
Abstract
Introduction/Objectives:
Exposure to adverse social determinants of health (SDoH) in childhood is associated with poorer long-term health outcomes. Within structurally marginalized populations, there are disproportionately high rates of developmentally vulnerable children. The RICHER (Responsive, Intersectoral, Child and Community Health, Education and Research) social pediatric model was designed to increase access to care in marginalized neighborhoods. The purpose of this study was to describe the children and youth engaged with the RICHER model of service and characterize the needs of the population.
Methods:
A retrospective chart review was conducted on children and youth who accessed primary care services through the program between January 1, 2018 and April 30, 2021. Basic descriptive data analysis was done using Stata v15.1.
Results:
A total of 210 charts were reviewed. The mean age in years at initial assessment was 6.32. Patients most commonly identified their race/ethnicity as Indigenous (33%) and 15% were recent newcomers to Canada. Evidence of at least 1 adverse SDoH was noted in 41% of charts; the most common included material poverty (34%), food insecurity (11%), and child welfare involvement (20%). The median number of diagnoses per patient was 4. The most frequently documented diagnoses were neurodevelopmental disorders (50%) including developmental delay (39%), ADHD (32%), and learning disability (26%). The program referred 72% of patients to general pediatricians and/or other subspecialists; 34% were referred for tertiary neuropsychological assessments and 35% for mental health services.
Conclusions:
Our data suggests that this low-barrier, place-based primary care RICHER model was able to reach a medically, developmentally, and socially complex population living in disenfranchised urban neighborhoods. Half of the patients identified in our review had neurodevelopmental concerns and a third had mental health concerns, in contrast to an estimated 17% prevalence for mental health, behavioral, or developmental disorders in North American general pediatric aged populations. This highlights the impact adverse SDoH can have on child health and the importance of working with community partners to identify developmentally vulnerable children and support place-based programs in connecting with children who may be missed, overlooked, or disadvantaged through traditional models of care.
Keywords
Introduction
It is now widely accepted that exposure to adverse social determinants of health (SDoH) in childhood is associated with poorer long-term health outcomes across a wide range of measures of physical and mental functioning, irrespective of socio-economic status as an adult.1 -4 Research in the fields of developmental neuroscience, molecular biology, and genomics have found adversity can negatively impact the developing brain, cardiovascular system, immune system, and metabolic regulatory controls.5 -9 This leads to disproportionately high rates of developmentally vulnerable children in communities where social and material disadvantages are prevalent.4,5,10
Given that the impact of adverse SDoH accumulates over the life course, and families with multiple forms of disadvantage may not be able to navigate the healthcare system, it is imperative that children at risk for developmental challenges are identified and connected to a primary care provider.4,5,10 -12 For at-risk children, having a primary care provider can lead to early screening of conditions, timely referrals to subspecialists, and coordination of care. 13
To address this issue, there have been an increasing number of social pediatric initiatives (SPIs) across Europe and North America. 14 Social pediatrics is a holistic, multidisciplinary approach to child health care that considers the needs of the child in the context of their family and society; it views medicine through a social justice lens and aims to address SDoH such as income, housing, and education.10,15 -18 SPIs work toward the goal of improving health and developmental outcomes amongst children in equity-deserving populations through place-based care.10,16 Place-based care is a model of care developed to support children from materially disadvantaged neighborhoods by addressing individual, family, organizational, and community level issues through integration of health care into local services and community at-large.19,20
The purpose of this retrospective review was to characterize the population seen by an inner-city, low-barrier, place-based social pediatrics healthcare program using a particular SPI model, RICHER. 4 RICHER is an acronym, standing for Responsive, Intersectoral, Child and Community Health, Education and Research. In this model, nurse practitioners and specialist physicians work hand-in-hand to provide care to children, youth, and their families. Clinicians operate out of a clinic embedded within a social housing complex in the targeted community, and provide outreach to schools, daycares, community centers, and partnered health clinics. 4 Families in the clinic’s catchment area face multiple and intersecting barriers in accessing care—financial, transportation-related, discrimination, and/or previous healthcare-related trauma. 4 Studies have found this area has a high percentage of developmentally vulnerable children.21 -25 A study by the local health authority reported that residents within the catchment area primarily accessed care through ambulance pickups, emergency rooms, street nurses, and police officers rather than through primary care. 26 Additionally, due to community health resources currently focusing on meeting the needs of street-involved adults, there are a limited number of clinics within walking distance where families feel safe accessing care, particularly with children. 27 Nurse practitioners in the program provide care for the whole family, in recognition of the importance of caring for the parent-child dyad. 28 The referral process to the program is barrier-free and can be made by parents, primary care physicians, childcare workers, social workers, other child- and family-serving community organizations, or by drop-in/self-referral. Through this process, community partners help to identify and refer families who may not otherwise access care. Appointments with general and subspecialty pediatricians (developmental and behavioral pediatrics, adolescent health and medicine, child and adolescent psychiatry, and dermatology) and allied healthcare services (eg, social work, massage therapy, and counseling) are offered in clinic to make care more accessible for families. Clinicians meet weekly to discuss and review shared patients, allowing effective collaboration. The clinical team approaches care in a culturally sensitive, trauma-informed manner and works together with community-based organizations to identify and overcome social and structural barriers to healthcare on an ongoing basis.
