
Abstract
Background
Chronic pain is a global problem affecting approximately 20% of adults. The prevalence of opioid use for chronic pain has contributed to a widespread crisis of addiction and inadequately managed pain. Though national and international guidelines recommend nonpharmacological, integrative, multi-modal therapies for chronic pain, numerous systemic barriers limit access to these services for those with the highest need and fewest resources.
Objective
This paper describes the development and testing of an innovative “Heals on Wheels” (HoW) community engagement and Group Medical Visit (GMV) program for underserved communities experiencing chronic pain in Hennepin County, Minnesota.
Methods
The HoW program’s curriculum was collaboratively adapted from pre-existing Hennepin Health care GMV programs for chronic pain. Free community-based “Appetizer” workshops were developed alongside an 8-week “Full Meal” GMV program titled Easing Pain Holistically (EPH). Three pain-affinity variations of EPH were created (the “Body”, “Head”, and “Heart”) and delivered to 6 cohorts (2 cohorts of each variation). Feasibility was measured by attendance, demographics, and insurance provider information. To evaluate program acceptability, thematic analysis of patients post-GMV weekly progress sheets was performed.
Results
The curriculum for the HoW program included experiential training and education in evidence-based integrative pain management strategies. Fourteen community appetizer workshops (n = 142) were offered in partnership with organizations representing underserved populations. Fifty-five patients completed EPH from 2022 to 2024 with the greatest number of patients in the Heart (n = 23), followed by the Body (n = 19), and the Head (n = 13). Feasibility for the GMV program was demonstrated with average attendance across 6 cohorts at 75.1%. Thematic analysis of qualitative data revealed themes highlighting appreciation for group connection (“sharing”) and the EPH program content.
Conclusion
The HoW program shows promise as a feasible and acceptable model of community outreach and engagement to improve access to evidence-based integrative pain care.
Keywords
Introduction
Chronic pain is a global problem with the prevalence of pain standardized across countries estimated to be 27.5%. 1 Data from the International Association for the Study of Pain shows that approximately 20% of adults in the United States report experiencing chronic pain. 2 Studies that examine various drivers of chronic pain physiology shed light on its multifaceted nature as the prevalence of chronic pain can be due to a variety of diagnoses and mechanisms. 3 Furthermore, research shows that specific communities experience higher rates of and greater negative impacts from chronic pain such as women, 4 Black and/or Hispanic individuals, 5 individuals who have experienced trauma, 6 and/or people with low socioeconomic status. 4 According to a 2023 report from the U.S. Centers for Disease Control and Prevention (CDC), adults with income less than 100% of the federal poverty level (FPL) have a 4 times greater prevalence of chronic pain than those with income greater than or equal to 400% of the FPL. 7 Other risk factors for experiencing chronic pain include comorbidities, chronic stress, poor mental/emotional health, poor sleep, experiences of abuse or social isolation, and unsafe environments. 8
Evidence suggests that opioid medications fail to provide long-term benefits for individuals with chronic pain, 9 but rather carry deleterious side effects and high addictive potential. 10 Historically, opioids have been over-prescribed as a primary treatment for chronic pain, which has contributed to a widespread crisis of both addiction and poorly managed pain. 11 Data from the CDC shows that the drug overdose rate in 2021 was over 6 times the rate in 1999, with over 75% of these involving opioids. 12 Minnesota Department of Health (MDH) data shows a total of 977 opioid-related overdose deaths in Minnesota in 2021, with 340 in Hennepin County. 13 Given the inter-related crises of chronic pain and Opioid Use Disorder (OUD), along with the loneliness crisis precipitated by the COVID-19 pandemic, 14 it is imperative that social drivers of health are addressed alongside evidence-based pain management approaches.
