
Abstract
The aim of this systematic review was to investigate the malignant transformation of oral leukoplakia (OL) infected with Candida. Literature search was conducted using Medical Subject Heading terms ‘leukoplakia’, ‘neoplasms’, ‘Candida’, ‘malignant transformation’ and ‘oral’ and included all results until February 2017. The initial search identified 372 articles, which was consolidated to 16 articles after applying inclusion and exclusion criteria. The occurrence of candidal infection in OL ranged from 6.8% to 100.0%. Only 3 of 16 studies reported malignant transformation rates of leukoplakia with Candida infection. The overall malignant transformation rates reported in these studies were 2.5%, 6.5% and 28.7%. This review supports the contention that candidal infection promotes cellular and dysplastic changes in OL. However, further follow-up studies are recommended to confirm the role of Candida infection in malignant transformation of OL lesions.
Introduction
World Health Organization (WHO) states that the term ‘oral leukoplakia’ (OL) should be used to recognize white plaques of questionable risk having excluded (other) known diseases or disorders that carry no increased risk for cancer. 1 The estimated prevalence of OL is 2.6% (95% CI 1.72–2.74%), with an incidence rate of malignancy attributed to OL between 6.2 and 29.1 per 100,000. 2 Some risk factors that increase likelihood of malignant transformation of OL include grade of dysplasia, advancing age, female gender, leukoplakia size exceeding 200 mm2, non-homogenous leukoplakia (erythroleukoplakia, speckled leukoplakia), tobacco use, betel nut chewing, alcohol consumption, nutritional deficiency and immunosuppression. 3 –7
Studies also have identified the presence of Candida infection as a potential risk factor for malignant transformation of OL. 4,5,8,9 Some candidal species have the ability to penetrate and colonize host tissues. 10,11 A number of studies indicated invasion of candidal hyphae contributes to malignant transformation via the production of carcinogenic nitrosamines. 11,12 Nitrosamine compounds may activate specific proto-oncogenes responsible for malignant transformation. 13 However, a direct association between candidal nitrosamines and malignant transformation could not be confirmed because of confounders such as exposure to tobacco, alcohol, areca nut and immunosuppression. 11,13,14
