
Abstract
Although there is a strong consensus that music listening is a common and effective means to induce states of relaxation, little attention has been given to the physical effects of such states and the potential health-related applications. In this article, we investigated whether music listening could induce affective states of relaxation and accelerate the recovery of fatigued muscles, through the analysis of quality of movement. Twenty healthy participants were asked to perform a fatigue induction protocol of the non-dominant arm followed by a resting period and the execution of a drinking task. During recovery periods, all participants were exposed to three experimental conditions: listening to relaxing music; arousing music; and no music. 3D motion capture and surface electromyography were used to record upper limb movements and muscle activity when performing the drinking task before and after the recovery periods. Movement quality was assessed by means of movement smoothness (jerk index) and muscle recovery (motor unit recruitment). Results showed that recovery of movement smoothness in the relaxing music condition was significantly greater (-35%) than in the relaxing music condition (compared to arousing music, -25%, and silence, -16%) which demonstrates that listening to relaxing music speeds up the recovery process of (fatigued) muscles. We discuss our findings in the context of potential applications of music listening for reducing muscle tension in people suffering from hypertonia.
Introduction
Hypertonia is a condition characterized by an excessive level of muscle tone (i.e., the amount of tension in a muscle at rest) caused by damage to brain regions that regulate muscle activity and/or to the spinal cord (which affects the transmission of those signals to the body) (Sanger et al., 2003). Such damage can occur for a variety of reasons including traumatic head injuries, strokes, brain tumours, neurodegenerative diseases (e.g., multiple sclerosis or Parkinson’s disease) or neurodevelopmental disorders (e.g., cerebral palsy). The effects of hypertonia are muscle stiffness and difficulties in moving the joints, which have an impact upon people’s ability to maintain postures, execute movements (including ambulation), and function normally in a variety of everyday life contexts and situations (Gracies, 2005; Singer et al., 2010).
Hypertonia management typically involves various types of muscle relaxant medications, physical and occupational therapy, which are usually used in combination rather than isolation in clinical practice and depend on the underlying cause of the condition (Chang et al., 2013; Nair & Marsden, 2014). Medications can be orally administered (the three most common are Baclofen, Diazepam, and Dantrolene), transdermally, intramuscularly, or intrathecally (i.e., injections into the spinal canal). However, high doses of medication can lead to an unwanted number of side effects due to its systematic effect, procedural errors, and possible transmission to other areas of the body (Chang et al., 2013). Beside these side effects, medication use hinders easy access to care as it requires experienced providers, is not well tolerated by patients (especially children), and is expensive (Chartered Society of Physiotherapy, 2012). Although physiotherapy has been proposed to treat hypertonia, evidence that supports its effectiveness is lacking (Khan et al., 2017; Nair & Marsden, 2014). Together with issues related to limited provision (e.g., resource limitations, lack of therapists (Physiotherapy, 2012)) and poor therapy adherence (e.g., due to several physical, psychological, socio-demographic, and clinical barriers (Jack et al., 2010)), new treatment strategies should be explored to avoid a negative impact on patient outcome and activities of daily living (ADL). Therefore, finding new, complementary, easily accessible interventions for hypertonia that promote therapy compliance could bring many benefits to a large number of people.
Music Listening and Muscle Relaxation
Music listening is a common and effective means used by people in everyday life to induce states of relaxation in a variety of ways. Indeed, listening to music can allow people to avoid unwanted environmental stimuli via masking, as a means for distraction from stressful stimuli (e.g., psychological distress, physical pain) and, most importantly, eliciting central and peripheral physiological responses that facilitate relaxation responses (Krout, 2007). One such type of responses can be elicited through entrainment via the autonomic nervous system (ANS), which results from the human natural predisposition to respond to and synchronize with internal and external stimuli (including sound and rhythm) (Clayton et al., 2004). Via entrainment processes it is possible for auditory information to facilitate relaxation by positively affecting heart rate, respiration, oxygen consumption, and blood pressure (Collinge, 1998; Crowe, 2004), in part via the activation of the parasympathetic nervous system (Schneck et al., 2006). There are various demonstrations of this phenomenon for stress reduction (Bernardi et al., 2006; Chafin et al., 2004; Kemper & Danhauer, 2005; see also Pelletier, 2004 for a meta-analysis), but also for the induction of a variety of emotional states. In fact, entrainment is a core mechanism of emotion induction through music (Scherer & Coutinho, 2013).