There is a growing body of evidence for nonpharmacological, integrative approaches to chronic pain management. 15 By applying a whole-person, bio-psycho-social-spiritual framework for the complex issue of chronic pain, better outcomes are achieved, including fewer harmful side effects than management involving opioids. 16 The American Medical Association (AMA) pain care task force has emphasized the importance of integrated, multidisciplinary, and multimodal chronic pain care, but recognizes that health care systems rarely support this type of care. 17 Many nonpharmacological, evidence-based interventions may be inaccessible to populations affected by Social Determinants of Health (SDOH). Significant barriers to accessing this care include administrative barriers such as prior authorization requirements and limited to no insurance coverage for some evidence-based services.17,18 People with limited financial resources who also suffer from chronic pain may find these services inaccessible due to out-of-pocket expenses. Transportation is also a barrier for those with limited economic means and for those living in rural areas where fewer nonpharmacological pain care services are available.19,20 Another frequent barrier is the lack of health care provider knowledge in nonpharmacological pain management strategies, as many patients with chronic pain report that their providers do not have adequate information or expertise to offer them nonpharmacological services, resources, or referrals. 18 People who suffer from both chronic pain and addiction may have even fewer nonpharmacological care options, as they may have additional barriers of stigma and/or mistrust in health care institutions due to previous poor treatment by health professionals. 20
Integrative Group Medical Visits (GMVs) are an effective model to potentially eliminate some of these barriers to nonpharmacological evidence-based pain care. GMV’s are a shared medical visit where a group of patients with a common condition or concern meet with a provider in a group format. GMVs are billed to insurance as a typical office visit. GMVs focused on integrative approaches to chronic pain in racially diverse communities have shown improved pain outcomes as well as improvements in depression, stress, quality of life, and sleep.21,22 A study by Jackson et al (2024) suggests that clinicians may also be positively impacted from experiences with integrative GMVs in addition to the health outcomes of their patients. 23 In their study, qualitative interviews of health care staff from safety net health care settings across the United States depicted themes of human-centered engagement, interprofessional team collaboration, and enhanced meaning and purpose to describe how integrative GMVs may improve clinician well-being. Our study aims to describe the development, feasibility, and acceptability of Hennepin Health care System’s (HHS) Heals on Wheels (HoW) community engagement and Group Medical Visit program addressing access and equity through an Integrative Health (IH) approach to chronic pain management in historically underserved populations. A future paper will report qualitative and quantitative outcomes for the GMV associated with the HoW program.
Materials and Methods
HHS is a safety net hospital and clinic system throughout Minneapolis and surrounding areas, largely serving Hennepin County, Minnesota. HHS’s mission is to partner with the community, patients, and their families to ensure access to outstanding care while improving health and wellness through teaching, patient and community education, and research. As the largest safety-net hospital in Minnesota, Hennepin Health care predominantly serves a historically marginalized and under-resourced low-income population, including those who are homeless, incarcerated, uninsured, and underinsured.
The HoW program grew from pre-existing GMV curricula for chronic pain delivered at HHS. Previous programs based in Family Medicine and Internal Medicine respectively called Tame Your Pain (TYP) (2017- present) and Growing Resilience in Chronic Pain (GRCP) (2020-2022), brought nonpharmacological management of chronic pain to patients through an 8-week, 2-hour/week curriculum. Weekly topics included pain neuroscience education alongside information and practices to support sleep, nutrition, stress management, movement, art, and social connection as mechanisms for healing. All sessions included experiences and practices based in IH modalities such as chiropractic, yoga/integrative physical therapy, and acupuncture.
Heals on Wheels (HoW)
Drawing from our experiences with TYP and GRCP, Heals on Wheels was conceived as an innovative model to bring integrative, evidence-based, whole-person chronic pain care directly to communities in need. HHS received grant funding from the Opioid Epidemic Response Advisory Council (OERAC) through the Minnesota Department of Human Services in 2021 to launch the HoW program. The goal of the program was to improve access to holistic chronic pain treatment and self-management strategies to serve as preventative and restorative interventions for people at risk of or experiencing OUD throughout Hennepin County. This study was reviewed by the Hennepin Health Care Human Research Protection Office (HRPO) Institutional Review Board (IRB) and was deemed program evaluation and as such full IRB approval was waived.
The Heals on Wheels program consists of 2 ingredients, community “Appetizer” workshops and a “Full Meal” 8-week GMV series. A community-based Integrative Pain Care (IPC) workshop or “Appetizer” was incorporated into the program with the specific purpose of improving access and reducing barriers to care. By bringing the care directly to communities in need, we ameliorated and/or eliminated access barriers such as transportation, insurance coverage, and other health care costs such as copays or deductibles. The Appetizers also served as a recruitment effort for the GMV program. Various community partner organizations throughout Hennepin County hosted these HoW Appetizer workshops. Partners were chosen through consultation with HHS’s Health Equity department, with priority given to organizations located in under-resourced geographical areas and those with a mission of serving people experiencing disproportionate harm from the opioid crisis. To maximize alignment with these priorities, a grid was created based on Hennepin County neighborhoods identified as high-poverty neighborhoods on 1 axis and populations experiencing disproportionate opioid harm on the other. 24 Potential organizations were identified by the HoW Leadership and Health Equity teams and organized on the grid. The Program Manager contacted each organization and used snowball recruitment methods, receiving more recommendations for partners from the organizations contacted to ensure community representation based on geographic and demographic diversity and need. The community partner organizations coordinated the recruitment for the Appetizers through word of mouth and posting signup sheets and fliers. The community partner organization staff were encouraged to participate in the workshops alongside their community members.