In the published scientific literature, candidal infection in OL lesions was considered synonymous with chronic hyperplastic candidiasis (CHC), however these are now considered histologically distinct. 15 CHC was previously termed as candidal leukoplakia, however OL may not always be present in this condition. 16 CHC is therefore regarded as a separate clinical entity that is caused primarily by candidal infection. 16 In Candida-infected OL, the OL must exist as the primary lesion which is secondarily infected with Candida and the authors acknowledge this may be difficult to diagnose clinically. 17
To the best of authors’ knowledge, no systematic reviews of observational studies on Candida involvement in malignant transformation of OL exist. Therefore, this systematic review was conducted with the aim of investigating malignant transformation rates of OL infected with Candida.
Materials and methods
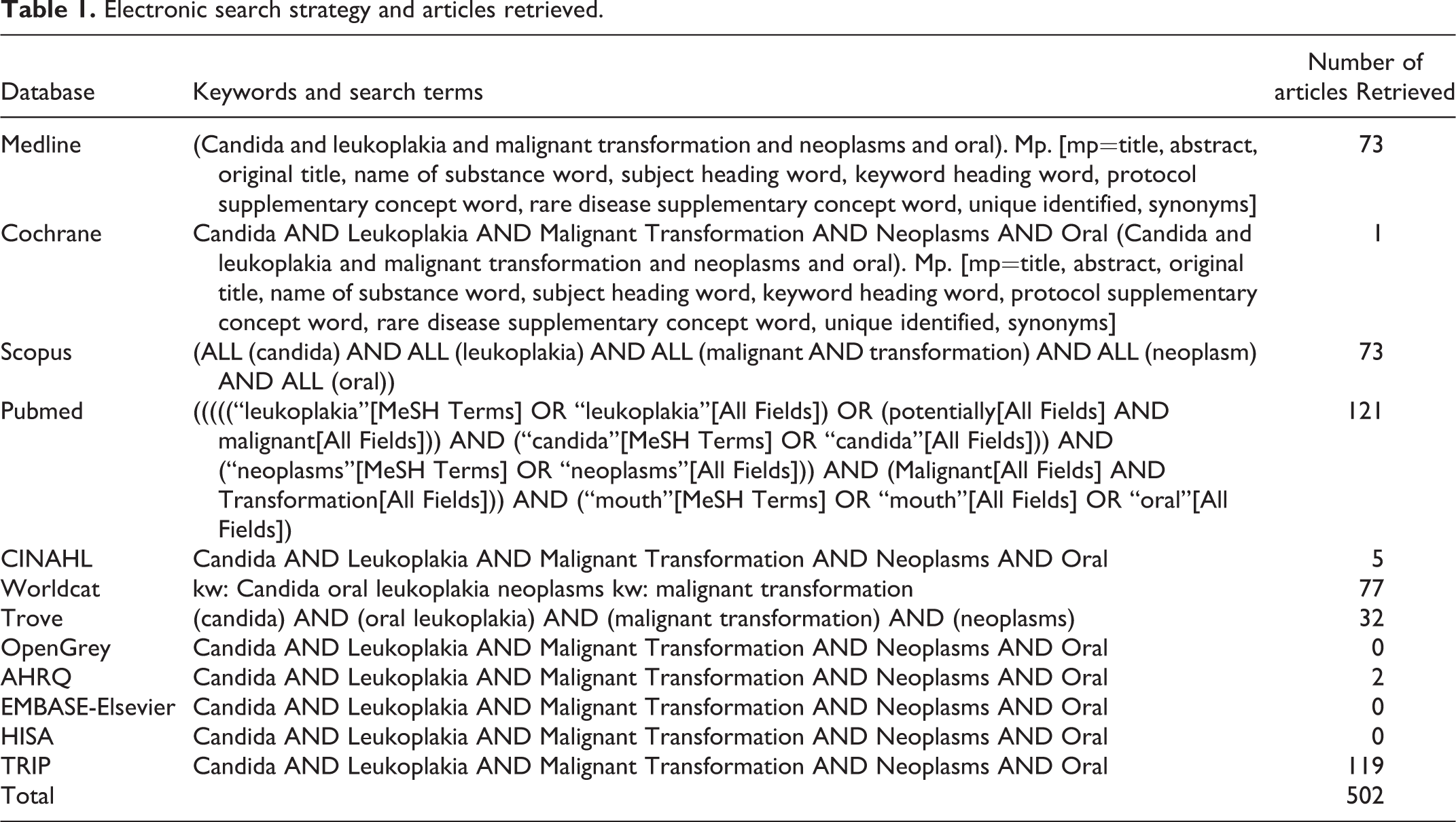
This systematic review used the Preferred Reporting Items for Systematic Review and Meta Analyses (PRISMA) guidelines. 18 The following electronic databases: Medline, Cochrane, Scopus, PubMed, EMBASE-Elsevier and CINAHL were searched. Additional searches were conducted using grey literature databases: WorldCat, Trove, OpenGrey, AHRQ, HISA and TRIP. Our database search strategy was created using the Medical Subject Heading (MeSH) terms ‘Candida’, ‘leukoplakia’, ‘malignant transformation’ AND ‘neoplasms’ AND ‘oral’. Our literature search included all available results until February 2017 (Table 1). A manual search was also completed by examining citations in included studies. Results were screened based on title and abstract, and final papers were selected in accordance with our inclusion criteria (Figure 1).
Electronic search strategy and articles retrieved.

PRISMA guideline flowchart detailing article selection process. PRISMA: Preferred Reporting Items for Systematic Review and Meta Analyses.
Our review was limited to observational studies, including prospective and retrospective cohort and case-control studies. Experimental studies, reviews, in vitro studies and case reports were excluded. Studies that did not report OL associated with Candida and malignant transformation and studies relating to CHC were excluded. Studies duplicating and reporting on the same cohort of patients with different research objectives were also excluded. Final decisions of inclusion and exclusion were agreed upon by five authors (KS, IV, IL, GL, CM), with final review by the senior author (AA). Papers included in the final analysis were reviewed by at least two independent reviewers.
