
Abstract
Purpose:
This pilot study tested the feasibility and acceptability of a pragmatic randomized trial evaluating group-based non-pharmacologic approaches to increase access in primary care and improve pain-related outcomes.
Methods:
This 2 × 2 factorial trial assessed two 12-week interventions: group acupuncture and integrative group medical visits (IGMVs). Adults with chronic pain lasting ≥3 months were enrolled from safety-net primary care clinics. Participants were randomized to group acupuncture, IGMVs, both, or neither (usual care). We analyzed data using linear mixed models, ANCOVA, and abductive qualitative analysis.
Results:
Overall, 44 participants were randomized (25 English-speaking and 19 Spanish-speaking); 59% were female (mean age = 55 years), 21% African American or Black, 52% Latine, 21% non-Latine White, and 5% more than 1 race; and 78% had annual income <$25 000. At baseline, the average duration of chronic pain was 13.0 years, and the mean pain impact score was 36.0 (SD = 6.4). Participants randomized to interventions attended 6 of 12 sessions on average; 89% would participate again; and 86% reported clinically relevant pain improvements versus 20% in usual care (P < .001). Qualitative data revealed substantial barriers to accessing multimodal care and social benefits of group-based models.
Conclusion:
Group-based integrative pain management is feasible and acceptable when co-located within safety-net primary care.
Introduction
Clinical guidelines recommend a multimodal approach to chronic pain treatment, including non-pharmacologic therapies.1,2 Numerous challenges impede guideline-concordant care in primary care safety-net clinics serving low-income patients with chronic pain, including the length of primary care visits 3 and the lack of insurance coverage for many non-pharmacologic therapies. 4
Established group-based approaches to chronic pain management include group acupuncture and integrative group medical visits (IGMVs), both of which provide simultaneous treatment to multiple patients in a shared space. Group acupuncture lowers costs and improves treatment access,5,6 without compromising patient perceptions of quality of care. 7 In previous research with patients from primary care safety-net clinics, group acupuncture was associated with improvements in pain severity, pain interference, and depression in a quasi-experimental study, 8 and with reduced chronic pain and improved physical function in a randomized clinical trial. 9 IGMVs combine clinical care, including non-pharmacologic therapies, with health education and peer support. 10 IGMVs provide extended visit time and increase access to multimodal care.11,12 IGMVs for chronic pain confer multiple benefits, including decreased pain interference, increased self-efficacy, 11 improved quality of life,13-15 lower healthcare utilization,12,16 and reduced opioid use.12,17
Social determinants of health, including stigma, racism, and social isolation, profoundly impact pain outcomes18-23 but are inadequately addressed in clinical care. Social isolation and pain-related stigma have led to dire consequences, including unmanaged pain and overuse of opioids.17-18 The potential benefits of addressing social factors in pain are understudied. Group-based pain management may fill a significant gap in current pain care by incorporating the “social” aspects of a biopsychosocial approach. Studies of IGMVs have found interpersonal-level benefits, such as decreased social isolation, increased social support, and improved patient-clinician relationships.24-27 The presence of peers may reduce discriminatory or stigmatizing practices by clinicians. 28 The San Francisco Department of Public Health implemented a 12-week Integrative Pain Management Program offering multimodal pain management using a biopsychosocial approach. This program includes IGMVs with pain education, social support, and mind-body approaches (meditation and yoga), group acupuncture, and other non-pharmacologic treatments. In a quasi-experimental study, the program was associated with decreased pain interference, increased pain self-efficacy, and social support. 11 Qualitative findings highlighted pain relief through social connection with group members and feeling understood by others who experienced stigma. 26
This mixed-methods pilot study aimed to assess the feasibility and acceptability of a pragmatic randomized trial of the program’s group-based components in Spanish and English, in preparation for a larger trial to assess whether acupuncture, IGMVs, or both account for observed benefits in participants.
Methods
Study Design
This pilot pragmatic randomized trial used a 2 × 2 factorial design. The 2 treatment factors were 12 weekly sessions of group acupuncture, and 12 weekly sessions of an IGMV, with half assigned to each factor and half assigned to the absence of the factor. Participants were randomized into 4 equal study arms: (1) group acupuncture, (2) IGMV, (3) concurrent participation in both acupuncture and IGMV, and (4) assignment to neither condition (ie, usual care, with the option to receive acupuncture after study participation), as described in detail elsewhere. 29 This study was approved by the University of California San Francisco (UCSF) Institutional Review Board (#22-37078).
