
Abstract
Background:
Non-medical drivers of health, including social, demographic, and geographic conditions, play an important role in shaping women’s healthcare use in rural settings. How these intersecting factors form patterns that influence care seeking remains underexamined.
Methods:
A cross-sectional survey (n = 159) was conducted through public health service sites across 29 rural counties in Texas, United States. K-means clustering identified groups of women with shared patterns of health burden, health-related social needs, and geographic proximity to care. Chi-square tests and one-way ANOVA assessed demographic differences, and a Generalized Linear Model estimated the proportion of times participants reported receiving needed care based on profile membership and demographics.
Results:
Seven clusters, interpreted as profiles, reflected variation in combinations of health burden, health-related social needs, and geographic proximity. Cluster membership and difficulty affording healthcare were significantly associated with higher odds of receiving needed care. Women in profiles characterized by multiple co-occurring constraints, as well as one profile marked by elevated health-related social needs, had significantly lower odds of receiving care compared to the reference profile with no constraints.
Conclusions:
Findings suggest that profile-based, analytic approaches may help clarify differences in unmet care needs and inform more targeted efforts to address delayed or forgone care in rural settings.
Keywords
Introduction
Persistent differences in health outcomes are closely tied to the social and structural conditions in which people live. 1 These contextual factors include interconnected demographic, socioeconomic, geographic, and place-based conditions that can increase exposure to adverse life circumstances, shape the navigation capacity of institutional systems, and create substantial barriers to accessing the healthcare, social services, and resources essential for building and maintaining overall health and well-being. 2 Often referred to as non-medical drivers, such factors tend to operate in combination rather than in isolation, influencing both patterns of engagement with healthcare systems, and, ultimately, health outcomes. 3 In rural areas, influential intersecting qualities of place include less availability of primary and specialty care providers, fewer public social support services, long travel distances to care, and constrained employment opportunities that reduce insurance coverage and income, limiting the ability to absorb costs and overcome such barriers to seeking and receiving care when needed.4,5
With approximately 16% of its 30.5 million residents living in rural areas, 6 Texas has the largest rural population in the United States and offers a relevant case study for examining differences in rural care-seeking patterns common at the state level. 7 These differences are driven by a combination of institutional (eg, absence of Medicaid expansion), geographic (eg, expansive rural land areas), and sociodemographic (eg, unemployment, uninsurance rates, food and housing insecurity) conditions. 7 Recent evidence suggests that these intersecting conditions shape care-seeking behavior and accessibility in ways not fully captured by single-factor or demographic approaches, particularly in under-resourced regions. 8 General care availability also remains a concern, with rural Texas counties being more likely than urban counties to be classified as primary care shortage areas. 9
Women living in rural areas across the United States experience these conditions acutely, contributing to differences in health behavior and outcomes when compared to those in urban areas.10,11 Rural women in Texas are no exception and face disproportionate risks across several indicators, especially as multiple such social and geographic determinants (such as physical location, community-level vulnerability, and insurance access) frequently cooccur (Supplemental Figure A.1). These co-occurring conditions can influence whether and when women seek care, contributing to worse health outcomes for rural women compared to men and their urban counterparts, including higher rates of chronic disease, obesity, and hospitalization, as well as lower rates of preventive screening and later-stage cancer diagnoses with poorer survival rates.12-14 They also contribute to reduced engagement in maternal care. 15 In 2020, only 68% of Texas mothers initiated prenatal care during the first trimester (the lowest rate of any U.S. state), with even lower rates observed among Hispanic and non-Hispanic Black women. 15 Delayed or forgone care represents not only a marker of unmet needs, but also a potential mechanism through which non-medical drivers translate into long-term health differences among groups. 16
This study examines an application of understanding care seeking using survey data from rural women to identify shared contextual profiles defined by indicators of health burden, health-related social needs, and geographic care availability. By assessing how these profiles relate to getting care when needed, the findings demonstrate an analytic approach that can offer insight into localized drivers of delayed or forgone care and may be useful for service planning in comparable rural settings.
Methods
Study Area
This study focused on rural counties in Texas’ Public Health Region 4/5, serviced by jurisdiction 4/5N. Rurality was determined using the U.S. Department of Agriculture’s (USDA) 2023 Rural-Urban Continuum Codes (RUCC); categories 4 to 9 were considered rural. 17 Of 38 counties in the region, 29 met the inclusion criteria (Supplemental Figure A.2).