Risk of bias assessment
Newcastle–Ottawa risk of bias assessment tool 19 for case-control and cohort studies was used. Although, the tool applies to case-control and cohort studies, the papers included in the study have retrospective studies as well. Hence, we have slightly modified the scale to fit into the objectives of our review. The scoring system consists of three categories that determine the bias: selection, comparability and outcome factors. A star is allocated when the study fulfil the criteria of the Newcastle–Ottawa scale.
Results
Study selection
The initial electronic search yielded 502 articles. A further 40 articles were identified through manual search and after removal of duplicates, 372 were available for initial screening. One hundred articles remained after the screening based on the title and abstracts. These articles were screened against the inclusion/exclusion criteria and 16 papers were selected for full review. The papers excluded during the screening process were case reports/case series (n = 5), animal/lab studies (n = 1), reviews (n = 26), Randomized Controlled Trials (RCT) (n = 1), in vitro (n = 6), not English (n = 3), book/chapters (n = 8), studies not linking Candida infection to OL or cellular changes (n = 23; 3 of these studies were excluded as they described CHC), studies with irrelevant outcome (n = 9) and studies with the same cohort but different study objectives (n = 2).
Risk of bias and quality assessment
Tables 2 and 3 summarize the risk of bias assessment based on Newcastle–Ottawa risk of bias tool. Scores for case-control studies and cohort studies are given in these tables. Our assessment indicates only two of cohort studies 26,33 and one case-control study 20 acquire 5 points.
Risk of bias assessment for case-control studies: modified Newcastle–Ottawa scale.
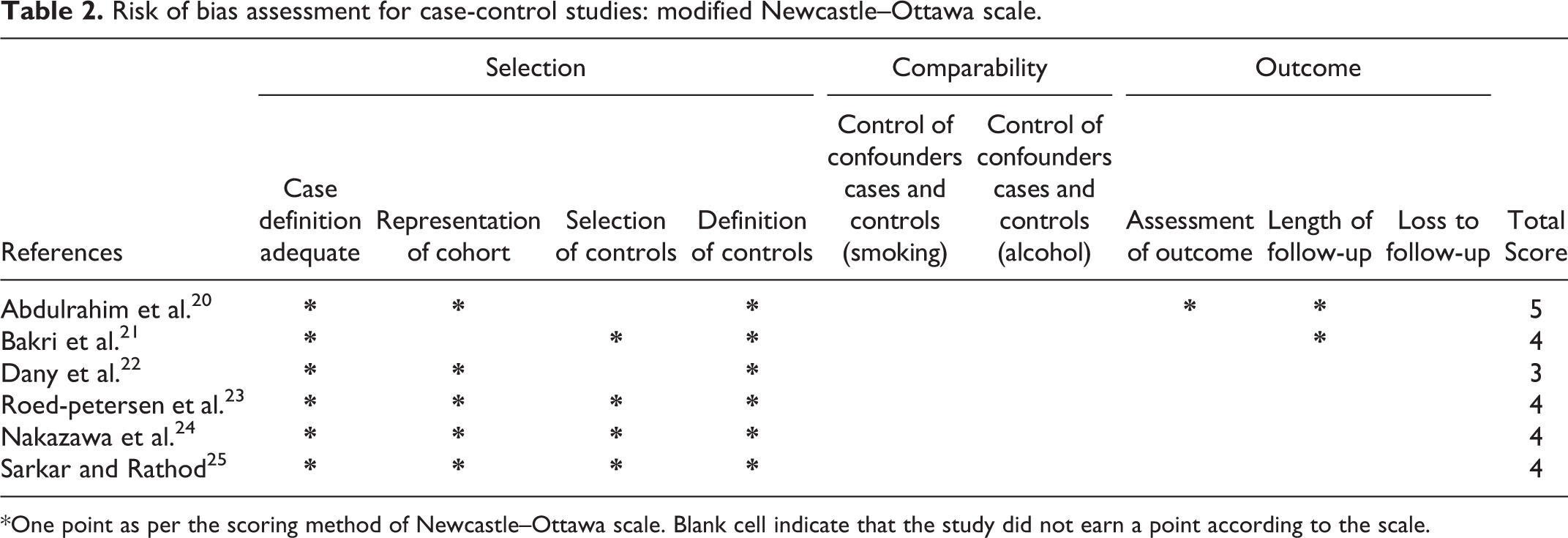
*One point as per the scoring method of Newcastle–Ottawa scale. Blank cell indicate that the study did not earn a point according to the scale.