Study Procedures
We recruited patients in safety-net primary care clinics that are part of the San Francisco Health Network (SFHN). The inclusion criteria included age ≥18 years, fluency in English or Spanish, empanelment to an SFHN primary care provider, a diagnosis of chronic pain lasting ≥3 months, ability to provide a phone number, ability to participate in groups, and expected availability for 24 weeks. The exclusion criteria were active cancer treatment or inability to provide informed consent.
We assembled a team with substantial experience recruiting and retaining racially and linguistically diverse patients in safety-net clinics. We presented the study to primary care teams and individually contacted clinicians to solicit patient referrals. Bilingual research assistants (Spanish/English) conducted recruitment via phone calls, invited participants to study orientations, and obtained informed consent. Written materials were available in English and Spanish. Following the consent process, a 45- to 60-min baseline assessment was administered. Participants were randomized to 1 of the 4 conditions using a computer-generated list with randomly permuted blocks of 4 and 8, stratified by language.
Study retention efforts included weekly follow-up from a known study team member via phone call and/or text message based on participants’ preferences. Intervention sessions aimed to create a welcoming environment, with consistent staff and flexibility for participant needs (eg, late arrivals and modifications to physical movement). Given the high symptom burden and low incomes of most participants, providing food at study visits was an important part of retention. Participants received gift card incentives.
Measures
We assessed the feasibility of study procedures, including enrollment and randomization, intervention attendance, and survey completion at baseline and 3-month follow-up. We examined the acceptability and impact of interventions on patient experiences with pain management, patient-clinician relationships, and clinical care using participant satisfaction surveys, open-ended questions, interviews, focus groups, and participant-observation of interventions. 29
Quantitative
We included measures recommended by the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials 30 and the National Institutes of Health (NIH) Helping to End Addiction Long-term® (HEAL) Initiative Common Data Elements. We measured pain impact, which is based on 9 items in the NIH Patient-Reported Outcomes Measurement Information System (PROMIS) and yields scores ranging from 8 to 50. 31 We measured pain intensity using the PROMIS Pain Intensity instrument, which is a single-item measure with scores ranging from 0 to 10. We measured pain interference using the PROMIS v1.1 Pain Interference 8a instrument (converted to T-scores with a mean of 50 and a standard deviation [SD] of 10 points in reference populations) and the Patient Global Impression of Change questionnaire (a 7-point Likert scale). We measured depression using the Patient Health Questionnaire-2 (PHQ-2) and anxiety using the General Anxiety Disorder-2 (GAD-2), both with scores ranging from 0 to 6. 32 We included the PROMIS v1.2 Global Health and PROMIS v2.0 Physical Function 6b measures (converted to T-scores).33,34 We evaluated social support in chronic pain using a 6-item scale, with scores ranging from 0 to 24 35 ; social isolation using the PROMIS Social Isolation 8a T-score 36 ; internalized stigma in chronic pain using a 28-item scale, with mean scores ranging from 1 to 4 37 ; pain self-efficacy using a 10-item scale, with scores ranging from 0 to 60 38 ; and perceived discrimination using the Intersectional Discrimination Index, a 7-item scale, with scores ranging from 0 to 28. 39
Qualitative
All participants were invited to participate in a semi-structured interview at 3-month follow-up. Interview guides were developed to explore participant experiences in each study arm, the impact of study participation on chronic pain management, and broader topics related to life with chronic pain, including social support and isolation, stigma, discrimination, and ideal healthcare. IGMV participants were also invited to participate in a focus group. Trained researchers observed IGMV and acupuncture sessions at weeks 1, 6, and 12, and took structured notes on what occurred during the sessions, including interactions among participants and clinicians and discussions related to social isolation, stigma, and support or belonging.
Data Analysis
Quantitative
Sociodemographic data and baseline patient-reported outcomes were summarized. Feasibility and acceptability metrics were analyzed by computing rates of retention and enrollment as percentages.
As a feasibility pilot, we analyzed clinical outcomes to make a preliminary assessment of the strength of intervention effects, identify potential issues with missing data or skewed distributions, and refine the statistical analysis plan. Analyses included changes from baseline to week 12 within treatment groups and between groups with and without each treatment factor, examining acupuncture versus no acupuncture and IGMV versus no IGMV.
