
Abstract
Background
Individuals with a uterus experience menopause, the cessation of menses, on average at age 51 years in the United States. While menopause is a natural occurrence for most, over 85% of women experience multiple interfering symptoms. Menopausal women face health disparities, including a lack of access to high-quality healthcare and greater disparities are experienced by women who are black, indigenous, and people of color. Some women are turning away from hormone therapy, and some seek integrative health interventions.
Objective
Some menopausal women who seek healthcare do not receive it as they lack access to medical and integrative healthcare providers. A potential solution to this problem is a medical group visit (MGV), during which a provider sees multiple patients at once. The aims of this study were to gather women’s opinions about the menopause, provider access, and conventional and integrative health interventions for later use to develop a menopause MGV.
Methods
We conducted a Community Engagement Session and a Return of Results (RoR) with midlife women to learn about their menopause experiences, barriers and facilitators to accessing health providers, and their interest in and suggestions for designing a future integrative MGV (IMGV). Thematic qualitative research methods were used to summarize session results.
Results
Nine women participated in the Session and six attended the RoR. Participants were well-educated and diverse in race and ethnicity. Themes included: an interest in this topic; unfamiliar medical terms; relevant social factors; desired whole person care; interest in integrative health; barriers and facilitators to accessing healthcare. The group expressed interest in ongoing participation in the future process of adapting an IMGV, naming it MENOGAP.
Conclusion
These findings highlight the importance of stakeholder engagement before designing and implementing MENOGAP and the great need among midlife women for education about the menopausal transition, integrative self-care, and healthcare.
Keywords
Background
All individuals with a uterus experience menopause, 1 the cessation of menses, which is a natural occurrence experienced during midlife. In the United States, the mean age of menopause is 51 years. 1 The menopausal transition leads up to menopause and may last a decade. Even though menopause is a natural occurrence for most, over 85% of midlife women experience multiple symptoms that interfere with their quality of life and daily activities. 2 Individuals may experience irregular periods, vaginal dryness, sleep problems, mood changes, weight gain and slowed metabolism, thinning hair, dry skin, vasomotor symptoms (VMS) including hot flashes, chills and night sweats, or loss of breast fullness.1,3
However, symptom experiences varies, and multiple studies report greater menopausal symptom severity and bothersomeness among black, indigenous, and other people of color (BIPOC) women.4,5 The Study of Women Across the Nation (SWAN) was launched to study physical, biological, and social changes experienced by African American, Hispanic, Chinese, Caucasian, and Japanese women. 6 The SWAN study is a multi-site, longitudinal, epidemiologic study designed to examine the health of diverse midlife women. 6 For example, this study informed us that African-American women are more likely to report heavy menstrual bleeding and to undergo hysterectomy and more severe VMS. 3 Notably, this study did not include American Indian/Alaska Native (AI/AN) women and very little is published about their menopause experiences. 7
A common treatment for women experiencing bothersome menopausal symptoms is Menopausal Hormone Therapy (MHT). The Women’s Health Initiative (WHI) conducted a study in 2002 about the safety of MHT and later conducted a risk/benefit analysis study of MHT in 2013, concluding that it is appropriate management for most women and contraindicated for women with estrogen-sensitive cancer or a history of coronary heart disease, blood clot, or stroke. 8 Data were re-examined in 2016, and MHT is listed as a first-line intervention to treat menopausal symptoms such as hot flashes, vaginal dryness, and mood changes. 1 Recent studies have indicated minimal to no contraindications to MHT being utilized by women younger than 60 without the contraindications mentioned above and during the 10 years after menopause. 9 MHT is a first-line treatment in The Menopause Society’s hormone therapy position statement, 10 and even though it is indicated for most women, there is a gap in care as not all women can access or choose to take MHT. For example, the State of Menopause Survey conducted in 2021 with 1039 women aged 40-65 across the United States found that more than 72% of surveyed women were familiar with MHT, but 65% said they would not consider using it unless their provider recommended it (32%) or a new clinical study emerged proving its safety (29%). 11 Further, a systematic review of nine surveys reported that 50.5% of women reported using non-pharmacologic interventions specifically for their menopause symptoms. 12 Thus, the present study was informed by these trends in the utilization of evidence-based integrative health and self-care information. The study team sought to gather midlife women’s feedback about the future process of designing an intervention that includes both medical and integrative healthcare interventions.