A primary goal of the RICHER model is to provide low-barrier care. In the context of harm reduction and HIV testing, low-barrier has been sometimes described as “meeting the people where they are” and helping overcome physical or mental barriers, real or perceived.29 -31 In this program, clinicians (both primary care and specialists) practice directly in venues identified by community-based organizations as safe and trusted by families (ie, daycares, schools, community centers, and non-profit family support agencies) as well as a free-standing clinical space. These tactics mitigate barriers that families might otherwise face in connecting to both primary and tertiary care. Understanding the population seen by a program with this unique model of care may inform those who want to employ a similar model in materially disadvantaged communities.
We believe that other programs could utilize the previously published RICHER model to provide low-barrier care through a social pediatric model to structurally marginalized families. However, prior to this study, patient-level characteristics of the program’s population had not been described. The purpose of this project was to describe patient-level characteristics including referral source and diagnoses of a snapshot of the children engaging with this RICHER healthcare model clinic. Our hypothesis is that through its innovative care delivery model, the program provides care to children with complex health needs and facilitates linking these children with necessary health services including pediatric subspecialty care.
Methods
Institutional Research Ethics Board approval was obtained prior to data collection. A retrospective quality improvement (QI) chart review was conducted on patients born after 1993 who accessed primary care services through the program between January 1, 2018 and April 30, 2021. The start date was chosen as it was when the program completed transition to using an electronic medical records system, thus allowing for reliable data accessibility of all patients seen in the nurse practitioner primary care clinic. Round table discussions were held with nurse practitioners, community stakeholders, and physicians to identify variables of interest that would (1) help illustrate the current patient population and (2) aid in future resource allocation. These variables were compiled into a case reporting form used for all eligible files. During the study period, 4249 patients were seen by the 4 primary care nurse practitioners in the place-based social pediatrics clinic. Of those, 3321 were born after 1993. A list of these eligible patients was randomized and the first 210 were selected for inclusion in the study. The number of charts reviewed was a convenience sample due to limitations in available personnel given the significant time required to review each chart. De-identified data including demographics, factors influencing social determinants of health, and past medical history was collected using the REDCap (Research Electronic Data Capture) software (Supplemental Appendix A). Basic descriptive data analysis was done using Stata v15.1.
Results
A total of 210 charts were reviewed. The mean age in years at initial assessment was 6.32 (0.04-25.84). 55% of patients were assigned male sex at birth and 45% female. Patients for whom race-based data were available most commonly identified as Indigenous (33%), Middle Eastern (7%) and Latinx (6%; Table 1). The percentage of patients unspecified was 28%, as race is not consistently collected in Canadian health records. 15% reported they were recent (<5 years) newcomers to Canada (ie, immigrants, refugees, and undocumented).
Demographic Characteristics of Patients Included in the Study (n = 210).