Within-group effects were estimated using linear mixed models, with indicators for assignment to acupuncture and IGMV, timepoint (baseline or follow-up), and interactions between each treatment indicator and time. Models included language as a covariate, and a random intercept for correlation of repeated measures. Between-group treatment effects were estimated using analysis of covariance (ANCOVA), which included baseline scores as a covariate to account for possible group imbalances at baseline. Models had indicators for assignment to acupuncture and IGMV and included a covariate for language.
Qualitative
Interviews and focus groups were audio-recorded and professionally transcribed. We used established qualitative methods, including an abductive approach to flexible coding of data to generate index codes that were both deductive and inductive.40,41 All qualitative data were coded by 2 trained researchers using Dedoose software, with ongoing team discussions to clarify any coding disagreements. Further analysis for this manuscript focused on identifying connections between quantitative and qualitative findings. We linked sociodemographic data and baseline patient-reported outcomes with qualitative data to facilitate mixed-methods integration.
Results
Study Participants
We received 160 referrals for the study; 116 individuals were excluded because they were uninterested in participating, could not be contacted, or were ineligible (Figure 1). We consented and randomized 44 participants (25 English-speaking and 19 Spanish-speaking). Of these, 20% identified as Black or African American, 52% as Latine, 20% as non-Latine White, and 5% as more than 1 race. The mean age of participants was 55.2 years (SD = 14.0). Most had not completed a 4-year college degree (86%), were not employed (73%), and had an annual household income of <$25 000 (78%; Table 1). Study participants had substantial health challenges: they had experienced chronic pain for an average of 13.0 years (SD = 9.7). The mean pain impact score at baseline was 36.0 (SD = 6.4). Additionally, the majority of participants (66%) had 3 or more chronic conditions.

CONSORT diagram.
Characteristics of Randomized Study Participants (n = 44).

The disability insurance pain indicator was missing for n = 1 participant.
Pain duration at baseline was missing for n = 4 participants.
Other medical problems listed by participants included: anxiety, brain tumor, neuropathy, pinched nerves, epilepsy, spinal stenosis, osteoporosis, osteopenia, HIV, endometriosis/pelvic pain and multiple other pain conditions.
Feasibility of Study Procedures
Overall, 12 participants were randomized to usual care, 11 to acupuncture, 11 to IGMV, and 10 to both acupuncture and IGMV. Among participants randomized to an intervention, 94% attended at least 1 session. Participants randomized to acupuncture attended an average of 6.4 sessions, and participants randomized to IGMV attended an average of 6.0 sessions. Follow-up surveys and interviews at 3 months were completed by 39 of 44 participants (89%).
Staff were available at all visits to support patients with limited literacy to read consent forms and complete surveys. Over 75% of Spanish-speaking participants and 50% of English-speaking participants requested staff assistance with survey completion for reasons related to pain and other symptoms, limited literacy, or a lack of familiarity with technology.
Study Acceptability
Participant satisfaction was assessed post-intervention (Table 2). At least 89% of intervention participants said they would participate in the program again and recommend it to others. Among IGMV participants queried about specific aspects of the program, 89% or more reported satisfaction with each aspect.
Participant Satisfaction and Experience.

Abbreviation: IGMV, integrative group medical visit.
Regarding randomization, 12% of study participants indicated that they were disappointed with their group assignment. Disappointment was proportionally higher among participants randomized to usual care (n = 3, 30%) and acupuncture only (n = 2, 20%) compared with those randomized to IGMV (n = 0). Among those randomized to neither intervention, reasons for disappointment included not being able to contribute more to science and not getting to interact more with the diverse research team, while 1 participant looked forward to accessing acupuncture after completing data collection. One participant who received acupuncture expressed disappointment in not being able to participate in the group mindfulness aspect of the IGMV.
Chronic Pain Experiences
Participants consistently described bidirectional relationships between pain and overall quality of life, including social factors, in interviews, focus groups, and observations of treatment sessions (Table 3). When pain was interfering less with daily life, participants found it possible to connect with neighbors and family members and to consistently engage in health behaviors likely to benefit pain (eg, movement, healthy eating, and mind-body practices). In turn, these kinds of support and daily practices often helped participants’ pain.
Summary of Within-Factor Effects from Integrative Group Medical Visits and Acupuncture.

Abbreviation: CI, confidence interval; GAD-2, Generalized Anxiety Disorder-2; PHQ-2, Patient Health Questionnaire-2; PROMIS, Patient-Reported Outcomes Measurement Information System.