Participants
The study presents cross-sectional data collected from adult (over 18 years old) individuals identifying as female (henceforth, women) receiving health services within the study area. Data were collected online through the survey platform Qualtrics. Participants were primarily recruited in person at Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) service centers, particularly those serving clients from rural counties. While at the centers for appointments, which included WIC voucher pick-up as well as other general health and education services, participants were recruited both actively by staff and passively via advertisements. A small portion of participants were recruited at community-health events near WIC centers. Participants received a small bag of personal hygiene items (worth less than $15) if they completed the survey on-site; otherwise, they received no incentive.
Survey Construction and Measures
The survey included up to 50 items assessing demographics, health status, geographic access, socioeconomic factors, health information preferences, and care-seeking behaviors. After screening for completeness and consistency, 159 responses were retained. Variables were then operationalized and prioritized for analysis due to sample size. 18
Demographic characteristics were obtained from self-report. Items prioritized were age, pregnancy status within the past year, race/ethnicity, insurance status, employment status, and difficulty affording healthcare. Age was continuous and included to account for differing health needs of younger and older women. Employment, insurance coverage, and the ability to afford healthcare were included as they are often associated with greater access to and use of care. 5 Insurance and pregnancy statuses were assessed with yes-no questions. Employment statuses included employed full-time, employed part-time, seeking work, retired, and not currently working. Race/ethnicity categories included American Indian/Alaska Native, Asian, Black/African American, Hispanic/Latino, Middle Eastern/North African, Native Hawaiian/Pacific Islander, White, and other. Employment and race/ethnicity categories were dichotomized due to low sample sizes. Difficulty affording all healthcare costs was assessed using a 4-point Likert-type scale and dichotomized based on the 2 highest points of the scale.
Health burden was defined by having a chronic condition, as well as ratings of physical and mental health and health-related quality of life, widely used and reliable survey measures that have been associated with healthcare utilization. 19 Chronic condition status was assessed with a yes-no question and included to reflect increased care needs or exacerbated health issues. 20 Health quality was self-assessed using a 5-point Likert-type scale and considered poor if the worst 2 scale points were rated for current mental and physical health and if the worst 3 scale points were rated for health-related quality of life.
Health-related social needs were assessed with ratings of access to basic resources needed for living (transportation, food, housing, and income). 2 Access to each of these resources was rated using a 3-point Likert-type scale. Geographic availability of care was represented by using counts of up to 5 healthcare facility types within 30 min, a threshold at which travel time begins to significantly deter care-seeking behavior. 21
The primary outcome was getting different types of care when needed. Delays or failures in receiving needed care are linked to poorer outcomes, including reduced long-term care utilization, worsened chronic disease, and higher mortality. 22 Care access frequency was calculated as a proportion, summing the number of (up to 13) care types received when needed and dividing by the total number of care types received and not received.
Analytical Approach
Cluster analysis was used to identify subgroups of rural women with shared patterns of health burden, health-related social needs, and geographic availability of care and examine their collective impact on receiving care when needed. Latent class analysis was not used due to the small sample and numerous categorical variables, which risked overfitting and unstable results. 23 Data were first standardized and explored with K-means clustering using the scikit-learn library in Python, assessing the contribution of various individual measures to defining contextual profiles. To improve performance and interpretability, 3 binary composite variables were created: health burden, health-related social needs, and geographic availability (Supplemental Table 1). Simplifying variables reduced sparse feature spaces and “cube corner” effects that complicate cluster geometry. 24 The cutoffs selected reflected indicators of contextual constraints and included high health-related social needs (≥2 indicators), low geographic availability of care (≤2 facilities within 30 min), and high health burden (having a chronic condition or ≥2 poor health indicators). While some specificity was lost, dimensionality reduction improved stability and preserved the ability to examine the overlapping and mutually reinforcing contextual factors shaping care access. 2
The consolidated variables were explored again with K-means clustering to identify natural groupings (contextual profiles) within the data. K-means was selected due to its computational efficiency, widespread use in applied research, and ease of interpretation. 24 The final seven-cluster solution demonstrated strong performance across validation metrics, indicating reliable, distinct, and well-defined clusters (silhouette score, 0.93; Davies-Bouldin Index, 0.403; Calinski-Harabasz Index, 513.7).