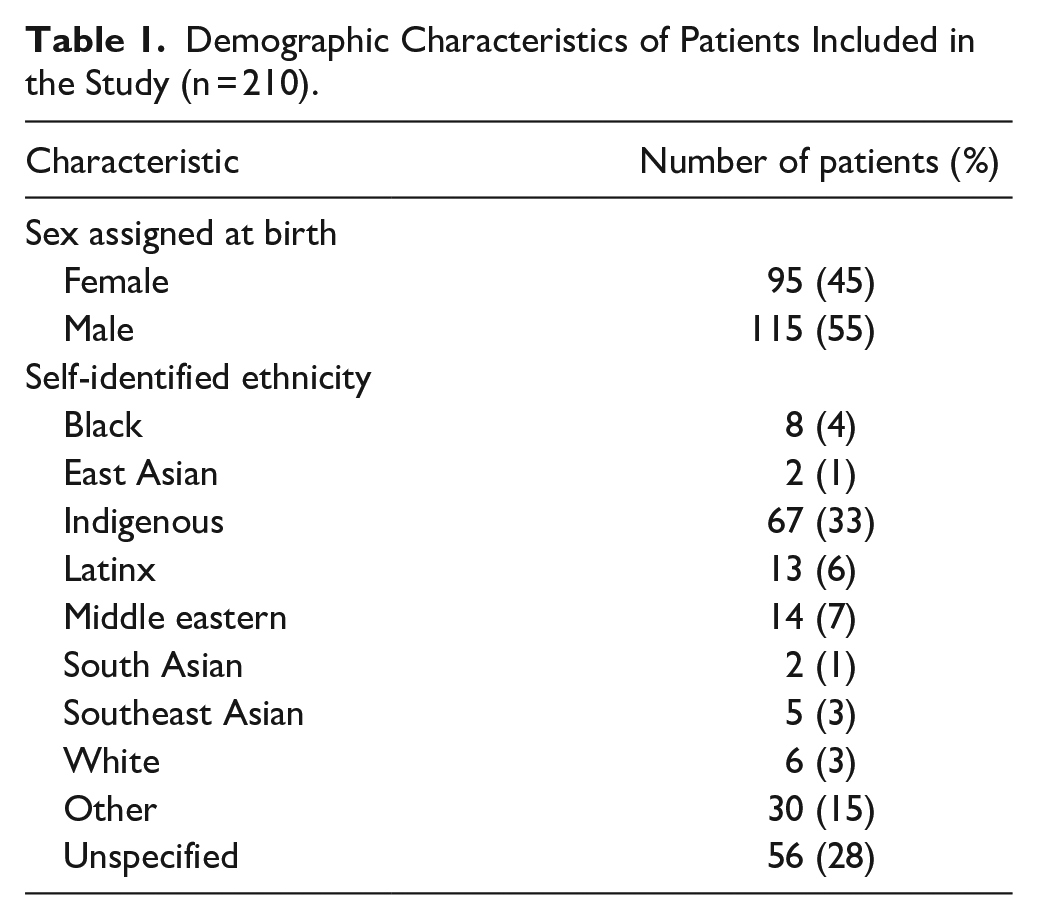
21% of patients had a documented history of being seen by a healthcare provider due to concerns related to a social challenge (eg, situational disturbance, family disturbance, and housing problem). Evidence of at least 1 adverse social determinant of health was noted in 41% of charts: 34% mentioned poverty as an issue, 23% were documented to be receiving government income assistance or tax benefits, and 11% mentioned food insecurity as an issue. Child welfare involvement (current or history of involvement with child protection services) was noted in 20% of charts and 7% of patients had a history of being placed in foster care. Caregiver substance use was documented as an issue in 31% of charts and 3% had history of an incarcerated caregiver. Despite the prevalence of multiple adverse SDoH in these historically oppressed neighborhoods within the program’s catchment area, referral to child protection services was found for only 5% of patients.
The median number of diagnoses per patient was 4 (range: 0-18). The most frequently documented diagnoses were neurodevelopmental disorders (50%) including developmental delay (39%), ADHD (32%), and learning disability (26%; Table 2). Other common diagnoses included skin disorders (36%), acute infection (35%), and asthma (11%). Onward referrals for complex developmental assessments were made for 34% of patients. Mental health concerns were frequently seen in clinic, with it being documented as a primary concern during at least 1 appointment with a nurse practitioner or general pediatrician in 30% of patients and 35% being referred to mental health services (ie, counseling and/or psychiatry).