Women face many health disparities, high mortality rates, and healthcare access concerns. These problems can partially be attributed to the poor education of medical residents. 13 Only 6.8% of surveyed medical residents indicated that they felt adequately prepared to manage the care of women experiencing menopause. 13 Within the medical and nursing educational systems, there is a demand for better trainee education regarding care for women in the menopausal transition. 14 Insufficient training translates to poor care: one survey of midlife women reported that one-third of women said they felt their doctor isn’t comfortable talking about menopause, causing them to look elsewhere for support. 15 This could potentially be due to a lack of in-depth education of medical students. Approximately one-third of the surveyed residents opted not to offer MHT to a symptomatic, newly menopausal woman who did not have any contraindications to receiving MHT or to a prematurely menopausal woman until the natural age of menopause, despite the overwhelming evidence that MHT is efficacious and safe for these two categories of women. 16 As previously discussed, MHT does not come without side effects, nevertheless, some medical residents are not providing what is currently the first-line treatment for symptomatic menopausal women. Few publications highlight the attitudes of Nurse Practitioners (NPs) and other healthcare providers toward managing various symptoms and conditions during the menopausal transition. Still, literature does exist to educate NPs about the care of women during the menopausal transition.17,18
Another barrier midlife women face is the miscommunication of menopausal terms. Some cultures refer to the perimenopausal term as “the change” or “a transition” instead of using a medical term. In Europe, menopause is referred to as the “climacteric stage”. 19 In addition, high costs from the healthcare system, lack of insurance coverage, geographic location of residence, life priorities, and native languages are all barriers women may face to receiving adequate care.
There are numerous ways to decrease these health disparities. From a clinical standpoint, improving access to health care is a critical solution. Because of the potential negative consequences of MHT and health disparities, more women are turning away from MHT. Medical group visits (MGVs) are one efficient way to fill the gap in disparities in care so that whether a woman wants to take MHT or does not, she can receive medical care in a group setting.
MGVs, also known as shared medical visits, are medical appointments in which one to two providers deliver medical care for a group of patients with similar diagnoses or questions instead of a one-to-one medical appointment. MGVs are one potential solution to the shortage of providers because they allow for more individuals to be seen by a provider trained in concerns of the menopausal transition. MGVs allow individuals to be more easily seen by providers and create a community for the patients because they can meet others experiencing the same problems. 20 A qualitative study was performed on the delivery of MGVs, concluding that MGVs “successfully deliver on the promise of patient-centered care”. 21 MGVs have been designed for women receiving antenatal care, 22 for patients with diabetes mellitus, 23 and for psychiatric patients 24 – and participants in all 3 types of MGVs reported a preference for the group format over a return to individual medical visits.
There is minimal literature on MGVs for menopause. 25 Of the few studies of MGVs for the menopausal transition, one study included annual examinations, follow-up menopausal concerns, hormone therapy, bone densitometry results, and osteoporosis treatment follow-ups. The authors concluded that shared medical visits increased physicians’ productivity by 20% compared to individual appointments. The participants were surveyed afterward and responded, with the majority stating that they would prefer to go to another shared medical visit instead of the individual visit. 26
The aim of the present study is to ask a sample of midlife women about their experiences of the menopausal transition, what medical attention they sought out when they had bothersome symptoms, and whether they were interested in MGVs with integrative health components and if their communities might find a MGV of interest. The present study is the first step in a planned series of studies to adapt a MGV for peri- and post-menopause and test it for efficacy. If found efficacious, future studies of effectiveness and implementation in health systems will be conducted. The results from this first study will inform the future detailed development of an intervention to bridge the gap in knowledge about whether midlife women would prefer MGVs and components of evidenced-based integrative health and self-care information.
Methods
Ethics Statement
This study was approved by the University of Utah Institutional Review Board and each participant provided informed consent before the start of the session.
Community Engagement Sessions
We conducted two sessions with the same community members: (1) a Community Engagement Session (similar to a focus group) and (2) a Return of Results. The Engagement Session (“Session”) was designed to elicit community members’ opinions about the menopausal transition and access to medical care and non-pharmacological interventions such as acupuncture, acupressure, massage therapy, and chiropractic. We also asked about their preferred evidence-based, non-pharmacological components and delivery format. Community Engagement Sessions provide a format for researchers to consult with community experts – people with expertise about a particular topic from their lived experience. 27 The Meharry-Vanderbilt Community-Engaged Research Core 27 has identified best practices for enhancing community engagement in community consultations: early input, researcher coaching, researcher humility, balancing power, neutral facilitator, and preparation of community stakeholders. 28 These practices are also used to increase participant participation, to include various viewpoints, and avoid conflation or squelching of any idea or voice. We incorporated these best practices into the conduct of the Session, the results of which are presented here.