The facilitation team leading the Appetizers included an integrative physician, an integrative physical therapist/yoga therapist, and a community ambassador. The community ambassador was a patient who had participated in GRCP groups with firsthand experience of chronic pain self-management strategies and IH modalities. Additional staff specializing in massage and acupuncture also contributed to Appetizers depending on availability. Appetizer workshops were adapted to variable duration (30-90 min) and format (formal workshops or informal information booths) depending on the hosting organization preferences.
The new GMV series for the HoW program was titled Easing Pain Holistically (EPH) and included 3 pain-affinity variations designed for different populations: “Head” (patients experiencing chronic headaches or brain injury), “Body” (patients experiencing muscle and joint pain throughout their body), and “Heart” (patients interested in exploring the relationship between emotions and chronic pain). These visits were co-facilitated by an integrative physician and an integrative physical therapist; the “Heart” cohort incorporated a third facilitator with a PhD in psychology. By creating 3 distinct pain-affinity variations of the GMV, we hoped to address condition-specific concerns by focusing the teaching and practices offered to the specialized needs of those conditions. We also hoped to create a stronger sense of belonging and community within groups, allowing for the sharing of similar experiences and stories among participants.
The curriculum for Appetizers and Full Meal GMV was developed collaboratively by the 3 integrative physician co-leads, 2 of whom were the leads on the previous TYP and GRCP GMVs, and the integrative physical therapist/IH Program Manager. Past TYP and GRCP curriculum was collaboratively refined and adapted for use in the short Appetizers and the specific cohorts in the new GMV. Additional input from a psychologist specializing in Cognitive Behavioral Therapy (CBT) and the psychology of chronic pain care enriched the Heart GMV curriculum. In the first 3 cohorts, the GMV coordinator had additional training in Healing Touch and offered experiential energy healing services to patients during the didactic portion of the visit. In the final Heart cohort, the new GMV Coordinator was also a massage therapist who offered massages to interested patients during the didactic portion of the visit. The curriculum was refined iteratively, taking patient and facilitator feedback into account for continuous improvement throughout the program.
Participants were recruited for the GMV through the community Appetizer workshops, internal referrals throughout HHS and past IH GMV’s. Each person referred to the GMV received a screening call from the HoW coordinator. Participants were provided with details on the time/location of the visits, parking and directions, and a basic description of the series. They were offered transportation support if needed and questions were answered about insurance coverage for the visits, with patients assured that the visits would be covered in the same way as a primary care medical visit. Eligibility criteria included: English language proficiency, >/ = 18 years old, interest in nonpharmacological pain management strategies, and willingness to participate in a shared medical visit. Patients were considered ineligible if they had active/untreated addiction or serious psychiatric diagnosis (ie, psychosis or personality disorders) and if their schedule did not permit them to attend at least 6 of the 8 sessions. Participants were screened for the presence of chronic pain; however, we did not exclude anyone from the group based on a specific baseline pain score. This study aimed to establish the HoW curriculum and structure for optimal delivery and accessibility, alongside program feasibility and acceptability as outcomes. Feasibility was measured through attendance at the Appetizer workshops and attendance, demographic, and insurance provider information at the GMV. Patients were considered enrolled in the HoW program if they attended at least 1 GMV. Retention was defined as the percentage of participants that remained enrolled in the HoW program for their 8-week GMV series. Feasibility benchmarks for the GMV were set at a minimum of a 75% attendance average for each session, at least 75% of attendees attending 6 or more sessions, and a retention rate of greater than 75%. This paper focuses on the pedagogical and methodological process of an integrative health program for nonpharmacological pain management. As such, we utilized weekly progress sheets to elicit information that was iteratively used by the clinician to progressively address the needs of individuals. In addition, information collected from these weekly progress sheets was evaluated in conjunction with clinical measures through a mixed-methods approach. While it is beyond the scope of this paper to report on the complete set of outcomes, acceptability and pain ratings provide important feedback and can guide future programming. We utilized systematic content analysis first using direct content analysis and then applying a thematic analysis to identify patterns.25,26 Furthermore, pain ratings (0 = no pain, 10 = worst) were collected and analyzed using Microsoft Excel. To understand the pain at baseline, pre-session pain ratings were averaged.