Risk of bias assessment for cohort studies: Newcastle–Ottawa scale cohort studies.

aRetrospective study.
*One point as per the scoring method of Newcastle–Ottawa scale. Blank cell indicate that the study did not earn a point according to the scale.
Summary of results
A summary of the 16 studies included in the final systematic review is provided in Table 4.
Summary of data on epithelial changes and malignant transformation OL infected with Candida infection in OL.

N/A: Not available; OL: Oral leukoplakia.
aThe studies reporting malignant transformation of leukoplakia infected with Candida.
The incidence of candidal infection in OL ranged between 6.8% and 100.0%. Only 3 of 16 studies reported malignant transformation rates of OL lesions associated with Candida infection. 20,26,33 The overall malignant transformation rates reported in these three studies were 2.5%, 33 6.5% 20 and 28.7%. 26 The rest of the included studies were not conclusive of direct relationship of Candida infection and malignant transformation. However, they provide evidence of cellular changes associated malignant transformation in which direct association of candidal infection with epithelial dysplasia and atypia was shown.
Individual study characteristics
Individual study characteristics and the outcome extracted from each included study are given below:
Renstrup 32 in a hospital-based study in Copenhagen, Denmark, investigated biopsies of 235 OL patients (83 speckled OL, 152 homogenous OL). Leukoplakia was defined as a white patch or plaque, not less than 5 mm in diameter, which could not be classified as any other diagnosable disease. Candidal invasion was identified using Periodic Acid Schiff (PAS) staining in 55 (23%) leukoplakia lesions. Of these, 31 (56.4%) had a combination of candidal invasion and epithelial atypia. In speckled OL cases, 61.0% showed candidal invasion and 37.0% showed concurrent candidal invasion and epithelial atypia. Among homogenous OL cases, only 3.0% showed candidal infection and no atypia was detected. No follow-up data were provided on malignant transformation. The authors concluded a possible association between candidal hyphae and disorderly maturation of the epithelium in OL.
Roed-Petersen et al. 23 conducted a case-control study on 226 Danish patients diagnosed with OL. Leukoplakia was defined as a white patch, not less than 5 mm in diameter, which could not be removed by rubbing and which could not be classified as any other diagnosable disease. Candida was found in 30 of the 98 patients with OL (30.6%). Authors identified atypia in 40.0% of Candida-invaded OL biopsies (demonstrated using PAS staining), and in 67.0% of smears. However, researchers concluded the association between presence of Candida and atypia could not be confirmed. No follow-up data on malignant transformation were reported.
Daftary et al. 28 conducted a survey among 50,915 villagers across four districts in India. Of them, 723 leukoplakias were biopsied and examined for the presence of Candida. Leukoplakia was defined as a raised white patch of the oral mucosa measuring 5 mm or more which could not be scraped off and which could not be attributed to any other diagnosable disease. PAS staining confirmed the presence of Candida in 49 (6.8%) of the lesions (27 homogenous, 15 ulcerated, 7 speckled). Atypia was associated with candidal infection in seven (14.3%) non-homogenous OL cases (two ulcerated and five speckled). No atypia was detected in homogenous OL. Forty-three patients with Candida-infected OL were tobacco smokers, a known risk factor for malignant transformation. The authors were unable to demonstrate a statistically significant association between atypia and candidal invasion of OL. No follow-up data were provided on malignant transformation.
Banoczy and Sugar 26 followed up 520 OL cases in Hungary over 25 years. Leukoplakia was defined as an elevated white patch on the oral mucosa that could not be scraped off and could not be classified as any other type of disease. Candida infection was present in 13.5% of cases (n = 70) of OL. Thirty-eight percent of cases regressed while 53.0% progressed. Regression was defined as a clinical decrease in size and severity of the lesion whereas progression was an increase in size and severity. Of the 70 cases infected with Candida, 20 cases transformed to cancer with a malignant transformation rate of 28.7%. The study concluded a link existed between Candida-infected OL and malignancy, but early detection and treatment has potential to inhibit this progression.