Our participants were recruited through referrals with The University of Utah’s Clinical and Translational Science Institute’s (CTSI) Community Collaboration and Engagement Team (CCET). This team is expert at conducting Sessions. Recruitment involved flyers, existing community partnerships, word of mouth, social media, and referrals from past participants. Screening of eligibility to participate was conducted by telephone and email. Potential participants were considered for inclusion if they were female, self-described, other, or prefer not to disclose sex/gender; had an intact uterus; within the ages 40-55; report poor menopause-related quality of life (≥3 on a 0-6 scale) and experiencing hot flashes (severity ≥3 on a 0-10 scale) lasting for 6 or more months; were willing to provide menstrual history which indicates either late transition (1+ missed periods in the last year) or early post-menopause stage (within 1 year of the final menstrual period); and were able to provide informed verbal consent.
The following questions were asked in the Session: 1. What interested you in this discussion? 2. Are the terms perimenopause, menopausal transition, and post-menopause familiar? 3. What is your experience with the menopausal transition? a. What age is relevant to this topic? b. What about social changes or social pressures? Are there any social aspects relevant to your experience of the menopausal transition? c. Are there any healthcare aspects to your experience of the menopausal transition? 4. What are the barriers to accessing healthcare providers (e.g., primary care providers, gynecologists, etc.)? What are the barriers to accessing integrative health providers (e.g., acupuncturists, massage therapists, chiropractors, etc.)? a. What helps you access healthcare providers? What helps you access integrative health providers? b. Where should resources for the group intervention be posted? 5. What are your feelings about the proposed group intervention?
These questions used lay language and were open-ended when possible. The questions were written to avoid negative or positive bias and allowed for any amount of detail and self-disclosure. Participants received a short verbal description of the Session and the proposed group medical intervention and were emailed the Session questions at least a week before the Session.
The Session was held on September 28, 2021, and was led by a CCET staff member experienced in facilitating this type of group and is independent of the research team. During the 2-hour Session, a facilitator led a discussion of the questions with the aim of eliciting responses from all Session participants; an experienced CCET scribe summarized the discussion on large paper as part of the facilitation. Several members of the research team observed the discussion. Session participants were provided with a $75 gift card to compensate them for their time.
Data Analysis
Conventional content analysis, an inductive method of qualitative research,29,30 was used to analyze the Community Engagement Session results. The Session was audio-recorded and transcribed. The de-identified transcription was read and re-read, after which coding was performed to identify themes and subsequent sub-themes by the first and second authors, with recoding until consensus was achieved. Participants’ comments are direct quotes, except that they were edited for brevity while maintaining the original meaning. Descriptive statistics, performed on de-identified data, were used to analyze the participant demographics using SPSS Version 27. 31
Return of Results
We conducted a Return of Results (RoR) to review the data tables with Session participants. This was an opportunity to obtain feedback from women about whether the identified themes were accurate and whether community members would suggest any additions, deletions, or changes to the data analysis.
Results
Demographics of Engagement Session Participants.

