessary to substantiate this evidence.
Strengths and limitations
The primary strengths of this review encompass a comprehensive search of databases and additional sources, adherence to PRISMA guidelines, and the utilization of appropriate evaluation tools to assess the MQ and risk of bias ROB of the included studies. The studies included in the review had good MQ, and most of them had a low ROB in most domains of the Cochrane ROB tool, thereby enhancing the overall strength of the evidence. The primary limitation of this review is the absence of a meta-analysis for the outcomes, attributable to either an insufficient number of studies reporting these outcomes or the significant variability among the studies. Various factors contributed to the limitations of this systematic review, including differences in the administered HB interventions, variations in the control groups, diversity in the components of telerehabilitation employed, inconsistency in the outcome measures for certain outcomes across some studies, and technical challenges in the technologies used during the interventions. In addition, the review is susceptible to language and publication bias, as the exclusion of studies that are not in English or unpublished may lead to skewed results. The primary limitations identified in the included studies include a high ROB in the performance bias domain across the majority of the studies, and in most studies (five out of nine), the sample sizes were relatively small, with each involving fewer than 50 participants. Additionally, the included studies revealed shortcomings in safety reporting, as adverse events were not reported, underreported, or insufficiently captured in some studies, thereby restricting the evaluation of the associated potential harms. Therefore, further research is necessary to address these limitations and substantiate our findings.
Conclusions
Telerehabilitation-monitored home-based therapies showed potential to improve upper extremity function-related outcomes in children and adolescents with unilateral cerebral palsy (predominantly spastic UCP studies).
Supplemental Material
sj-docx-1-jtt-10.1177_1357633X261420104 - Supplemental material for Effects of telerehabilitation monitored home-based therapies on upper extremity function-related outcomes in children and adolescents with unilateral cerebral palsy: A systematic review
Supplemental material, sj-docx-1-jtt-10.1177_1357633X261420104 for Effects of telerehabilitation monitored home-based therapies on upper extremity function-related outcomes in children and adolescents with unilateral cerebral palsy: A systematic review by Jibrin Sammani Usman, Thomson Wai-Lung Wong and Shamay Sheung Mei Ng in Journal of Telemedicine and Telecare
Supplemental Material
sj-docx-2-jtt-10.1177_1357633X261420104 - Supplemental material for Effects of telerehabilitation monitored home-based therapies on upper extremity function-related outcomes in children and adolescents with unilateral cerebral palsy: A systematic review
Supplemental material, sj-docx-2-jtt-10.1177_1357633X261420104 for Effects of telerehabilitation monitored home-based therapies on upper extremity function-related outcomes in children and adolescents with unilateral cerebral palsy: A systematic review by Jibrin Sammani Usman, Thomson Wai-Lung Wong and Shamay Sheung Mei Ng in Journal of Telemedicine and Telecare
Footnotes
Ethical consideration
Not applicable
Consent to participate
Not applicable
Consent for publication
Not applicable
Author contributions
All authors contributed to the study design, conception, methodology, analysis, and interpretation of the data. JSU drafted the manuscript; JSU, TWLW, and SSMN critically revised the manuscript for important intellectual content. All authors have read and approved the final version of the manuscript.
Funding
This research was funded by a grant from the General Research Fund (Reference Number: 15126224
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data will be made available by the corresponding author on reasonable request
Supplemental material
Supplemental material for this article is available online.