Acceptability of the GMV was measured through qualitative self-assessment weekly progress sheets completed by patients at the end of every session asking “What portion(s) of the group visit did you like the most?“ and “Any suggestions for improvement or other topics?”. Additional quantitative and qualitative outcomes from HoW will be reported in a future paper.
Results
Appetizers
A total of 14 Appetizer workshops, in partnership with various community organizations, served a total of 142 participants between 2022 and 2024. Community partners hosting the appetizers included low-income, assisted living (1), and women’s transitional/recovery housing (1) and homeless shelters (1), recovery centers (1), HIV + housing (1), farmers markets/food shelves (3), and community advocacy organizations serving Indigenous populations (1), immigrants/refugees (2), BIPOC communities (2), and survivors of sexual violence (1).
Curriculum for Heals on Wheels Appetizer Workshops.

Full Meal
Easing Pain Holistically GMV Series Attendance and Demographics.

Easing Pain Holistically GMV Topics for Each Cohort.

The curriculum for EPH included diverse IPC strategies and practices. These included education and practices around lifestyle, including anti-inflammatory and mindful eating skills, sleep hygiene and cognitive behavioral strategies for sleep optimization, movement and pacing strategies for pain, and stress management strategies based in nervous system regulation and relaxation practices. Sessions also included pain science education and cognitive behavioral strategies for pain management. While there were common themes and elements to each cohort, the curriculum was adapted for the specific needs of each cohort. For example, in the Head cohort, we used low lighting and frequent breaks to minimize triggers and fatigue. In the Heart cohort we included a session on thoughts and emotions and weekly CBT homework opportunities were woven into the curriculum. Movement practices for each group were also tailored, with more movements to decrease neck and jaw tension in the Head cohort. Social connection exercises such as personal sharing and guided discussion were encouraged throughout. These included a recognition of group norms ensuring respectful and supportive behavior, icebreaker question prompts to solicit group connection, small and large group discussion prompts, and invitations to share personal experiences on the topics presented.
Complementary and IH practices were included throughout. Each cohort included mindfulness meditations and yoga-based movement at every session and a single session dedicated to acupuncture. Three of the 6 cohorts received a session dedicated to chiropractic care, healing touch was offered at 3 cohorts, and massage was offered during 1 cohort.
Minor adjustments were made to the curriculum throughout the project based on patient and facilitator feedback. For example, in the first 3 cohorts, patients reported wanting more time to explore the relationship between nutrition and pain. In response to this, an additional session on nutrition was added to the second round of Head and Body cohorts. Starting with the third cohort, a decision was made to eliminate the chiropractic session. This decision was based on the facilitators’ observations that the content on posture provided by the chiropractor could be incorporated by the physical therapist facilitator during movement breaks throughout the series. This allowed room for the thoughts and emotions session with the Heart cohort and for the additional nutrition session with the subsequent Head and Body Cohorts. (Table 3) Based on the experience of teaching the first 2 cohorts during the movement and yoga session, an additional topic of pacing was added to the third and subsequent cohorts.
Full Meal GMV Participants
Three pain-affinity variations of the EPH curriculum were piloted with a total of 66 participants enrolled in the HoW program across the 6 cohorts, of which 55 completed their self-selected 8-week GMV series and 11 withdrew from the program. The retention rate was calculated to be 83.3%, exceeding the program’s benchmark for feasibility. Of patients that completed the program, demographic representation included 70.9% of participants identifying as White, 25.5% as Black, and 3.6% unknown (Table 2). The average age was 57.6 years old (ranging 24-83) with a median age of 61. Most of the participants identified as women (80.0%), with 12.7% identifying as men, and 7.3% identifying as nonbinary. Demographic information for patients that withdrew from the program (n = 11) is listed in Table 2. Participants’ initial average pain rating scores (0-10) that were reported at the beginning of each group session was 5.7. An analysis of payor mixes revealed that 79.9% of visits were billed to public insurance (Medicare, Medical Assistance, and MN Senior Health Options) with the remaining visits billed to private insurance. Participants were recruited during Appetizer workshops, from previous GMV participants, and through referrals throughout the HHS system. Free Lyft rides were offered to all participants who requested transportation support to and from the GMVs and 20.0% of participants utilized this service.