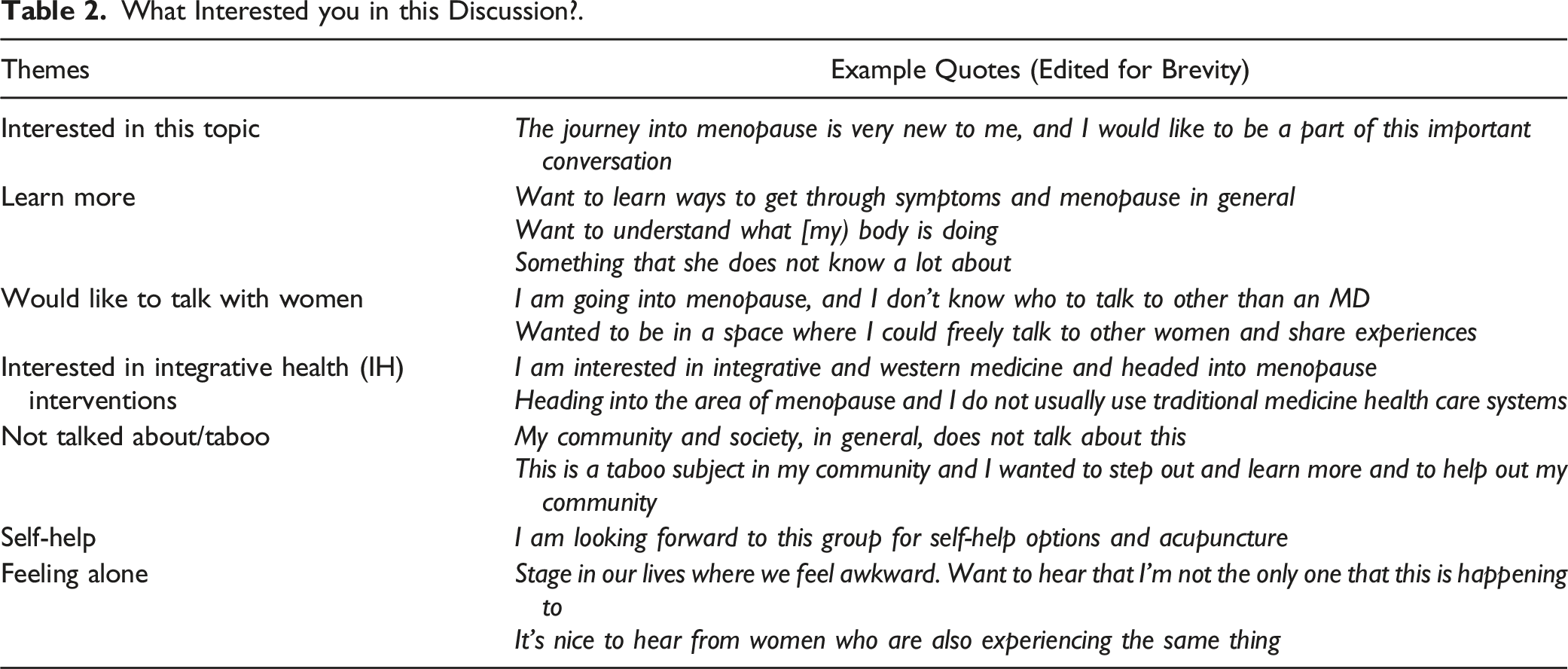
What Interested you in this Discussion?.
Are the Terms “Peri-Menopause” and “Post-Menopause” Familiar?.

What is Your Experience With the Menopausal Transition?.

Age Dimensions.

Social Dimensions.

Health Care Dimensions.

Barriers and Facilitators to Accessing Healthcare.

Perceptions of the Proposed IMGV Model.

Are the Terms Perimenopause, Menopausal Transition, and Post-menopause Familiar?
Several views were presented concerning terminologies such as perimenopause, menopausal transition, and post-menopause (see Table 3). Several women reported that they had not heard of various terms before attending this session. Women also noted that, for example in a Latino communities, the terminology is less important than having conversations on the topic while in a Polynesian communities, the change of life is a term that is used, but not really talked much about so it was difficult to know what age(s) were relevant. It was noted that in the Somali language that there was not a word for menopause. Women noted terms such as ‘change of life’ or ‘transition’ were helpful.
Tables 4–7 include the following four topics: 1) women’s experiences with the menopausal transition; 2) ages relevant to this topic; 3) social dimensions; and 4) healthcare dimensions.
What is Your Experience With the Menopausal Transition?
Concerning experiences, participants reported experiencing headaches, hot flashes, irregular menstrual periods, loss of memory, changes in mood, sleep disturbances, and vaginal dryness, as well as having no symptoms being experienced and being unsure about experiences. See Table 4, which also includes perceptions, or appraisals, about the various symptom experiences.
What Age is Relevant to This Topic?
Participants also mentioned age dimensions. Six of nine women commented about age as related to this topic. Some women reported that they had irregular periods in their late 30s and 40s and had problems with mood and sleep. Some women also reported that they did not have particular symptoms in their 40s and did not have the symptoms they thought they would in their 50s (see Table 5).
Are there Any Social Aspects to Your Experience of the Menopausal Transition?
Social dimensions reported by women (see Table 6) included being in the “sandwich generation,” trying to confide in friends but finding they were not also in the menopausal transition, basing anticipated menopausal experiences on their mother’s experiences, and that communication was needed about the transition.
Are there Any Healthcare Aspects to Your Experience of the Menopausal Transition?
Participants reported healthcare dimensions (see Table 7) such as unhelpful care from a provider, helpful care from a provider, the sex of the provider being relevant, and interest in whole person care vs pharmacologic treatments.