The top portion of each subtable includes measures for which a score decrease shows improvement, whereas the lower portion of each subtable includes measures for which a score increase shows improvement.
From baseline to post-intervention at 3 months, the mean pain impact score among participants receiving acupuncture decreased by an average of −6.2 (95% CI = −9.5, −2.9). The mean pain impact score decreased by −3.7 (95% CI = −5.9, −1.6) among IGMV participants (Table 4). Notably, the minimal important change in pain impact has been estimated to be a 3-point decrease. 42 Additionally, the mean pain interference, global physical health, and physical function scores improved among participants receiving either intervention.
Exploratory Analyses of Main Effects of Acupuncture and Integrative Group Medical Visits (IGMVs) a .

Abbreviations: IGMV, integrative group medical visit; CI, confidence interval; GAD-2, Generalized Anxiety Disorder-2; PHQ-2, Patient Health Questionnaire-2; PROMIS, Patient-Reported Outcomes Measurement Information System.
Mean differences are estimated using separate ANCOVA models for each outcome listed. The dependent variable for each model was the outcome at follow-up, with indicators for each treatment type (acupuncture and IGMV) as the independent variables, and controlling for the baseline value of the outcome and for language. Effects indicate the difference in change in outcome at follow-up between participants assigned to the listed treatment versus participants not assigned to the treatment, averaged over the other treatment type (in this 2 × 2 factorial trial). Note that this is a main effects analysis and assumes no interaction between the 2 treatments (no interaction term was included in these models). The top portion of the table includes measures for which a score decrease shows improvement, while the lower portion of the table includes measures for which a score increase shows improvement.
Indicates mean differences with P < .10.
Indicates mean differences with P < .05.
We conducted exploratory analyses using ANCOVA to inform the development of our larger study (Table 4). Based on the residualized change from the ANCOVA model, participants who received acupuncture had a 5.2-point greater decrease in their pain impact score at the 3-month follow-up (95% CI = −9.9, −0.6) compared with participants who did not receive acupuncture, controlling for IGMV participation. Using a Fisher’s exact test based on dichotomizing the Global Impression of Change assessment (any improvement vs no change or worsening of symptoms), 86% of participants randomized to a study intervention reported clinically relevant pain improvements compared with 20% of participants randomized to usual care (P < .001).
Social Support, Isolation, and Stigma