Qualitative Acceptability Outcomes for Easing Pain Holistically GMV.

Note. Themes derived from qualitative weekly sheets of open journal responses to the prompt: “What portions of the group did you like the most?”
aYear 1 of the HoW program occurred in 2022-2023. Year 2 occurred in 2023-2024.
Themes of Participant Suggestions on Content per Week for Easing Pain Holistically GMV
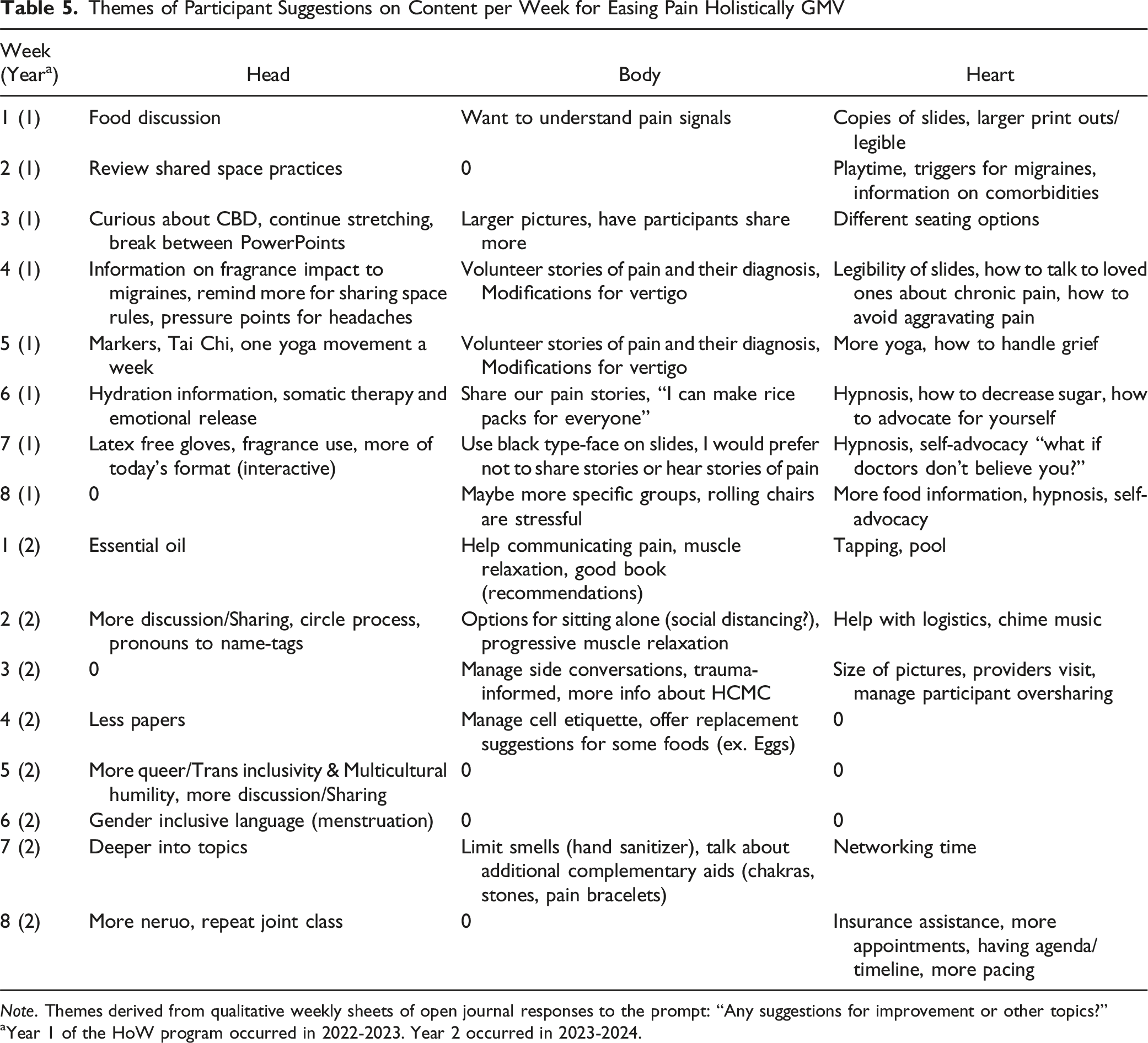
Note. Themes derived from qualitative weekly sheets of open journal responses to the prompt: “Any suggestions for improvement or other topics?”
aYear 1 of the HoW program occurred in 2022-2023. Year 2 occurred in 2023-2024.