What are the Barriers to Accessing Healthcare Providers (e.g., Primary Care Providers, Gynecologists, etc.)? What are the Barriers To Accessing Integrative Health Providers (e.g., Acupuncturists, Massage Therapists, Chiropractors, etc.)? What Helps you Access Healthcare Providers? What Helps you Access Integrative Health Providers? Where Should Resources for the Group Intervention be Posted?
Participants provided detailed comments regarding barriers and facilitators to accessing health care – both conventional healthcare providers and integrative healthcare providers, such as acupuncturists, chiropractors, and massage therapists (see Table 8). Concerning accessing Integrative Health care providers, participants noted that location and availability were an issue and a lack of awareness about what acupuncture or massage could be used to treat. With respect to accessing conventional care, COVID-19-related concerns were noted, as well as issues with the location and availability of the provider, the need for childcare, lack of information about going in for preventive care, and finding that providers were reactive and not preventative. General limitations were noted, such as time and finding a provider they liked. A frequency count of barriers is included in Table 8, with the physical location being the most frequently mentioned barrier.
Facilitators to accessing healthcare providers (both conventional and integrative) included word of mouth, having insurance coverage, education about the insurance plan, doing their research, and having easily accessible public information (along with suggestions as to where we could post information about the proposed integrative medical group visit, IMGV).
What are Your Feelings About the Proposed Group Medical Visit Intervention?
Participants’ perceptions of the proposed IMGV are listed in Table 9. They indicated several positives about the proposed IMGV, such as a safe and designated time and place to talk about the menopausal transition, desire for a follow-up session, excitement about the IMGV, and that it is a whole person approach. Another expressed theme was that women feel unheard and unseen at this age and in this transition and that the IMGV would give acknowledgment to women. Several barriers were described, such as midlife women being very busy and lacking time to devote to a multi-session intervention, that childcare may be needed, and that perhaps the IMGV would need to be tailored for various cultures (and delivered in various languages), and that the IMGV might be overwhelming with many different components such as journaling and healthy eating. The name of MENOGAP was proposed and discussed, with the idea of the IMGV filling a GAP in MENOpausal women’s healthcare. Suggested formats included online, either synchronously or asynchronously, with a learning management system such as Canvas or via discussion boards.
Return of Results Session
We conducted a Return of Results Session on May 19, 2022, and 6 of 9 participants attended. The research team reviewed the data tables presented here with the midlife women. Participants provided input regarding clarifications and confirmed the identified themes in each of the tables. Feedback on Table 4 included that after the discussion in the fall, women’s thinking changed, and that hearing other women’s perspectives changed their own perspective. Several women mentioned that they had sought care from a healthcare provider; one participant found a menopause group on Facebook and found the discussion online helpful. Participants mentioned that having community and culturally specific tailoring to the IMGV would be appropriate and that the biggest identified need is education for midlife women about this topic because every woman will someday go through menopause.
Discussion
The Community Engagement Session with nine midlife women and Return of Results (RoR) session with six women yielded important information about their lived experiences during the menopausal transition and provided valuable advice about the future development of MENOGAP. Participants were diverse in terms of race/ethnicity and had various levels of post-secondary education. Fifty-five percent were black, indigenous, and people of color (BIPOC) compared to the state of Utah which is 23.3% BIPOC. 32 Themes included an interest in participating in this conversation; medical terms were unfamiliar and less important than having a conversation; this sample of midlife women experienced many symptoms; many social factors affected participants; receiving unhelpful and helpful healthcare; a desire for whole person care; a need for information about what conditions Integrative Health interventions can treat during menopause; and barriers to accessing both conventional and integrative care were identified. The group expressed great interest in the proposed IMGV model but expressed barriers such as a lack of time available and needing childcare. Women indicated that an online format may be helpful to overcome these barriers. Participants also indicated that cultural and linguistic adaptations of MENOGAP may be needed, so it could be culturally relevant for a specific community and offered in languages besides English. These findings highlight the importance of extensive engagement with potential stakeholders before the future design and implementation of MENOGAP. We plan to continue engagement with this group of community members, forming a Community Advisory Board (CAB), to collaboratively design an IMGV called MENOGAP.