Diagnoses, Referral Sources, and Outgoing Referrals of Patients Included in the Study (n = 210).

Please note when interpreting this section that the categories are not mutually exclusive, as many patients had more than 1 diagnosis charted.
Social challenge includes the following: psychosocial circumstances, situational disturbance, inadequate material resources, involvement of child welfare services, housing insecurity, family disruption, unspecified counseling for parent/child.
Acute infection includes the following: upper respiratory tract infections, ear infections, common cold.
Other sources of referral include the following: regional delegated Indigenous social service providers, emergency department physicians, in-patient physicians arranging community follow-up, general practitioners, social workers.
Primary care clinicians referred 72% of patients to general pediatricians and/or subspecialists; referrals were most commonly made to general pediatrics (26%), developmental pediatrics (20%), ophthalmology (15%), psychiatry (14%), and dermatology (7%; Figure 1). Psychotropic medications such as stimulants, selective serotonin reuptake inhibitors, alpha agonists, and antipsychotics were documented in 17% of patients.

Referral sources to the place-based primary care clinic lead by nurse practitioners, and referrals from the clinic to specialists (percentage of patients).
The most common referral sources to the primary care program were from schools (20%) and community centers (6%); 17% were walk-in patients and 33% had no recorded referral source (Table 1). Patients referred from schools and community centers were most commonly diagnosed with neurodevelopmental disorders (79% and 77%, respectively) whereas for walk-in patients, the most common diagnoses were skin disorders (53%; Table 3).
Most Common Diagnoses Among Patients Seen in Primary Care Program by Low-barrier or Outreach Referral Source.
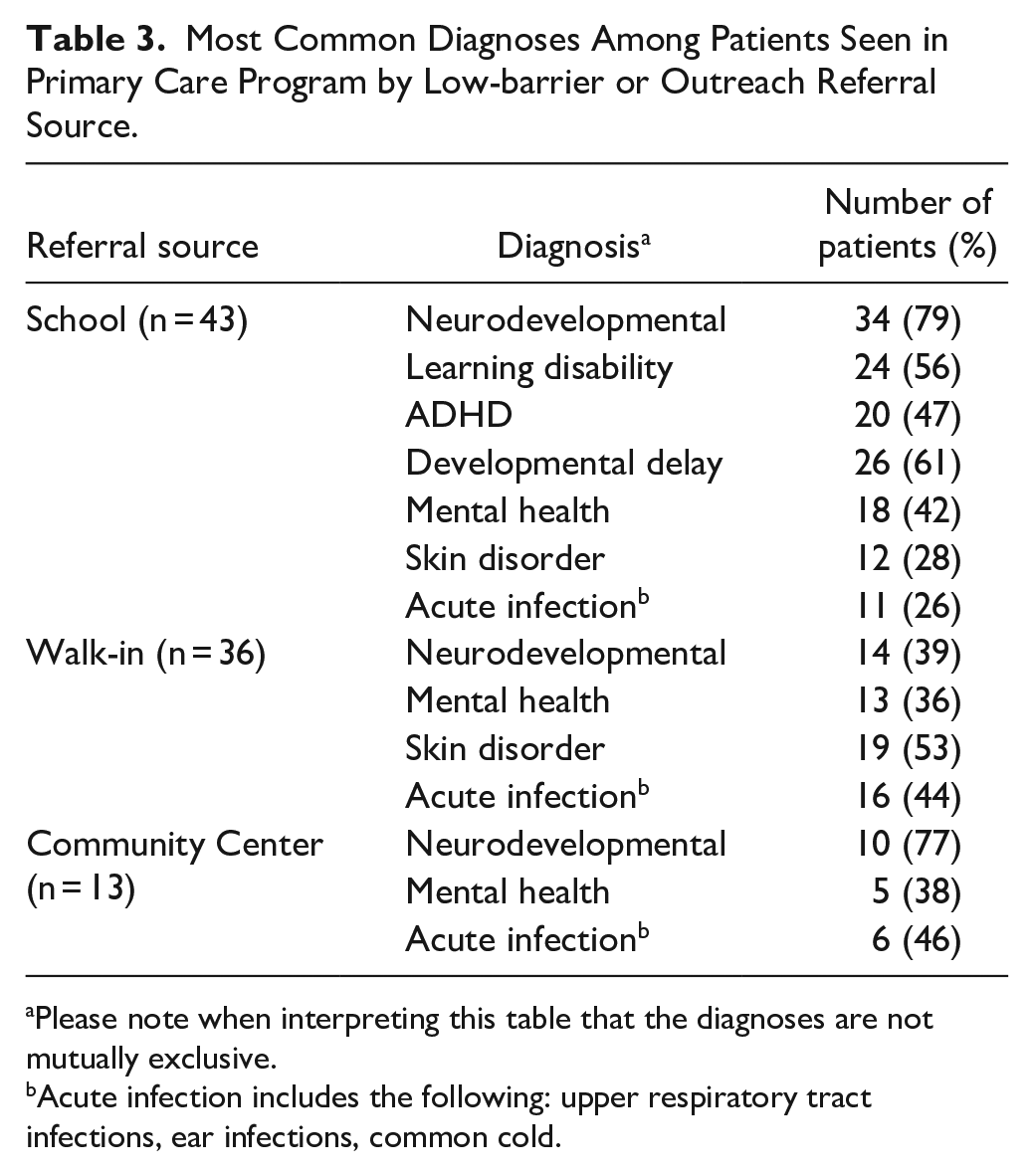
Please note when interpreting this table that the diagnoses are not mutually exclusive.
Acute infection includes the following: upper respiratory tract infections, ear infections, common cold.
Discussion
This study describes the patient population seen by a single inner-city, low-barrier, place-based social pediatric integrated primary-specialty care program. The program utilizes the previously published RICHER model, including a place-based clinic in a housing complex and community-based outreach. 