Health equity was at the forefront of curriculum design, development, and implementation. This included addressing drivers of chronic pain (sedentary lifestyle, stress, inflammatory foods, isolation, sleep deprivation, etc.)27,28 through an emphasis on low to no-cost resources such as free meditation and sleep support apps, YouTube movement and relaxation videos, free farmers markets or food access resources, low-cost cooking approaches, etc. Many of the grant-funded gifts provided through the Integrative Pain Care kit (sleep masks, recipes, food/spices/teas, gift card for healthy food purchases, etc.) also provided resources and support to address these drivers.
Discussion
Heals on Wheels illustrates a collaborative multi-disciplinary program, addressing whole-person, integrative pain care education and practices for historically underserved participants within Hennepin County. The multi-disciplinary curriculum included various lifestyle, behavioral, complementary, and integrative health approaches to the complex and highly personal issue of chronic pain. Participants in the GMVs were primarily middle-aged women, with a high percentage of patients utilizing public insurance. This is in contrast to recent evidence showing that people with public insurance are less likely to access integrative, nonpharmacological pain care services, illustrating the health equity need behind our program. 29 The HoW program demonstrated high attendance and retention, demonstrating the feasibility of this innovative approach of community engagement workshops paired with an 8-week clinic-based GMV. Participant responses from the weekly qualitative clincal weekly sheets demonstrated appreciation and acceptability of the program, with particular emphasis on the importance of social support and group sharing. Suggestions for improvement were addressed through iterative changes to the curriculum and implementation of the GMV as well as through open discussions with the patients, gathering consensus on how to incorporate their suggestions. It is of note that the Heart series recruited the most patients, indicating an interest in exploring the emotional needs and stressors of people experiencing chronic pain. This program highlights the utility of IH approaches in service of health equity, bringing evidence-based integrative pain care to historically underserved communities.
In comparing our work with other studies, several innovative features of the Heals on Wheels program stand out. To our knowledge, no other health care system has implemented a combined GMV and community workshop program for Integrative Pain Care, with a health equity focus and outreach to historically underserved populations. Heals on Wheels Appetizer workshops stand out as a highly innovative and novel implementation strategy to expose more community members to evidence-based IH strategies for managing pain, recruiting new patients into the system, and building community trust. Patient mistrust in health care systems and providers has been identified as a barrier to optimal care and is associated with negative health behaviors and outcomes, specifically among racial/ethnic minority populations.30,31 By bringing non-pharmacological pain care directly to communities in the form of free interactive workshops, including the distribution of pain management self-care kits, we hoped to increase visibility and trust for the Heals on Wheels program. Building on the success of this model, with additional funding from foundations, we have implemented a “Light Lunch” 4-week community workshop series. This series has been hosted by community partner organizations that have hosted successful Appetizers. Light Lunch workshops utilize portions of the EPH curriculum but are accessible and offered at no cost to community members and take place in community spaces. Noting that 5 of the 149 Appetizer participants enrolled in the Full Meal GMV, the Light Lunch workshop series serves as an intermediary program to offer a more robust curriculum with the accessibility of community spaces. We are also exploring the possibility of billing for GMV’s hosted within community spaces.
The HoW program compares with several other early studies exploring GMVs for chronic pain in low-resourced communities. A prospective observational cohort study of 65 participants evaluating the feasibility and effectiveness of integrative GMVs for people with chronic pain and common comorbidities for primarily low-income and racially diverse populations found that integrative GMVs addressing chronic pain were feasible, with similar retention rates to EPH. 32 Our study showed similar gender/age breakdowns as this 1, but with fewer non-White participants. Their group intervention utilized similar mindfulness and evidence-based integrative medicine self-management techniques (such as acupuncture), healthy food activities, and topics (stress, sleep, mental health, activity, and nutrition) as our curriculum. Their groups were co-facilitated by a physician and an experienced co-facilitator with training in mindfulness and yoga, however, our GMVs additionally included an integrative Physical Therapist and psychologist co-facilitators with additional support from a team of other IH clinicians. Furthermore, our program uniquely separated the group into specific Body, Head, and Heart cohorts.