Once clusters were established, one-way ANOVA and Chi-square tests of independence with post-hoc adjusted standardized residual analysis examined if clusters differed by demographic characteristics. A Generalized Linear Model (GLM) with binomial distribution and a log link function was used to model the percentage of times successfully getting care when needed based on cluster membership while accounting for age; employment, insurance, and pregnancy status; identifying as a person of color (POC); and difficulty affording healthcare costs. Statistical tests were performed using SPSS, version 28.0 (Chicago, IL, USA). P values greater than 0.05 were considered significant.
Ethics Approval
The study was performed in compliance with relevant laws and institutional guidelines. All participants’ privacy rights were observed, and participants provided informed consent via the survey interface prior to participation.
Results
Participant Characteristics
Table 1 summarizes demographic characteristics of participants. Slightly over half of participants identified as white (54.1%). The mean participant age was 32.7 years (SD = 11.7). Most were employed either full- or part-time (57.2%). Approximately 23.2% of respondents reported having chronic health conditions. The majority (82.4%, 131) indicated they had children; the average number of children was 2.1 (SD = 1.4). A smaller share reported being born outside the United States (10.0%) or speaking a primary language other than English (8.0%).
Demographic Characteristics of Participants.

Contextual Profiles from the Clustering Approach
The clustering approach identified 7 distinct clusters, interpreted as profiles, in the sample based on indicators of contextual constraints including high health burden, high health-related social needs, and low geographic availability of care. Table 2 summarizes these dimensional characteristics of women in each cluster. Figure 1 shows the scatter plots of the characteristics from 2 angles to visualize the position and separation of each cluster, with lines from the origin marking the central point (centroid).
Profiles of Contextual Constraints Identified Through K-means Clustering.

Indicators of contextual constraints are shown for women in each cluster. Cluster 0 is the reference cluster with no indicators. Low constraint is defined by the presence of 1 indicator; moderate, by the presence of 2 indicators; and high, by the presence of all indicators.
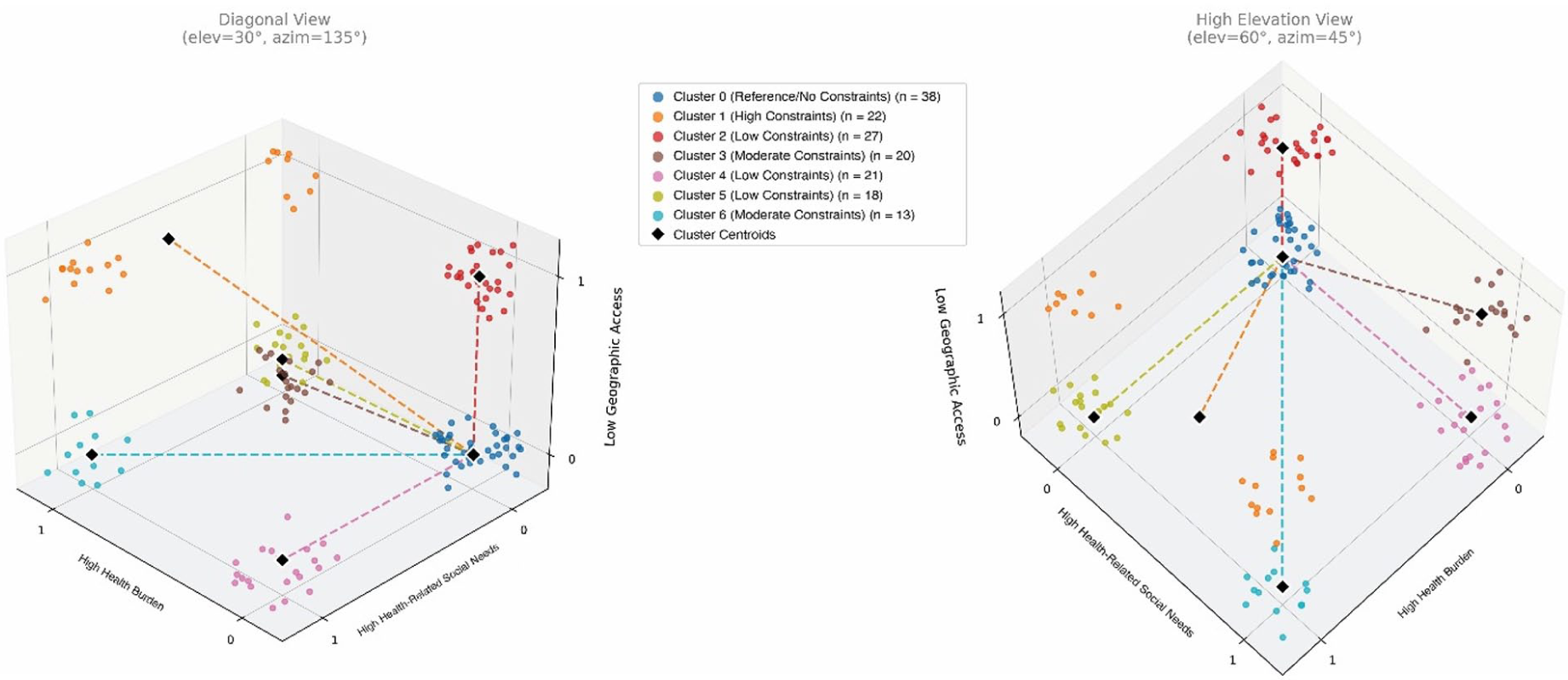
Health burden, health-related social needs, and geographic availability of care visualized for women across clusters.