Our findings are in alignment with existing literature – most of which is conducted with White women – on women’s experiences of the menopausal transition. Yet, our work is also aligned with studies focusing on a specific community. For example, a qualitative study asking Black women about their menopause and weight gain concerns reported that their sample was unprepared for changes experienced during menopause and were interested in receiving information about menopause. 37 Unfortunately, the same concerns expressed by a focus group conducted over a decade ago were echoed in the session we conducted: lack of support and confusion about symptoms attributable to the menopausal transition, as well as difficulties in obtaining helpful care from healthcare providers. 36 Midlife women want reliable information and opportunities to discuss the menopausal transition with (preferably female) health professionals is another theme from the present study that aligns with prior literature. 38
Although the Session provides important preliminary information about midlife women’s beliefs about perimenopause, the menopausal transition and post-menopause, symptoms experienced, and access and barriers to medical and integrative care, there are several limitations associated with our study. We had a slightly younger sample that was highly educated (compared to general US and Utah rates), and we did not have any participants who were post-menopausal. We also had a relatively educated sample living in urban and suburban areas. Thus, results may not be representative of women living in rural or frontier areas, as well as those with less education. Further, we did not ask about menopausal hormone therapy (MHT) directly, which negated our ability to discern interest in MHT as well as integrative health, or separately. Perhaps most importantly, we conducted the study with a small group of women, thus results of the study must be taken with caution as they may not be reflective of women’s experiences in other regions of the country and may lack external validity. While a conversation was had among women of varying races and ethnicities, this study did not take a “deep dive” into any one community’s experiences of menopause. There is a risk of potential bias of minimizing experiences due to a lack of information. However, only so much depth may be obtained during a 2-hour focus group, and that is indeed a limitation of the present study. One step we did take to increase rigor was to conduct a follow up session, a RoR, in which results were presented back to participants for clarification, change or improvement.
Our study suggests the great need for education about the menopausal transition for midlife women. A novel finding is that a whole person health perspective to managing menopausal transition and post-menopausal symptoms is of great interest to midlife women who participated in the study. Future research can be informed by one finding from our study, to develop interventions in different languages and reach out to different cultures: we recommend that future interventions be developed with appropriate cultural and linguistic adaptations to be relevant to various cultures. For example, some communities have long-standing traditions of herbal or tea consumption and massage. We recommend that providers discuss natural folk remedies that are culturally relevant but also have safety data, and ideally, efficacy data. For example, Black Cohosh has been used by American Indian/Alaska Native women for centuries 39 and is likewise evidence-based. 40 Further, information provided in interventions should include symptoms commonly experienced, the timing of symptoms during the stages of the transition (late reproductive, early and late transition, early and late post-menopause), and variability in symptom experience (symptoms may last for years for some women while others are asymptomatic or experience minimally bothersome symptoms). Education could include self-care symptom management tips, pharmacological and non-pharmacological care, and information that is culturally relevant and tailored. Our participants repeatedly stressed that the social nature of the session was helpful and that women felt reassured they “weren’t going crazy” because other women in the group expressed having similar experiences. This points out the need for information and support for midlife women in the menopausal transition. The social support, education, and self-care included in an IMGV may provide much-needed care during this natural, but sometimes problematic, life transition experienced by everyone with a uterus.
The information gained from this qualitative data contributed to plans to engage in the future adaptation of an IMGV called MENOGAP, designed to fill these gaps in menopausal women’s care. Session participants expressed interest in joining a Community Advisory Board (CAB) to provide ongoing collaborative design of the MENOGAP intervention. Mixed-methods and application of the Meharry-Vanderbilt Community Engaged Research best practices 28 will be used to assess participant feedback in an iterative fashion to adapt MENOGAP to suit midlife women’s preferences for health education about menopause (“menopause 101”), pharmacological and non-pharmacological treatment options, and evidence-based self-care for behavioral change and improving patient activation and self-efficacy. Just as MGVs are preferred over individual visits by patients with diabetes, psychiatric disease, and women receiving antenatal care, we anticipate that MENOGAP may be acceptable, and perhaps even preferred to one-on-one visits, by some midlife women as social support has been identified as being beneficial to midlife women, 41 women report high levels of satisfaction 42 and appreciating the group medical visit format. 43
Summary Sentences
This study engaged midlife women before the design and implementation of MENOGAP, a proposed multi-component intervention with group medical visits and evidence-based integrative healthcare information. Participants reiterated the great interest in a whole-person health intervention and the need among midlife women for education about the menopausal transition, self-care, and healthcare.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by funding from the Undergraduate Research Opportunities Program at the University of Utah, which was awarded to KS.