Another early study by Znidarsic et al evaluated GMV’s for chronic pain in a similar 8-week format across a large cohort (n = 178). 33 Their GMVs differed in that they were 3 hours in duration, whereas the HoW GMVs were 2 hours long. Their groups were co-facilitated by a physician and a holistic psychotherapist and did not include a physical therapist. Similar to our study, Znidarsic et al utilized both yoga and meditation as part of the weekly activities. Znidarsic et al utilized a similar spectrum of integrative and self-care therapies (eg, acupuncture, yoga, massage, chiropractic, art therapy, meditation) and topics (eg, nutrition, pain science) for patients with chronic pain. However, their curriculum included a session dedicated to goal setting which was not addressed in depth in our curriculum. Alternatively, our curriculum included sessions on topics such as sleep and stress management that were not directly addressed in Zindarsic et al’s curriculum. Zindarsic et al included a similar age/gender/race demographic to ours.
A more recent systematic review by Roth et al (2024) highlights the importance of referral networks for GMV recruitment within the clinical environment. 34 Furthermore, Roth et al. (2023) also state that poor referral networks and providers’ limited knowledge of integrative services serve as significant barriers to patients accessing integrative pain care. 35 Our HoW study outlines novel methods of recruitment through the use of Appetizer events out in the community in addition to clinical referral networks. These proposed methods serve the dual purpose of extending GMV recruitment capacity while simultaneously spreading real-time access to integrative care modalities and knowledge to community members. Roth et al (2024) also describe transportation as a significant barrier to accessing in-person groups. The current study aimed to address this barrier by implementing a system for offering and coordinating Lyft rides to and from GMVs for patients needing transportation. Roth et al (2023) conducted a similar study to ours, investigating the implementation of a virtual telehealth integrative GMV program with a curriculum developed to meet the needs of diverse patients with chronic pain. However, our program delivered 3 distinct pain-affinity variations of the EPH curriculums to further address specific origins of pain. 35 The conception of the three-cohort model for our GMV (Head, Heart, and Body) is a unique feature of our program. This process of creating a generalized and adaptable curriculum could serve as a model for other GMV programs beyond chronic pain populations. Roth et al. (2023) also noted that approximately 75% of patients in their study attended more than 2 out of 9 weekly integrative GMV sessions, while 83.3% (55/66) of patients participating in our GMV program attended more than 2 out of 8 GMV sessions. 35
The inclusion of qualitative measures of acceptability is also a unique feature of our study. In addition to supplying quantitative data, the self-assessment weekly progress sheets tool provided information to assist the lead physician in writing their notes in the patient’s medical record. In a standard 1:1 medical visit, the provider generally documents in the medical record during the visits. However, in a GMV, it is not feasible to document in multiple charts while also facilitating a group. Thus, the weekly progress sheets provided the necessary information on the patient’s pain levels, function, specific questions and concerns, and response to the curriculum in real-time, providing the essential elements of documentation for billing. Utilizing this information for documentation eases the burden on the provider to remember the individual details of participants’ needs and experiences. This improved ease of documentation and reduced electronic medical record strain on the physician which may improve provider wellbeing. 36 The weekly progress sheets also served as a contemplative prompt for the patients, allowing them to pause and consider what they found most meaningful from the visit. The utilization of the weekly progress sheets could be a useful tool for other GMVs beyond those serving people with chronic pain.
Unique aspects of the HoW program that emphasize health equity initiatives include the focus on geographic health disparities and communities experiencing disproportionate impact from the opioid crisis. The free transportation offered to participants addressed 1 domain of SDOH (ie, access). Other SDOH domains addressed with HoW were reductions in social isolation through GMV and Appetizer workshops and education empowerment through the HoW curriculum. Key barriers to evidence-based, nonpharmacological pain care identified by the AMA Pain Task Force (administrative and reimbursement, utilization of evidence, stigma, and physician workforce training) were uniquely addressed. 17 Administrative and reimbursement barriers were addressed through community appetizers being offered at no cost, in community spaces, and without any need to register in advance. The GMV was billed as a routine office visit (CPT Code 99213 or 99214) based on medical decision-making; no prior authorization was needed. The utilization of evidence-based nonpharmacological pain care strategies was built into the curriculum, with an integrated, multidisciplinary, and multimodal care model implemented through the diversity of curriculum development and facilitation team members. Concerns related to stigma were addressed by normalizing struggles with pain, stress, and medication use by encouraging group sharing during the GMV and workshop sessions. The HoW program addressed physician training and education by training 3 additional providers new to both the EPH curriculum and GMV care model during the second year of the program. Two of these providers have gone on to establish their own GMVs focused on healthy living strategies, illustrating the efficacy of incorporating provider mentorship into the program. Additional funding has been received to expand the HoW program’s reach through training other health systems and providers in the Heals on Wheels model statewide across Minnesota.