Silverman et al. 33 followed a group of 257 OL patients (125 men and 132 women) in California, USA. Leukoplakia was defined as a clinical white patch or plaque on the oral mucous membranes that could not be removed by scraping and could not be classified clinically or microscopically as another disease entity. All patients had a lesion at least 1 cm in size and were observed for a minimum of six months. Lesions were subjected to microscopic examination (after PAS staining) and culture for Candida isolation. Cultures showed that 31% (n = 78) of the patients were positive for Candida. Two of these patients subsequently developed carcinoma during the follow-up period, resulting in a malignant transformation rate of 2.5%. The study demonstrated an association between Candida and malignant transformation of OL. However, exclusion of lesions smaller than 1 cm may have led to under-reporting of Candida-infected OL.
Krogh 31 studied 12 Danish patients with OL lesions that were infected with Candida and discussed the role of endogenous nitrosation and malignant transformation. The authors did not provide a definition of OL. The cases included in this study were a subgroup of smears identified from their earlier report in 1987. 10 Five of the 12 lesions (41.7%) showed epithelial dysplasia (two mild, two moderate, one severe). The authors found that higher levels of Candida were associated with increased dysplasia and provided further evidence in support of their hypothesis that yeasts play a causal role in oral cancer by means of endogenous nitrosamine production. However, small sample size is a major flaw of this study. Hence, the authors recommended more studies to determine the exact influence of Candida on OL malignant transformation.
Vučković et al. 34 reported a clinical and histological study conducted in Serbia on 30 biopsies from 30 patients with oral mucosal lesions (21 female, 9 male). Leukoplakia was defined as a range of nonspecific white lesions, whose appearance does not generally correlate well with histopathologic changes. Twelve lesions were diagnosed as OL and were stained with Haematoxylin and Eosin (H&E) and PAS for the identification of Candida and cellular changes. Three leukoplakia lesions (25.0%) presented with Candida infection. Of these lesions, mild dysplasia was detected in one case (33.3%). This study was limited by a small sample size and the authors noted that this reduced their ability to establish a link between Candida infection and malignant transformation of OL.
Nakazawa et al. 24 analysed 175 potentially malignant lesions and diagnosed 44 with OL in a university-based study in Japan. Leukoplakia was defined as a white lesion of the oral mucosa that cannot be characterized as any other definable lesion. Candida was detected using exfoliative cytology and PAS staining of biopsies. Twenty-six OL lesions (59.1%) were positive for Candida. Of the 16 lesions subjected to a histopathological assessment showed Candida in 10 cases (62.5%). No rationale was provided as to why the histopathological analysis was limited to 16 lesions. Immunohistochemical analysis revealed cellular markers of malignant potential, including p53 mutation (positive C. albicans 30.6%, negative C. albicans 15.3%), Ki-67 (positive 21.5%, negative 17.2%) and COX-2 (positive 8.5%, negative 3.4%). Cellular abnormalities were greater in Candida-infected cases, indicating higher DNA alterations and increased malignant potential.
Chiu et al. 27 conducted a retrospective study in Taiwan on 136 OL patients. Leukoplakia was defined as a chronic white mucosal macule which could not be scraped off, could not be given another specific diagnostic name and did not typically disappear with removal of a known etiologic factor. Two groups were formed: group A consisted of 31 patients who had multiple OL (73 lesions) and group B consisted of 105 patients with single OL (105 lesions). All lesions were excised and specimens were stained with PAS for the detection of candidal infection. Candida was found in 35 lesions (47.9%) in group A and 20 lesions (19.0%) in group B. Dysplasia was present in 10 Candida-infected cases (28.6%) in group A and 4 cases (20.0%) in group B. It was evident that multiple OL lesions showed higher grades of epithelial dysplasia and were more likely to become infected with Candida.
Dany et al. (2011) 22 conducted a case-control study in a sample of hospital-based OL patients in Chennai, India. The test group comprised of 30 patients with OL lesions and 30 subjects (age and sex matched) in the control group. This control group comprised individuals with no mucosal lesions (group I) and with mucosal lesions (group II). Candida was identified using PAS staining.