Cluster 0, with 23.9% of women, represented the reference (control) cluster (with no indicators of constraint). Low constraint profiles (with 1 indicator) were represented by Cluster 2 (17%), Cluster 4 (13.2%), and Cluster 5 (11.3%). Moderate constraint profiles (with 2 indicators) were Clusters 3 (12.6%) and 6 (8.2%). The high constraint profile (with all indicators) was represented by Cluster 1 (13.8%). Overall, 41.5% of women fell into low profiles, 20.8% into moderate profiles, and 13.8% into the high profile.
Table 3 presents demographic characteristics across clusters. The highest rate of insurance coverage was in Cluster 5, a low constraint profile, while Cluster 6, a moderate profile, had the lowest coverage. Employment rates were also highest in Cluster 5 (72.2%) and lowest in Cluster 6 (46.2%). Women of color were most represented in Cluster 4 (61.9%), a low constraint profile, and least represented in Cluster 5 (33.3%). Difficulty affording healthcare was most frequently reported in Cluster 1 (63.6%), the high constraint profile. Cluster 4 had the most women who had been pregnant within the past year (57.1%), while Cluster 5 had the least (22.2%).
Distribution of Demographic Characteristics Across Clusters.

P < .05.
A one-way ANOVA and chi-square tests of independence assessed statistical differences in demographic characteristics among clusters. Post hoc analyses with a Bonferroni correction (α_adj = .004) were conducted using adjusted standardized residuals to identify cells contributing to overall significance. Only having insurance demonstrated a significant association with cluster membership, χ²(6, N = 159) = 14.11, P < .05, with women in Cluster 5 being significantly more likely to have insurance (adjusted residual = 2.92, P < .001).
Impact of Cluster-Profile on Receiving Care
A GLM with binomial distribution and a log link function modeled the percentage of times getting care when needed based on cluster membership, accounting for age; employment, insurance, and pregnancy status; identifying as a POC; and difficulty affording healthcare. An Omnibus test was significant, χ²(6, n = 151) = 98.80, P < .001, indicating a better fit than the intercept-only model. When compared to a reduced model with only demographic predictors, a likelihood ratio test indicated the full model with cluster membership provided a significantly better fit to the data, χ²(6) = 70.32, P < .001. Despite some overdispersion in both models, goodness of fit statistics also supported this conclusion, with the full model demonstrating lower deviance (deviance/df = 3.09) compared to the reduced model (deviance/df = 3.46), as did Akaike’s and Bayesian information criteria (AIC = 584.11 vs. 643.43, BIC = 650.10 vs. 678.96).