One of the components of music-induced physiological reactions that is especially relevant for hypertonia is music’s capacity to affect muscle tension. Indeed, as already noted by Sears (1958), muscular tension is “a direct reflection of the emotional state” and so “the study of the effects of any stimuli such as music on the muscular system should reflect the total response of the whole organism” (Sears, 1958). This is even more evident due to the fact that music revolves around tension-resolution patterns (Koelsch, 2014), which is expected to induce a corresponding physical or muscular tension in the listener (Dainow, 1977). Perhaps surprisingly, very little attention has been devoted to this topic, partially because direct measurement of muscular tension was commercially unavailable until the 1950s (before then, indirect methods were applied by researchers to investigate the relationship between musical and muscular tension; see Dainow, 1977 for an overview). The first studies that used surface electromyography (EMG) as a means of measuring muscle tension were conducted in the 1950s and 1960s by Sears, who found that tension could be manipulated by music in predictable ways (Sears, 1958, 1960). Since then, only a few studies have investigated whether listening to music changes muscle tension and evidence is scarce, but findings tend to support the notion that it does, and particularly that “relaxing” (or sedative) music is linked to decreased muscle tension (amongst other physiological markers of relaxation; see Hodges, 2010 for a review).
Music-induced Relaxation and Hypertonia
In recent work (Van Criekinge et al., 2019), a systematic literature review of randomized control trials (RCTs) was conducted to evaluate the effectiveness of music listening on muscle activity and relaxation on patients suffering from neurological disorders and hypertonia (e.g., stroke, cerebral palsy, Parkinson’s disease, spinal cord injury, multiple sclerosis, etc.). Six studies met the eligibility criteria, which comprised a total of 171 patients with a variety of neurological conditions. The analysis showed a large treatment effect of music listening on muscle performance (SMD 0.96, 95% CI 0.29 to 1.63, I2 = 10%, Z = 2.82, p = 0.005), which suggests that music listening interventions (MLI) can induce muscle relaxation in neurologically impaired patients. It was also found that MLI can be used during rehabilitation tasks (e.g., physiotherapy) or during rest, and that musical preferences seem to play a major role in the observed treatment effect. Nonetheless, Van Criekinge et al. (2019) also found several gaps in the literature that warrant further research. The most important gap was that assessment tools varied greatly from study to study and only a limited amount of research was performed with adequately quantifiable measures, such as EMG.
Research Questions and Hypotheses
Despite the existence of some evidence that sedative music can reduce muscle tension and that MLI can induce muscle relaxation in neurologically impaired patients, no studies have investigated whether music-induced muscle relaxation has an impact on movement quality. The latter is a crucial outcome for demonstrating the potential benefits of music listening for people living with hypertonia, since it would show whether or not this type of intervention would have tangible effects on functional ability (Kwakkel et al., 2019). In our research, we intend to address this gap and test the effectiveness of music listening to induce muscle relaxation and facilitate the performance of physical exercises.
Given the exploratory nature of our work, we will focus on a healthy population (rather than a population of people suffering from hypertonia) and simulate hypertonia by inducing muscle fatigue in our participants (Gates & Dingwell, 2010; Vafadar et al., 2012). Our broad aim is to determine whether listening to sedative music can accelerate the recovery of fatigued muscles by improving the quality of movement whilst executing a daily task (drinking from a cup). Our objectives are twofold. First, we want to investigate if our protocol is effective in generating upper limb fatigue by comparing movement smoothness and motor unit recruitment to the non-fatigued state. Second, we want to determine if different types of music varying in their level of arousal (i.e., the energy level associated with the music affective experience) can speed up the natural recovery process of a fatigued muscle when compared to a silent condition.
We hypothesize that (1) our protocol for inducing upper limb muscle fatigue will result in decreased movement quality as a result of fatigue exercises which will lead to decreased smoothness of movement, increased motor unit recruitment but less activation of high-force motor units (and therefore decrease of firing frequency) when participants perform a drinking task; (2) sedative music will result in faster recovery rates in movement smoothness and motor unit recruitment when compared to arousing music or no music (silence). Overall, we aim to explore if music listening can have a positive effect on the recovery of movement quality, and therefore be a potential type of intervention for patient populations suffering from hypertonia to facilitate rehabilitation and ADL through improving movement quality and control.