Leukoplakia was defined as a predominantly white lesion of the oral mucosa that cannot be characterized as any other definable lesion. OL lesions were categorized into four stages: stage 1–4 (rationale for this staging was not provided). Eleven cases (37.0%) of OL were positive for Candida. Of these cases, two presented without dysplasia (18.0%), three showed mild dysplasia (27.0%) and six cases showed moderate dysplasia (54.5%). The relationship between the presence of Candida and different grades of dysplasia was not significant (p = 0.06). However, a statistically significant relationship was seen between the presence of Candida and the stage of the OL lesion (p = 0.01). Candida was found in two stage 1 lesions (14.3%), three stage 2 lesions (42.9%) and six stage 4 lesions (66.7%).
Abdulrahim et al. 20 collected biopsies, oral rinses and smears from 78 OL patients (40 males, 38 females) in Ireland. Leukoplakia was defined using the 2007 WHO definition of oral white patches or lesions of questionable risk, having excluded other known diseases that carry no increased risk for cancer. 1 Biopsy results (with PAS staining) showed Candida infection in 31 cases (39.7%). Candidal infection was also found via other sampling methods (55 oral rinse, 50 smears). Twenty-eight of the Candida-infected biopsies exhibited dysplasia (90.3%). Four cases showed mild dysplasia (12.9%), 14 showed moderate dysplasia (45.2%) and 10 showed severe dysplasia (32.3%). In this study, two cases (6.5%) of Candida-infected OL were found to have malignant transformation.
Hebbar et al. 29 conducted a study in India with 50 participants (30 male, 20 female) ranging from 18 to 75 years of age. Twenty-three OLs were present (15 homogenous, 8 non-homogenous). The authors did not provide a definition for OL. Seven (87.5%) non-homogenous OLs were positive for fungal growth after culturing and PAS staining. No data were available for fungal infection in homogenous OL. The authors noted that a small sample size was a limitation of their study but concluded that Candida infection may play a role in the malignant transformation of OL. However, they also postulated that increased Candida proliferation in these lesions may have been a result of the altered epithelium.
Wu et al. 35 investigated 396 cases of OL from Eastern China between January 2005 and December 2007. OL was defined using the 2007 WHO definition of a white plaque of questionable risk having excluded (other) known diseases or disorders that carry no increased risk for cancer. 1 Samples were stained with H&E and PAS for identification of candidal hyphae. Candida-infected OL was found in 59 patients (29 female, 30 male). Thirty-three samples showed signs of dysplasia (55.9%). Significant risk factors for candidal infection in OL included presence of dysplasia, age over 60 years and lesions on the tongue. The authors concluded patients with OL were more susceptible to Candida infection.
Bakri et al. 21 analysed 28 archival OL biopsies in Malaysia. The authors did not provide a definition for OL. Ten cases were infected with Candida (identified with PAS staining) and nine showed high expression of C. albicans ADH1 mRNA. The authors identified C. albicans as the predominant species associated with OL (p = 0.001). After a 3-year follow-up, one case of OL (with epithelial dysplasia) was diagnosed with oral squamous cell carcinoma, however Candida was not detected in this lesion. The study was limited by a small sample size and provision of antifungal treatment which possibly masked the involvement of candidal infection in OL. The authors concluded that C. albicans was the main Candida species associated with OL, however they did not provide any data on its role in the malignant transformation of these lesions.
Sarkar and Rathod 25 reported results from a hospital-based study in India on 61 patients (40 OL, 21 control). OL was defined as a predominantly white lesion or plaque of questionable behaviour having excluded, clinically and histopathologically, other definable diseases. Twenty-three cases were diagnosed as homogenous OL while 17 were diagnosed as non-homogenous. Candida infection was detected via direct microscopy, culture and histopathology. Tissue sections were stained with Grocott’s Methenamine Silver (GMS). Nineteen (47.5%) direct OL smears showed Candida compared to three controls (14.3%). Eighteen cases of OL cultures (45.0%) showed Candida compared to one control (4.8%). Candidal invasion was greater in non-homogenous OL (smear 64.7%, culture 64.7%) compared to homogenous OL (Smear 34.8%, Culture 30.4%). Dysplasia was present in 15 cases of the Candida-infected OL (78.9%). There was no significant difference in Candida detection between non/mildly dysplastic and distinctly dysplastic lesions (p > 0.05).The authors concluded a larger sample size was required to accurately demonstrate the relationship between Candida and dysplasia.