Results (Table 4) indicated that both cluster membership and difficulty affording health care were significant predictors of receiving care when needed. Compared to women in Cluster 0, those in Cluster 1 (OR = 0.28, P < .001), Cluster 3 (OR = 0.15, P < .001), Cluster 4 (OR = 0.47, P = .020), and Cluster 6 (OR = 0.26, P < .001) had significantly lower odds of receiving care when needed. Difficulty affording health care was the only demographic characteristic independently associated with reduced odds of receiving care when needed (OR = 0.42, P < .001); no others were significant (all P > .05).
GLM Results Examining Receiving Needed Care Based on Cluster Membership and Demographic Characteristics.
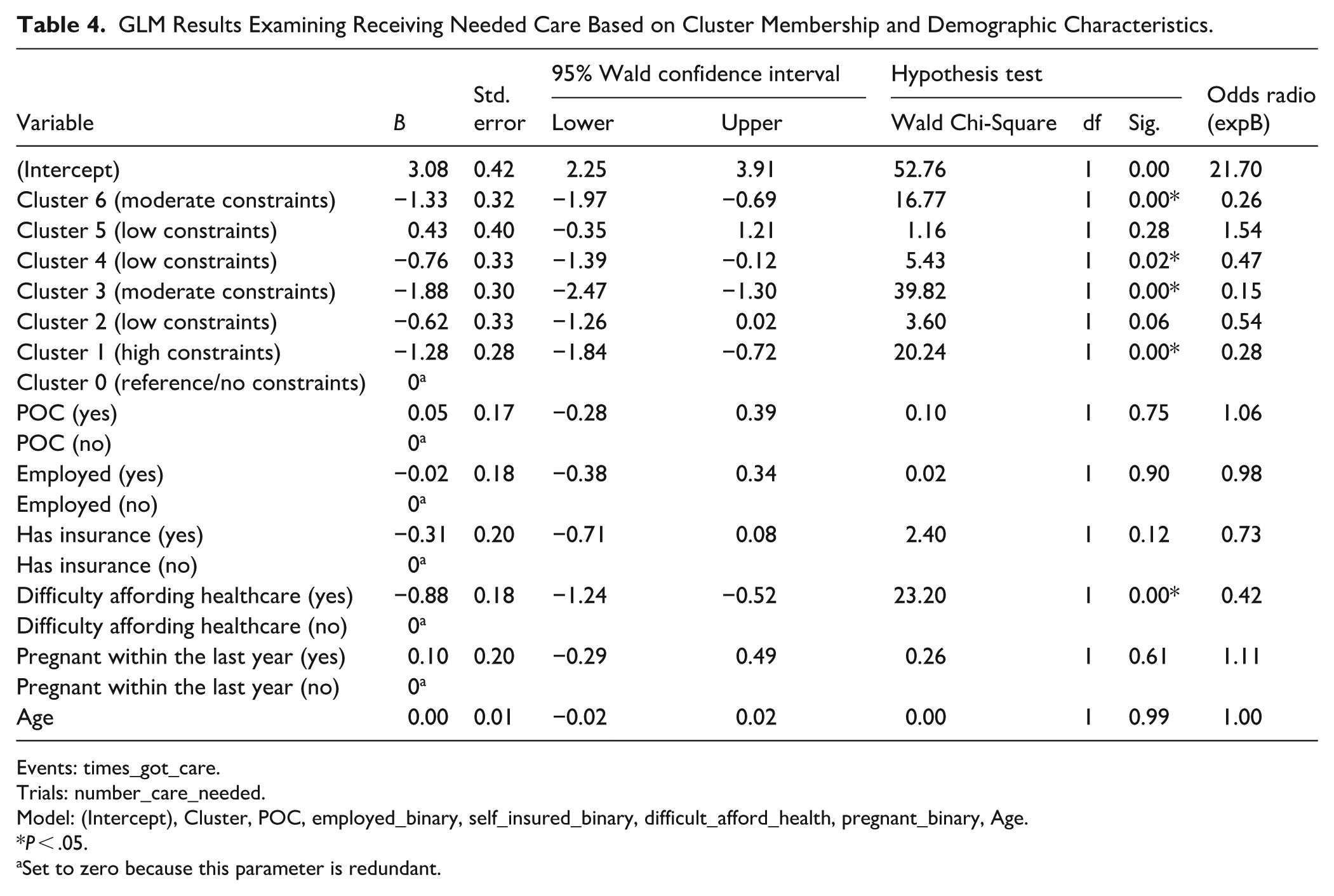
Events: times_got_care.