Methodology
This study was conducted according to the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) statement and received ethical clearance from the University of Liverpool’s Ethics Committee (project reference number: 4605).
Participants
We recruited 20 adult participants (age 18 or over) with no orthopaedic or neurologic conditions that could influence motor function of the upper limb. Informed consent was obtained from all subjects prior to participation.
Muscle Fatigue Induction Protocol
Participants fatigued the non-dominant arm by executing push-pull exercises performed via the Humac Norm isokinetic ergometer (Computer Sports Medicine Inc., Stoughton, MA, USA). The elbow-shoulder adapter of the Humac Norm was used, and angular velocity was set a 60°/s (see Figure 1). Data reports were collected to determine whether participants reached adequate levels of muscle fatigue, and exercises were terminated after completing the entire set of 5 series of 25 repetitions or sooner when performed power was reduced by 50%.

Fatigue inducing upper limb push and pull exercise using the Humac Norm.
Movement Measurements
An instrumented movement analysis was performed during drinking tasks of the non-dominant arm. The laboratory where the study took place is equipped with an automatic three-dimensional Qualisys motion capture system (Qualisys AB, Göteborg, Sweden) with 12 Mocap cameras (Qualisys OQUS-7 series, 12 Megapixel resolution, 200 frames per seconds). Twenty-nine reflective markers were attached to anatomical landmarks of the non-dominant arm: tip of second finger and thumb, (proximal) interphalangeal joint of the second finger and thumb, metacarpophalangeal joint of the second finger and thumb, styloid process of ulna and radius (wrist), lateral and medial epicondyle of elbow, left and right acromion (shoulders), jugular notch of sternum (thorax), C7, four on the head, upper and lower arm, and three on the object.

Overview of the drinking task.
Reflective markers were tracked and labeled using the Qualisys Track Manager, marker trajectories were filtered (low pass zero phase shift fourth order Butterworth filter, cut off frequency 6 Hz). Trials were further processed with the .c3d files obtained in Qualisys Track Manager and were exported to a custom-made MATLAB® (R2015a for Windows, ©The MathWorks, Inc., Natick, USA) file to calculate the variables of interest.
Movement quality is a hypothetical concept which can be related to a variation of kinematic parameters such as motion fluency, spatiotemporal variability, movement accuracy, smoothness of movement, joint range of motion, etc. To assess these parameters, jerk measures are traditionally used, which correspond well to the reaching movements of healthy subjects (Balasubramanian et al., 2015). Therefore, the primary outcome measure is this study is the smoothness of the trajectory path, calculated by the jerk index. Normalized jerk (NJ) is the time (third) derivative of position (dimensionless) (Alt Murphy et al., 2011); normalization with movement length and durations is necessary to calculate a dimensionless jerk-based measure (Hogan & Sternad, 2009). The mean value of the normalized jerk during the drinking task was calculated using the formula

where jerkhand(t) third derivative of hand displacement, tstart hand marker exceeding 5% of the peak velocity in the reaching task, tend hand marker was less than 5% of the peak velocity of the returning phase, MD movement duration, and Lhand movement length.
Muscle Activity Measurements
Movements are generated and controlled by muscle activations, and insufficient coordination between these muscles can generate irregular movement trajectories. To examine the effect of music listening on the recovery of the quality of movement, a thorough analysis of muscle activity is necessary. Muscle recovery can easily be assessed by motor unit recruitment; a motor unit is a group of muscle fibres innervated by a single motor neuron. The size principle of motor unit recruitment states that slow motor units are activated during low-force contractions and can sustain prolonged contractions, compared to fast motor units which are activated during high-force contractions for only a limited amount of time (Wakeling et al., 2002). Therefore, fatigued muscles after high-force contractions show less activation of these high motor units as they fatigue more rapidly (Wan et al., 2017), which enables investigation of muscle recovery based on motor unit firing. In order to measure muscle activity, we used an integrated, wireless surface electromyography (sEMG) system (Trigno, Delsys Inc., Natick, MA, USA) and followed Surface ElectroMyoGraphy for the Non-Invasive Assessment of Muscles (SENIAM) recommendations for sensor placement, sEMG sensor type, and sensor location on individual muscles (Hermens et al., 1999). Measurements were obtained for the following muscles: M. Deltoideus (lateralis), M. Pectoralis Major, M. Biceps Brachii, M. Triceps Brachii, M. Brachioradialis, and M. Extensor digitorum longus. Given that high and low frequency bands of the sEMG signal can distinguish between fast and slow motor unit recruitment (Wakeling, 2004; Wakeling et al., 2002), we computed the frequency bands of the myoelectric signals using wavelet analysis (Raez et al., 2006) implemented in Matlab. The centre frequency calculated during wavelet analysis was used to investigate motor unit recruitment. The cwt function of the Wavelet Toolbox in Matlab was used with three parameters set at 3 and 100 for time x bandwidth, yielding good resolution in the frequency domain.