There are several limitations inherent within our methodology. All our subject population volunteered to attend the GMV and Appetizer workshops and thus a selection bias could influence outcomes. It is unknown why some individuals only attended 1 or 2 sessions as we did not systematically contact participants who declined to return to the GMV series. However, in 1 case a participant was not able to continue attending because she did not have familiarity with how to interact with the Lyft rideshare program and thus our transportation services did not create accessibility for her. Our GMV participant pool included a small number of people, mostly women, all English-language speaking, with limited racial representation, and thus our results may not be generalizable. With a smaller subject pool, unpredictable factors significantly impacted attendance results. For example, a severe winter storm affected attendance in our 2024 Heart cohort, and increased medical complexity, COVID-19 infections, and hospitalizations impacted attendance in the Body cohorts. Larger studies would likely minimize these unforeseen factors. We also did not collect a broad set of demographics for the GMV participants and thus details on income, marital status, education levels, Social Determinants of Health, etc. Are unknown. However, the high percentage of participants utilizing public insurance and requesting transportation support suggests that a high proportion of GMV participants experience low socioeconomic status. Attendance was the only outcome collected at the community Appetizer workshops and thus participant demographics and responses to the workshops are unknown. However, given the brief duration of the workshops, we did not deem it appropriate to collect extensive outcomes from the participants. This was in tune with our value of engaging in authentic and respectful community partnerships and keeping our ask of the participants in proportion to the service we were providing. In this way, we attempted to build community trust and honor health equity concerns of avoiding medical re-traumatization and harm for communities who might have previous medical trauma and/or distrust in our health care system. Community Appetizer workshops were offered at no cost to participants and patients with Medicare, Medicaid, and other public insurance were able to participate in HoW without any out-of-pocket costs. However, people with private insurance with high deductibles or out-of-network costs may have been excluded. The qualitative weekly progress sheets utilized for this study have not been independently validated, although our team piloted it successfully with previous GMVs. Future programs and research could use the HoW curriculum and model with a larger, more diverse and representative sample and with more rigorous methodology such as a cohort comparison or Randomized Control Trial design.
Conclusion
The Heals on Wheels program is an innovative, feasible, and acceptable model of how a community engagement and Integrative Pain Care Group Medical Visit program can reach historically underserved populations. The curriculum was based on lifestyle (nutrition, sleep, movement, stress management), social connection, pain science education, behavioral strategies, and Complementary and Integrative Health practices (mindfulness, mind/body skills, yoga, massage, and acupuncture). The curriculum for both Appetizers and GMVs represents a whole-person, pain care guideline-concordant approach to chronic pain care. Bringing this work to historically underserved populations has the potential to improve access to evidence-based nonpharmacological pain care and reduce harm from the opioid crisis.
Supplemental Material
Supplemental Material - Heals on Wheels: Development and Implementation of Community Outreach and Group Medical Visits for People Experiencing Chronic Pain
Supplemental Material for Heals on Wheels: Development and Implementation of Community Outreach and Group Medical Visits for People Experiencing Chronic Pain by Catherine Justice, Susan Haddow, Kate Shafto, Tegan Reeves, Jadyn E Knox, and Arti Prasad in Global Advances in Integrative Medicine and Health
Footnotes
Acknowledgements
We would like to thank Marchion Hinton, JoAnn Bell, Charlotte Alverez, Eiko Mizushima, Tracy Kapan, Cass McLaughlin, our community partner organizations, the Minnesota Department of Health and the Opioid Epidemic Response Advisory Council, and all of the participants and co-facilitators from the Heals on Wheels program.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Heals on Wheels project was funded from the Minnesota Department of Human Services through a recommendation by the Opioid Epidemic Response Advisory Council (OERAC). The views expressed in this publication do not necessarily reflect the official policies of the Minnesota Department of Human services; nor do the mention of trade names, commercial practices, or organizations imply endorsement by the state of Minnesota.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.