Trials: number_care_needed.
Model: (Intercept), Cluster, POC, employed_binary, self_insured_binary, difficult_afford_health, pregnant_binary, Age.
P < .05.
Set to zero because this parameter is redundant.
Discussion
Seven clusters, interpreted as profiles, were identified based on contextual constraint indicators of health burden, health-related social needs, and geographic availability of care. Cluster membership significantly predicted getting care when needed, more so than individual demographic factors. Apart from one profile (4), those with fewer indicators of constraint (0, 2, 5) showed no impact on receiving care when needed, whereas profiles with more indicators (1, 3, 6) were associated with worse odds. Demographic variables were not significant, except for difficulty affording care. Limited sample size likely contributed to the lack of demographic differences, a finding deviating from broader literature. 25
Notably, women in some low-moderate constraint profiles (3 and 4) with low health burden reported worse care access than those in higher constraint profiles, suggesting compounding effects of social and geographic barriers even without health issues, as both showed high health-related social needs. Although those groups indicated fewer indicators of ongoing health issues warranting care, their lower reported access could indicate possible difficulties obtaining acute care for emergent issues, an important concern given that limited emergency care availability in rural areas is linked to worse health outcomes, including higher mortality. 26 The relatively high proportion of pregnant women in Cluster 4, while not statistically significant, may have influenced this pattern and could emerge more clearly with a larger sample size. This is consistent with prior research showing that pregnant women experiencing multiple health-related social needs or socioeconomic difficulties often receive fewer prenatal services and procedures, even when they have Medicaid. 27 Nonetheless, the findings also indicated that coverage-related factors still mattered within the context of constraints: insurance status emerged as the only statistically significant demographic variable differing among clusters, and difficulty affording care was the only significant demographic predictor of reduced odds of receiving care when needed. This aligns with evidence emphasizing the enabling role of insurance in encouraging the use of health services in rural and under-resourced contexts.8,28-30
More generally, the findings add to a growing body of work demonstrating that care use is rarely constrained by a single determinant, but instead reflects the interaction of multiple co-occurring needs.3,31 Consistent with prior studies showing that multidimensional needs profiles can better explain variation in care use than isolated indicators,32-34 especially when insurance coverage and financial resources intersect with geographic barriers, 32 the findings emphasize that layered constraints common in rural areas may compound unmet need even among individuals without chronic conditions or self-reported poor health. 35 That characteristics such as employment, insurance, or race alone were not independently predictive further underscores the inadequacy of unidimensional approaches and the need for more holistic assessment frameworks that move beyond basic demographic targeting to optimize services and expand access points.
Although broader reforms addressing fundamental issues with healthcare costs, insurance coverage, and structural drivers of health-related social needs are often concentrated at institutional or policy levels, such frameworks can combine individual-level health-related social needs screening with area-level measures to improve targeting of outreach, navigation, and wraparound services at more local levels.34,36 This type of practice-, community-, and/or locality-oriented analysis may be particularly useful for identifying types of individuals at risk for delayed or avoided care, whose personal needs may differ from the average socioeconomic conditions of typical residents31,33 and, if persistently unaddressed, may increase the likelihood of escalating needs that are more intensive to meet, especially in already under resourced rural communities. It also supports a more complete understanding of constraints facing local community or clinic populations, specifically, which constraints are most prevalent, which cooccur to form locality-based patterns, and what proportions of individuals experience low, moderate, or high cumulative access or care-use burden.
Such insights can help both community health systems and local service providers identify the extent of overlapping constraints, as well as the specific combinations potentially contributing to missed appointments or delayed care, and thereby prioritize more relevant, multi-domain solutions or support for these groups. At the community level, care models might be adapted to better leverage local infrastructure (eg, co-located health and social services, mobile clinics, community care teams, expanded community-systems partnerships) and encourage more precise matching of patients to bundled supports rather than generic referrals.33,34,36 In this context, simultaneous efforts to strengthen local affordability supports, streamline care navigation, and better coordinate service and follow-up referrals may further reduce cumulative barriers, 34 especially in rural communities with provider or service shortages37-39 where improved coordination may enhance the efficiency and responsiveness of existing infrastructure.