Experimental Conditions
Our study included three experimental conditions during the recovery periods: listening to relaxing music (C1), listening to arousing music (C2), and no music/silence (C3). The music pieces for conditions C1 and C2 were selected a priori by a group of six people (including the investigators). Both pieces were instrumental jazz pieces conveying only positive emotions (to avoid negatively affecting participants’ moods and adding confounding variables to the study) but contrasting in terms of affective arousal. The piece selected for C1—“Whistle Songs” 1 by Relaxing Jazz Instrumental (Album: Jazz Relaxing Cafe)—intended to elicit a positive mood with low arousal (i.e., feelings of relaxation) and the piece selected for C2—“Sing, sing, sing” 2 by Benny Goodman (Album: Bugle Call Rag—Live)—intended to induce a positive mood with high arousal (i.e., joy). Moods related to the music were assessed by means of the GEMIAC questionnaire (Coutinho & Scherer, 2017).
Procedure
The core task consisted of participants reaching towards a clinically relevant target: a cup filled with water placed at the patient’s maximum reach distance from the body midline (van Kordelaar et al., 2012). The location was marked on the table, so participants were able to place the cup at the exact location. The water level of the cup was predetermined and standardized in every participant and trial. The drinking task (DT) involved reaching, grasping, and lifting the cup, bringing it towards the mouth, and placing it back at the initial position (see Figure 2). During each measurement moment, the drinking task was performed a minimum of three consecutive times to ensure the recording of multiple qualitative trials.
At the start of the study, participants performed a baseline DT to measure their normal movement pattern and muscle activity. Then, they performed a set of fatigue induction exercises. Immediately after, participants performed another drinking task (post-fatigue measurement) followed by a rest period of 3min 18s. During the rest period, participants wore over-ear headphones and were exposed to one of the experiment conditions (C1, C2 or C3). At the start of the rest period, participants heard an audio message via headphones explaining whether they would listen to a music track or not (to avoid startling participants if a song would be played). After 30s of silence, one of the music tracks would start or the silence would continue for 2min 48s (the length of both tracks). The recovery time was normalized for all conditions, that is, an equal amount of time elapsed between the fatiguing exercise and the end of the rest period (with or without music). At the end of this period, participants performed another DT (post-recovery measurement). This sequence was repeated three times in such a way that every participating was exposed to all three conditions during the study. The order in which participants were exposed to each condition was randomized across participants to avoid serial effects, and the randomization process assured that each condition appeared (approximately) the same number of times in experimental sequence. Musical pieces were also equally distributed between conditions. Figure 3 depicts the study protocol.

Overview of the study protocol. DT: Drinking task. RP: Recovery period with either sedative music (C1), arousing music (C2) or silence (C3). MF: Muscle fatigue exercises. EMG and movement measurements were collected continuously throughout the session.
Statistical Analysis
Statistical analysis was performed using SPSS version 24 for Windows (IBM Corporations, New York, USA). Chi-squared tests were performed to compare the emotional responses elicited by the music in C1 and C2. In order to determine if the upper limb was sufficiently fatigued, we used a repeated measures generalized linear model (GLM RM) to detect differences between pre- and post-induced muscle fatigue. Specifically, a two-way 3 x 2 repeated measures Analysis of Variance (ANOVA) with condition (C1, C2, C3) and time (pre and post) as factors and mean wavelet centre frequency and jerk index as outcome measures. Mauchly’s test of sphericity was performed to assess the likelihood of Type I errors. When sphericity was violated, the Greenhouse-Geisser method was performed to correctly report the degrees of freedom and p-value. In addition, differences between experimental conditions (C1, C2, C3) were analysed with a one-way repeated measured ANOVA with only a condition factor. Bonferroni corrected post hoc tests were performed to determine significant differences between conditions.