4 It importantly identifies the value of low-barrier, social-justice oriented clinical programs in facilitating care access for children with significant health complexity. Patients most commonly accessed the program through referrals from school (20%), community centers (6%), or from self-referral (17%). An additional 33% had no documented referral source, which in our program’s experience suggests an informal process either directed by the family or a non-clinical community organization. By (1) having clinicians practice in venues identified by community-based organizations as trusted by families and (2) community partners referring children who may not otherwise seek care, the program is able to see children who may be missed, overseen, or disadvantaged through traditional models of care.
At least 1 adverse SDoH was documented in 41% of patients’ medical records. This is likely an underestimate, as not all clinicians routinely comment on unmet social needs during encounters, and this review relied upon clinician documentation to complete the case reporting form. Importantly, in 21% of the children studied, a social challenge (eg, inadequate material resources, involvement of child welfare services, and housing insecurity) was one of the main concerns for which they sought support from the clinic. This demonstrates that social pediatric programs are a viable entry point to support families with unmet social needs. This is particularly important given the high proportion of the patients belonging to populations that face structural inequities.
Children in our program reviewed in this study were currently in or had experienced foster care 11.5 times more than the provincial average. 32 This population is documented to experience higher rates of mental and developmental health challenges.33,34 Taken together, we believe that a low-barrier social pediatric program may mitigate some potential health risks for this population through connection to health services.
In keeping with our hypothesis, the social pediatric clinic’s patients reviewed in this present study were medically complex.1 -4,24,25 The mean number of medical diagnoses per patient was 4.5. Half of the patients had neurodevelopmental concerns (ie, ADHD, learning disability, developmental delay, autism spectrum disorder, and FASD) and a third had mental health concerns (ie, anxiety, depression, and PTSD). The prevalence of mental, behavioral, or developmental disorders in the patients studied is significantly higher compared to the general pediatric population; in the US, studies have estimated around 17% are diagnosed with such conditions. 33 This is in keeping with existing research that found low household or neighborhood socioeconomic status predicted diagnosis of neurodevelopmental disorders in childhood, as well as the severity of its presentation.24,25,35 -37 Again, this speaks to the opportunity of low-barrier social pediatric programs in providing care to children with substantial complexity.