At the practice level, these insights could translate into concrete strategies to expand access to patient groups experiencing high cumulative burden. Depending on profiles of needs, strategies might include expanded clinic hours, flexible or same-day scheduling options, team-based staffing models centralizing advanced practice providers and care coordination teams, local transportation partnerships, and/or service outreach through mobile units to community public services sites (eg, WIC clinics, schools, libraries). 40 These types of expanded services or availability options might help mitigate non-insurance-related cost burdens, such as lost wages or transportation expenses associated with attending appointments, that compound access challenges in rural settings.5,40 Additionally, as provider communication and trust-building interventions have been shown to improve adherence to recommended care, 41 including in the context of cost-related nonadherence, 42 incorporating a profile-informed understanding of patients’ access constraints could enhance these strategies by helping to tailor communication and recommendations to their specific circumstances.
Ultimately, the findings suggest that integrating individual-level needs mapping into rural health planning may help clarify intersecting factors shaping differences in care seeking 31 and support more targeted local service delivery at different entry points, as reflected in successful multilevel, socioecological programs currently implemented in many rural and underserved communities.43-45
Strengths and Limitations
This study offers insights drawn from a localized context not easily captured in larger population-level or aggregated datasets. 46 Nonetheless, several limitations must be considered. The cross-sectional design and non-random sampling limit causal inference. The modest sample size also constrained analytic power and limited variable inclusion. The use of composite variables may have reduced insight into within-group variability, although this is a known trade-off in clustering approaches. 47 Future work could address these limitations, for example, by redeploying the survey to increase sample size, using qualitative methods to examine the lived experiences of women from each profile type to add further contextual richness to understanding their care access, or applying longitudinal designs to assess whether profiles analyzed at a population-level might predict behavioral outcomes and health trajectories over time.
Conclusion
This study identified 7 distinct profiles among rural Texas women, reflecting variation in health burden, health-related social needs, and geographic care availability. Profiles with multiple co-occurring constraints had significantly lower odds of receiving care when needed, underscoring that combinations of non-medical social and geographic factors shape care seeking beyond demographics or health status alone. In contrast, a profile with high health burden but fewer non-medical factors demonstrated relatively good access, highlighting the protective roles of geographic proximity and reduced resource strain. The profile-based analytic approach illustrated here may be useful to apply in other settings to better characterize co-occurring needs of local patient populations, generate hypotheses about the implications of delayed or forgone care in specific groups, evaluate the impact of intervention programs on care seeking that address multiple non-medical drivers of health, and inform future service planning at practice and community levels to support earlier engagement with care in rural health systems.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319261432462 – Supplemental material for Profiles of Non-medical Drivers and Health Burden Associated With Care Seeking Among Rural Women
Supplemental material, sj-docx-1-jpc-10.1177_21501319261432462 for Profiles of Non-medical Drivers and Health Burden Associated With Care Seeking Among Rural Women by Elizabeth Ekren, Saksham Adhikari, Shadi Maleki, Jessica K. Sexton, Christina Aubert, Maria Tomasso, Russell Hopkins and Melinda M. Villagran in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The authors acknowledge the support of Drs. Michelle Crum, Catherine Goetz, Ilia Pashintsev, and Samiksha Srivastava at the University of Texas at Tyler Health Science Center.
Ethical Considerations
This study was conducted under the ethical standards of the Texas State University Institutional Review Board (#9510, June 18, 2024).
Consent to Participate
All participants provided informed electronic consent through a secure survey platform prior to participation.
Consent for Publication
Not applicable.
Author Contributions
E.E. led project conceptualization, survey design and administration, statistical analysis and oversight, and manuscript drafting and supervision. S.A. conducted data cleaning and management, statistical analyses (including clustering code development), figure generation, and contributed to the methods section. S.M. contributed to survey design and administration, map production, and manuscript writing and editing. J.K.S. led development of the discussion section, provided subject-matter expertise, and contributed to manuscript editing. C.A. oversaw recruitment and data collection, supported survey administration and data management, and contributed to manuscript editing. M.T. reviewed the statistical analyses, refined analytic code, and contributed to manuscript editing. R.H. and M.M.V. contributed to project conceptualization, supervision, resource administration, and manuscript editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this research was provided by the Community Health and Economic Resilience Research Center of Excellence at Texas State University.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Participant data are not available due to participant privacy considerations. Python code is available from the authors upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.