Our mixed-methods analysis indicated promising findings related to social support, stigma, and social isolation (Table 5). In interviews and focus groups, several participants shared that they expected to feel “like a guinea pig” while participating in research, but instead experienced the study as the best healthcare they had received. In observations, we noted that IGMV facilitators cultivated a supportive environment, encouraging interactions among peers and modifying therapeutic movement and mind-body practices to accommodate different physical capabilities and preferences for participation. Although acupuncturists did not specifically encourage participant interaction, participants in some group acupuncture sessions spoke to each other at length before and during treatment.
Case Examples of Participant Experiences.
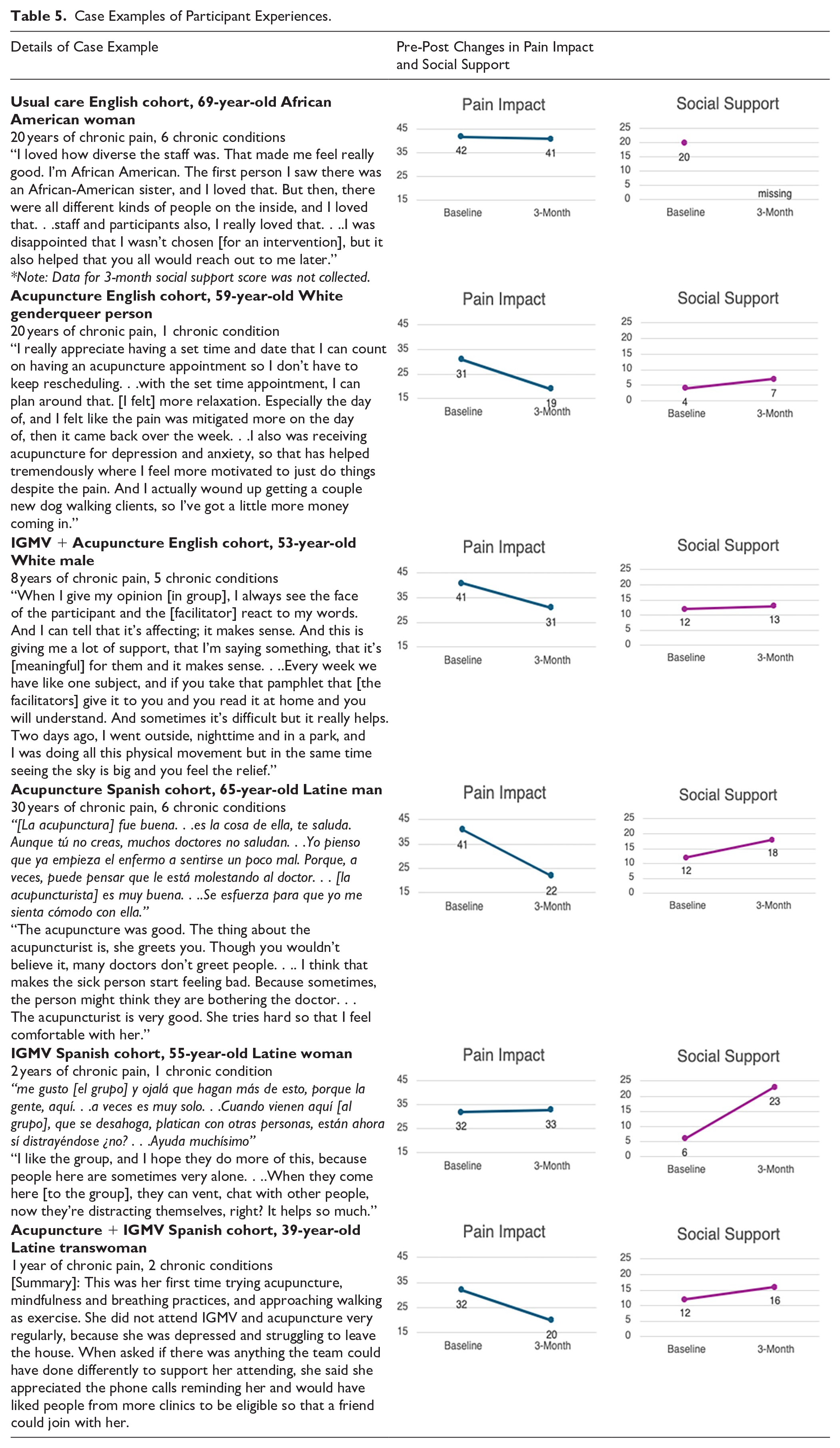
Across intervention arms, participants described how consistent relationships with study team members reduced their social isolation. IGMV participants generally experienced group visits as a supportive environment, in which clinician-facilitators were “on our level.” Many were new to spending time in a group of people living with chronic pain and found their peers to be understanding and encouraging, providing emotional support and practical support for coping with chronic pain (Table 5). Additionally, some participants in each intervention arm shared that improvements in pain and related symptoms allowed them to strengthen their relationships with family, neighbors, and friends.
Participants in all study arms described intersectional stigma in and outside of healthcare settings, which they viewed as related to their pain, as well as other identities (language, socioeconomic status, actual, or perceived substance use). Participants described stigma as substandard care including delayed or inaccurate diagnoses, confusion and tension about pain treatment, and lack of follow-up. Many IGMV participants found that group participation reduced internalized and pain-related stigma. They spoke about benefits of hearing others describe coping with pain, and appreciation for learning new mind-body skills (mindfulness and therapeutic movement) alongside peers. Study team members responded to higher-than-anticipated rates of suicidal ideation and grief after recent family deaths. We referred patients for ongoing mental health care, acupuncture, and other resources. Most participants said they would like to continue receiving care from study clinicians (90%). From baseline to post-intervention, social support for chronic pain increased by an average of 3.9 (95% CI = 0.8, 7.0) on a 24-point scale among IGMV participants. Mean scores for depression and anxiety improved among participants who received acupuncture; anxiety scores improved among IGMV participants (Table 4). Based on the residualized change from the ANCOVA model, IGMV participants had a 3.7-point greater increase in social support for chronic pain compared with participants not randomized to IGMV (95% CI = 0.2, 7.2), controlling for acupuncture participation.