About 79% and 77% of children referred from schools and community centers respectively ended up receiving a neurodevelopmental diagnosis, compared to only 39% of children who were self-referred. This illustrates that staff in schools and community centers are able to identify developmentally vulnerable children and appropriately make referrals to community services. It highlights the importance of working closely with community partners trusted by families for place-based programs that are serving marginalized populations. Previous studies have demonstrated that integrating community partnerships within a clinic or hospital can lead to greater success in addressing poverty’s upstream root causes while connecting patients to resources that mitigate poverty’s harmful downstream consequences.38 -40
For management of these medically and socially complex children, it is important to make timely referrals to subspecialty care, and to help them navigate available community resources. Seventy two percent of patients seen by nurse practitioners in the primary care program required involvement of general and/or subspecialty pediatricians within the clinic. This highlights the importance of providing an effective link between service providers and demonstrates that the RICHER social pediatric model improves access to enhanced care for children with complex medical and social needs. Patients were most commonly referred for complex developmental assessments (34%), mental health services (35%), and to general pediatricians (26%). The program plays a crucial role in assisting with care coordination and ensuring patients are not lost in follow-up with sub-specialists. Relationship-based primary care providers can refer patients to specialty services and provide a reliable foundation where specialists can direct instructions for ongoing management, screening, and long-term follow-up.
A limitation of the study is that the number of patient charts reviewed was based on convenience due to limited personnel available for data collection. As such, our results may not be generalized to the greater population seen by the program. Another limitation is the inconsistency in documentation; for example, 28% of patients had unspecified ethnicity, while 54% had an unspecified referral source. The gaps in the charts may be, in part, due to families and patients not disclosing demographics such as their ethnicity and/or gender identity due to histories of personally facing discrimination based on these factors in the healthcare system as well as intergenerational trauma.26,27 Providers may not ask about subjects such as immigration status, history of incarcerated caregivers, or history of caregiver substance use in the household in order to foster trusting therapeutic relationships and establish longitudinal care. Implementing a standard intake form with community and elder guidance for the program is a planned next step from this project, that will help improve routine sociodemographic data collection amongst different clinicians. Future community-based participatory research should guide and support clinicians on how to best collect information while building rapport and building trust. This information could then be used in future quality improvement projects to inform resource allocation and outreach efforts. Further research should be done to study the long-term health outcomes of children and youth from other disadvantaged neighborhoods and communities who have accessed similar low-barrier medical care compared to those who did not.
Conclusion
The patients and families seen by the low-barrier, place-based primary care clinic using the RICHER social pediatrics model were both medically and socially complex. Our results suggest that the program sees a diverse population that is disproportionately impacted by adverse SDoH. Referrals to general and/or subspecialty pediatricians from primary care nurse practitioners were often indicated, highlighting the level of medical complexity in the population seen. The integration of primary care with subspecialty care in the RICHER model supports the delivery of enhanced care that is often indicated in children who are developmentally vulnerable as a result of adverse SDoH. By allowing for self-referrals, providing care for the whole family, and partnering with community members who can identify developmentally vulnerable children, greater access to care was made available for structurally marginalized families.41 -43 By building relationships with families and community partners through family-centered, trauma-informed, and culturally-sensitive care, longitudinal care and trust in the healthcare system can be fostered. This allows for preventative care, navigational support within the healthcare system, and positive health outcomes for developmentally vulnerable children and youth historically overlooked or excluded in traditional models of care.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319241273284 – Supplemental material for Facilitating Access to Care for Children With Complex Health Needs Through Low-Barrier Place-Based Intake Processes: Lessons From the RICHER Social Pediatric Model
Supplemental material, sj-docx-1-jpc-10.1177_21501319241273284 for Facilitating Access to Care for Children With Complex Health Needs Through Low-Barrier Place-Based Intake Processes: Lessons From the RICHER Social Pediatric Model by Judy So, Sunny Sun, Annie Kim, Saina Nemati, Michelle M. Kim, Gwyneth McIntosh, Kristina Pikksalu, Christine Loock and Matthew Carwana in Journal of Primary Care & Community Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.