Results
Patient Characteristics
All participants were included in the final analysis. The sample characteristics are shown in Table 1.
Participant characteristics.

Y: years, kg: kilograms, cm: centimetres, SD: standard deviation
Emotional Experience
The average intensity with which participants experienced each of the GEMIAC feeling classes is depicted in Figure 4.

Ratings of intensity of experienced feelings while listening to the sedative (C1) and the arousing (C2) music pieces. Ratings range from 1 (not intense at all) to 5 (very intense) and were averaged across all participants.
In relation to the sedative music piece (C1), results show that the strongest feelings (those with ratings over 3, i.e., at least moderately intense) experienced by participants were relaxed/peaceful (M = 4.3, SD = 0.8) and full of tenderness/warmhearted (M = 3.6, SD = 1.2). Furthermore, Chi-square tests revealed that these both classes of feelings were significantly higher in C1 compared to C2 (relaxed/peaceful: χ2 (4, N = 104) = 33.2, p < .001; tenderness/warmhearted: χ2 (4, N = 40) = 14.2, p = .007). In relation to the arousing music piece (C2), the strongest feelings elicited were energetic/lively (M = 4.0, SD = 1.1), joyful/wanting to dance (M = 3.8, SD = 1.3), and inspired/enthusiastic (M = 3.4, SD = 1.2). Chi-square tests confirmed that these classes of feelings were significantly higher in C2 compared to C1 (energetic/lively: χ2 (4, N = 104) = 27.1, p < .001; joyful/wanting to dance: χ2 (4, N = 40) = 23.2, p < .001; inspired/enthusiastic: χ2 (4, N = 40) = 14.9, p = .005). Overall, these results confirm our expectations regarding the emotional experiences elicited by the two pieces: both pieces elicited positive emotional experiences, the sedative piece elicited feelings of relaxation/peacefulness, and the arousing piece elicited feelings of energy/liveliness and joy.
Movement Quality
Mean Normalized Jerk Index (MNJI)
The MNJI during the different conditions is shown in Table 2. The GLM RM showed that there were statistically significantly differences between conditions (p < .001). Post hoc analysis revealed that the MNJI at baseline was significantly lower compared to all the fatigued conditions (before sedative music: p = .001; before arousing music: p = .011; before silence: p = .001; see supplemental Figure 1). An increase in MNJI of 55%, 51%, and 59%, respectively, demonstrates that the muscle fatigue induction protocol was effective in producing a less smooth movement pattern during the drinking task. In addition, the Bonferroni corrected post hoc tests showed that recovery occurred during all conditions as significant differences were observed between the fatigued and recovered phases (p < .0001). Finally, listening to sedative music was the only condition that allowed for the MNJI to fully return to its baseline value in the period of time considered.
To compare the effect of the three experimental conditions on the recovery process, we computed the difference between MNJI before and after the recovery period for each condition. A one-way ANOVA revealed statistically significant differences between the three conditions (p = 0.002; see also Table 2 and supplemental Figure 2). Bonferroni corrected post hoc test showed that the only significant difference (p = 0.002) was between C1 (sedative music) and C3 (silence), which represented a decrease of 35% in MNJI after listening to relaxing music. No significant differences were found in any other comparisons, that is, C2 (arousing music) did not differ from C1 (sedative music) or C3 (silence).
Comparison of raw data and mean changes of the mean normalized jerk index during the different music conditions. BL: baseline; C1: sedative; C2: arousing; C3: silence, pre: fatigued; post: recovered; SD: standard deviation; SE: standard error; CI: confidence interval. Post hoc analysis was Bonferroni corrected.