Discussion
We conducted a pilot study of group acupuncture and IGMVs, co-located within safety-net primary care clinics. We tested all research procedures and implementation in English and Spanish in preparation for a larger trial. The results demonstrate feasibility and acceptability of a randomized pragmatic trial in this setting, in ongoing partnership with safety-net clinicians. Mixed-methods data collection provided opportunities to explore experiences of stigma and social support, important social factors in chronic pain that are insufficiently captured through quantitative measures (Table 5).43,44
This study used best practices to support recruitment and retention of a racially and ethnically diverse population in Spanish and English.45-47 Study participants were representative of the clinic where the program was offered and included slightly higher percentages of Black and Latine patients and lower percentages of Asian American and White patients than the overall SFHN patient population. Within a long-standing community-academic partnership, our research team combined multiple strategies to address social factors in chronic pain, with the goal of minimizing stigma and providing social support from peers and clinicians facilitating group-based care.
Group-based integrative pain management may be an effective approach to increase access to guideline-concordant pain care. Specifically, group-based approaches can target “social” aspects of biopsychosocial pain care by providing social support for coping with chronic pain and reducing pain-related stigma.48-50 These social factors are complex and interconnected, but notable shifts occurred for many participants in the 12-week program. Our mixed-methods findings affirm the benefits of continuity of care, peer relationships with others who have chronic pain, and supportive interactions with clinicians and peers. Social support is multi-faceted, and participants described increased social support in daily life and within the program, which aligns with prior findings on group visits.14,15 Pilot data support the expanded use of group-based care to increase access to multimodal treatment, address time constraints that contribute to disparities in pain management, and foster social connectedness and belonging. Because this pilot study was designed to test feasibility and was not powered for effectiveness, we report between-group analyses for transparency but cannot draw inferences from them. However, in within-group analyses, the direction of change suggests improvement across a range of patient-reported outcomes, and preliminary estimates from between-group exploratory analyses were overall consistent with support for these programs.
Group-based treatment is offered in a growing number of community health centers and other settings and provides a feasible way to increase access to care while providing multiple social benefits. Future research should explore approaches to multimodal care in primary care settings. We are currently conducting a large, randomized trial of IGMVs and group acupuncture, offering usual care participants the option to choose an intervention after 6-month follow up. 29 This study tests the hypotheses that assignment to group acupuncture or IGMV will improve pain outcomes and social support in participants with chronic pain. Additionally, we are evaluating multilevel effects of increasing access to multimodal pain care in a network of safety-net primary care clinics.
The United States has a long history of inequity in chronic pain care, with racism, economic segregation of health care, and gender-based discrimination shaping who has access to guideline-concordant pain care. 51 Opioid prescribing in primary care and elsewhere has notably decreased in recent years, without corresponding investments in guideline-concordant, multimodal chronic pain care.52,53 Widespread access to guideline-concordant care is an important form of institutional repair given the common undertreatment of chronic pain among Black and Latine individuals, women, and individuals with low incomes.18-20 Safety-net primary care clinics are a key setting for growing efforts to increase equitable access to group-based, biopsychosocial care.54,55 Now that treatment guidelines recommend a pain management approach that is both biopsychosocial and multimodal, including non-pharmacologic therapies, commitment is required to ensure a shift toward equitable care.
Footnotes
Acknowledgements
The authors thank the many people who have contributed to the San Francisco Health Network’s Integrative Pain Management Program (IPMP), including the IPMP Steering Committee, integrative health practitioners, primary care and behavioral health clinicians, San Francisco Department of Public Health primary care leadership, research staff, study consultants, and all the patients who have participated in the program. Special thanks to the pilot study clinicians and research team: Melissa Craven, LAc, Victoria Garcia Drago, BA, Annika Hansen, MA, Sudha Prathikanti, MD, Vadan Ritter, LAc, Nakarí Ron, LCSW, Denise Ruvalcaba, BA, Naomi Schoenfeld, MS, PhD, and Antonella Soldaini, LAc. We also thank the Castro-Mission Health Center leadership and staff, especially Keith Seidel, MD, and Lilibeth Morales, MBA.
Author Note
Ethical Considerations
This study was approved by the University of California San Francisco (UCSF) Institutional Review Board (#22-37078) on August 2, 2022.
Consent to Participate
All participants provided written informed consent prior to participating.
Consent for Publication
Not applicable.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the HEAL Initiative Advancing Health Equity in Pain Management Program, National Institute on Minority Health and Health Disparities (NIMHD) and the National Institute of Neurological Disease and Stroke (NINDS) of the National Institutes of Health (NIH) under Award Numbers R61MD018333, R33MD018333, and K01MD015766.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data and data collection tools from this study are available by request, and will be available through the ICPSR data repository.