Centre Wavelet Frequency
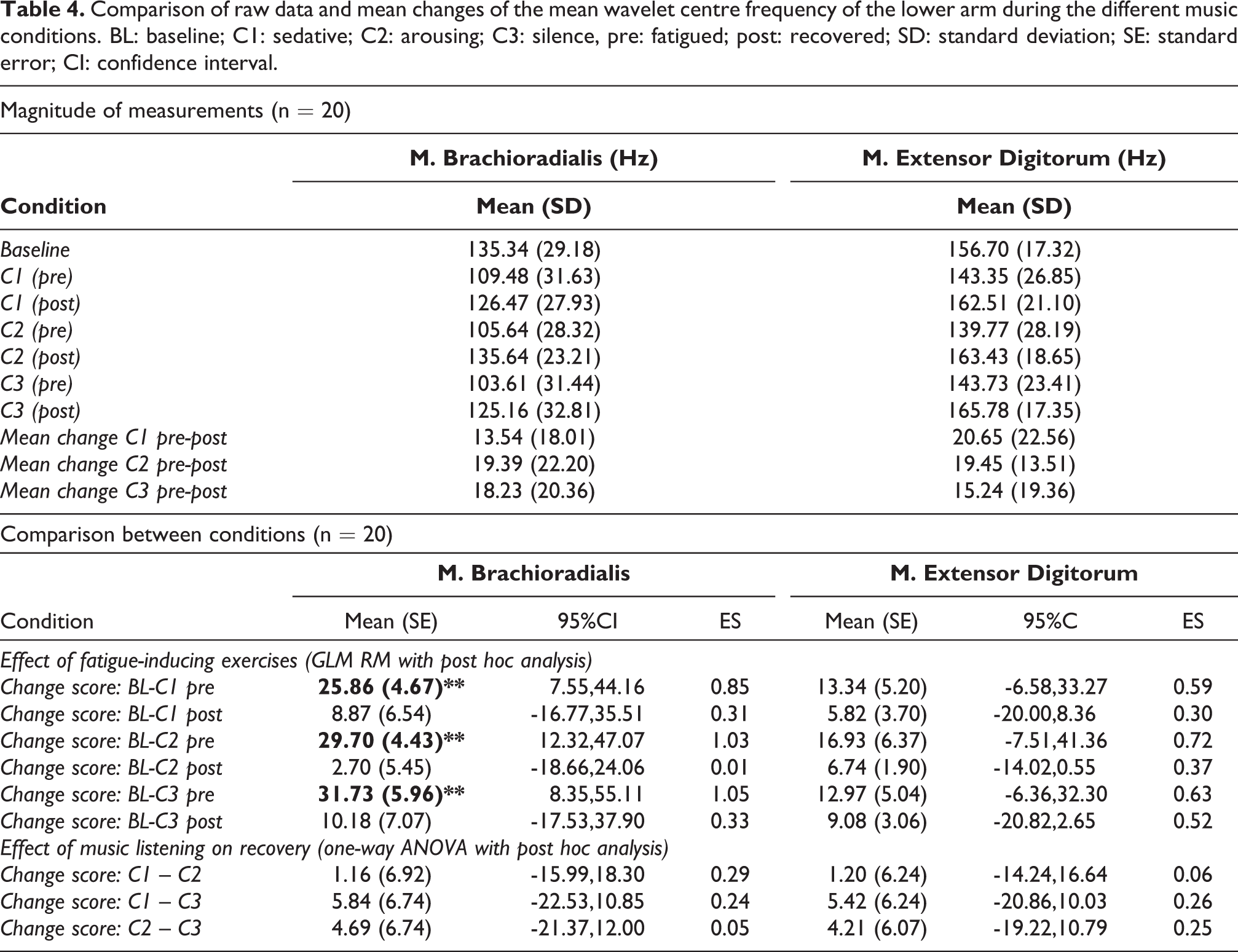
The mean wavelet centre frequency (MWF) during the different conditions was significantly different for M. Deltoideus, M. Triceps, M. Biceps, M. Brachioradialis, and M. Extensor Digitorum (p < .001) as depicted in Table 3 and Table 4 (see also supplemental Figure 1). Post hoc analysis showed that the drinking task at baseline was significantly different from the all the fatigued conditions for the M. Deltoideus, M. Triceps, M. Biceps, and M. Brachioradialis (see also supplemental Figure 2). Moreover, the least amount of recovery was found in the M. Triceps as significant differences between baseline and the recovered condition were still present in C2 (arousing p = 0.036) and C3 (silent p = 0.035) conditions. On the other hand, the fatiguing protocol did not seem to alter the MWF of the M. Extensor Digitorum. In addition, recovery occurred in all muscles during all experimental conditions when comparing the fatigues with the recovered conditions, except for the M. Brachioradialis after C1 (sedative music). No significant effects of musical conditions on MWF were found for all muscles (see Tables 3 and 4).
Comparison of raw data and mean changes of the mean wavelet centre frequency (Hz) of the upper arm during the different music conditions. BL: baseline; C1: sedative; C2: arousing; C3: silence, pre: fatigued; post: recovered; SD: standard deviation; SE: standard error; CI: confidence interval; *p < 0.05, **p < 0.01, ***p < 0.001. Post hoc analysis was Bonferroni corrected.

Comparison of raw data and mean changes of the mean wavelet centre frequency of the lower arm during the different music conditions. BL: baseline; C1: sedative; C2: arousing; C3: silence, pre: fatigued; post: recovered; SD: standard deviation; SE: standard error; CI: confidence interval.
Discussion and Conclusions
Music listening is a common and effective means used by people in everyday life to induce states of relaxation in a variety of ways. However, very little attention has been given to the effect of music listening on muscle relaxation and its ability to manage hypertonia and improve movement quality during ADL. In the research presented in this article, we addressed this gap and investigated whether music listening could aid in the recovery of fatigued muscles (an experimental proxy for muscle tension). To that end, we designed a protocol for inducing upper limb fatigue by analysing movement smoothness and motor unit recruitment during a drinking task and investigated whether listening to sedative or arousing music (compared to silence) could accelerate the muscle recovery process and the quality of movement when performing the same task.
Results show that the proposed muscle fatiguing protocol reduces the movement quality of the drinking task. Indeed, decreased movement smoothness was found during all fatigued conditions as compared to baseline. This suggests that the protocol was able to induce a less coordinated movement pattern (van Kordelaar et al., 2014). In addition, a reduction of high-force motor unit activation was seen when participants performed the drinking task in the fatigued conditions. Similar motor unit changes in fatigued muscle have been reported (Wan et al., 2017). Decreased activation of fast, high-force motor units was present for shoulder, upper and lower arm muscles. Thus, we can conclude that the push-pull protocol is effective in fatiguing the upper limb musculature, decreases movement quality during a drinking task, and can be used as a proxy for simulating movement difficulties associated with muscle tension. This validation will enable researchers to easily adopt this protocol in future works to selectively fatigue the following muscles: M. Deltoideus, M. Triceps, M. Biceps, and M. Brachioradialis.
Our central goal was to determine whether listening to relaxing (sedative) music over a period of time resulted in faster recovery rates when compared to arousing music or silence. In accordance with our hypothesis, we found that listening to sedative music (compared to silence) significantly accelerated the recovery process and improved the quality of movement when performing a drinking task, whereas listening to arousing music did not. Nonetheless, we did not find the expected differences in motor unit recruitment. In sum, although movement smoothness increased, the underlying mechanism of this improvement is unclear.
A reason for this discrepancy might be the difference between neural and muscular control of fatigue. Jerk was experimentally induced in our study by fatiguing the muscles on peripheral level and our EMG measurements also focused on peripheral fatigue. Nonetheless, recovery of fatigue cannot be explained by peripheral factors alone; the central nervous system is also involved in this process (Carroll et al., 2017). In fact, the central nervous system is highly important in the recovery process and research suggests that interventions aiming at improving central nervous system function might be even more effective in the recovery of fatigue (Minett & Duffield, 2014). Therefore, the lack of peripheral muscle improvements suggests that the fatigue reduction induced by music was due to neural regulation processes rather than muscular, and that the faster recovery of movement smoothness in the sedative musical condition found in our study may have been driven by central recovery instead of peripheral recovery (motor unit recruitment). This can explain why we found improved movement quality without muscular changes, in line with previous research showing that music listening can positively affect neural activity (Boso et al., 2006). Further work is necessary to validate this hypothesis.
Our findings have implications for people suffering with hypertonia, and particularly to those with disorders of the central nervous system, such as stroke survivors. After a stroke, patients are at great risk to develop upper limb spasticity which impairs their ADL and could eventually lead to increased levels of pain and contractures. Spasticity is a consequence of upper motor neuron lesions disturbing the balance between supraspinal inhibitory and excitatory signals (Trompetto et al., 2014). It might be that, similarly to central fatigue, interventions directed at the central nervous system could be key in the treatment of spasticity. Unfortunately, limited research has been performed on the effect of music on spasticity and further research is needed in this area (Van Criekinge et al., 2019). Our findings also have implications for people without hypertonia or other clinical conditions. For example, athletes could listen to relaxing music during intervals of strenuous exercise to fasten the recovery of the fatigued muscles.
Finally, there are some limitations to this study that should be highlighted. The first one is that we conducted our study with a healthy population. The reason to do so was the exploratory nature of this work and we provided evidence that our fatigue induction protocol could reduce the quality of participants’ movements in the drinking task. Nonetheless, in order to provide conclusive evidence that music can reduce muscle tension in people with hypertonia, it is necessary to evaluate this type of intervention in a population living with this condition. Second, past research suggests that the effectiveness of (at least some) music interventions may be mediated by music preferences. For instance, in the context of stress reduction, which is related to the induction of relaxation, several studies have reported that self-selected music is the most effective (Jiang et al., 2013, 2016; Juslin et al., 2008). In view of this, it is possible that our positive results are underpinned by participants’ enjoyment of the music style used in our study and future research should compare the effectiveness of researcher-selected music with participant-selected music. Nonetheless, it should be noted that a recent systematic review and meta-analysis on the use of music for stress reduction did not find evidence of the increased effectiveness of self-selected music (de Witte et al., 2020). Furthermore, the authors alerted to the fact that the term “self-selected music” tends to be used both when the participant freely selects pieces from their own favourite music and when the participant is asked to pick the pieces from a pre-selected list provided by the experimenter. The second strategy is particularly important when the music characteristics are central to the achievement of the desired outcomes and underpin the effectiveness of the intervention. Indeed, according to de Witte et al. (2020), nonlyrical music with a tempo of 60–80 bpm and a sound intensity level of 60 dB is the most effective for stress reduction. Also, in our study we have used two music pieces belonging to the same music genre, which, as hypothesized, lead to different outcomes. Thus, future work should not only consider participants’ individual preferences, but also guiding their choices based on the musical characteristics that support the intervention aims.
Supplemental Material
Supplemental Material, sj-png-1-mns-10.1177_20592043211015353 - Music and Hypertonia: Can Music Listening Help Reduce Muscle Tension and Improve Movement Quality?
Supplemental Material, sj-png-1-mns-10.1177_20592043211015353 for Music and Hypertonia: Can Music Listening Help Reduce Muscle Tension and Improve Movement Quality? by T. Van Criekinge, K. D’Août, J. O’Brien and E. Coutinho in Music & Science
Supplemental Material
Supplemental Material, sj-png-2-mns-10.1177_20592043211015353 - Music and Hypertonia: Can Music Listening Help Reduce Muscle Tension and Improve Movement Quality?
Supplemental Material, sj-png-2-mns-10.1177_20592043211015353 for Music and Hypertonia: Can Music Listening Help Reduce Muscle Tension and Improve Movement Quality? by T. Van Criekinge, K. D’Août, J. O’Brien and E. Coutinho in Music & Science
Footnotes
Author Contribution
All authors contributed to the study conception and design. Material preparation and data collection were performed by TVC , KDA and EC. Data analysis was conducted by TVC and EC. The manuscript was written by TVC and EC and revised by all authors. All authors read and approved the final version. Funding for this project was obtained by EC and TVC.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project has received financial support from the University of Liverpool (School of the Arts Research Development Initiative Fund) and the Flanders Research Foundation (FWO; Travel Grant no 54727). The publication of this article was supported by the University of Liverpool Institutional Open Access Fund.
Action Editor
Eckart Altenmüller, Institut für Musikphysiologie und Musikermedizin, Hochschule für Musik, Theater und Medien Hannover.
Peer Review
Matt McCrary, Hochschule für Musik, Theater und Medien Hannover.
Maria Schuppert, University of Music Wuerzburg, Music & Health.
Notes
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.