Hongal et al. 30 carried out a study in India on 70 cases of potentially malignant lesions, which included 29 cases of OL. The authors did not provide a definition for OL. To evaluate for fungal hyphae, tissue sections were stained with H&E, PAS and GMS. Twelve cases of OL (41.4%) were positive for fungal hyphae. Dysplasia was present in all 12 cases (100%) of Candida-infected OL. A significant association was seen between presence of fungal hyphae and degree of dysplasia. The authors acknowledged a larger sample size was required for future studies.
Discussion
Candida is a genus of fungi that is frequently isolated within the oral microbiome. C. albicans is considered to be the most common opportunistic pathogen in this genus. 5 Follow-up studies have noted the presence of Candida in OL lesions and postulated that this may be linked to an increased risk of malignant transformation. 7,30 This review aimed to investigate the role of candidal invasion in the malignant transformation of OL.
The studies included in this review assessed Candida infection using smears, oral rinses and staining of biopsies with PAS or GMS (Table 4). Some studies 19,20–22,25,26,31,32,34 used a combination of tests to confirm the presence of Candida. Included studies identified that the prevalence of candidal infection in OL lesions ranged between 6.8% and 100.0%. 23,28 The authors’ acknowledge that the different methodologies used across studies to identify Candida in the lesions has likely resulted in under or over-reporting of the incidence of infection. 26,36 The presence of Candida was substantially less in biopsy results when compared to smears, suggesting that while Candida often exists superficially, true hyphal invasion into the lesion is less common. 36 Though this review analyses the effects of candidal invasion in OL lesions, further studies may elect to compare whether superficial Candida infection and the depth of penetration into the OL lesion also plays a role in malignant transformation.
Epithelial changes that were observed in the studies reviewed include varying grades of dysplasia and cellular atypia. Grades of dysplasia ranged from mild to carcinoma-in-situ, and ranged from 20.0% to 100.0%. 22,24,25 One study 29 noted dysplasia was higher in OL lesions infected with Candida (55.9%) compared to OL lesions without candidal infection (33.5%). This finding suggests that OL lesions that are infected with Candida experience increased dysplastic changes, placing them at higher risk of progressing to malignancy. Cellular atypia was another common finding, and ranged from 14.3% to 56.3% in Candida-infected OL lesions. 23,33 Three studies 22,23,33 found non-homogenous lesions (e.g. speckled leukoplakia, erythroleukoplakia) had a higher prevalence of Candida compared to homogenous leukoplakia, however the full extent of this association was not established. Although, most of the studies did not provide follow-up data on malignant transformation, all studies showed presence of dysplasia and cellular atypia in lesions infected with Candida. These findings are typical of early changes observed in oral epithelial carcinogenesis. Additionally, candidal invasion was found to be higher in speckled OL lesions, which have a higher established risk of malignant transformation. 3,19,33
There are several proposed cellular mechanisms whereby Candida can induce dysplastic and malignant changes in the oral epithelium. 10,28,37 These include: the production of endogenous nitrosamines, acetaldehydes, and over-expression of p53, Ki-67 and COX-2 factors. 34,38,39 The production of nitrosamines such as N-nitrosobenzylmethylamine have been found to induce tumour development in animal models. 40 For candidal species, the ability to induce tumour formation via this process lies in their ability to deliver these nitrosamine compounds into the epithelial tissue via hyphal invasion. 10 A secondary mechanism by which Candida can influence carcinogenesis is via acetaldehyde production. Gainza 39 found C. albicans to display a strong capacity to produce acetaldehyde, a carcinogen, from precursors found in the oral cavity. Candidal organisms can metabolize ethanol and glucose to produce acetaldehydes in high amounts, especially when coupled with smoking and alcohol consumption as patient risk factors. 38 Acetaldehyde has been shown to possess mutagenic qualities in DNA when present in sufficient concentration, bearing relevance for the ability of Candida to induce oral cancer development. 41,42 These underlying chemical and cellular mechanisms highlight the ability of Candida to influence malignant and cellular changes in OL and are potential avenues for future research.
The over-expression of p53, Ki-67 and COX-2 are some of the additional mechanisms by which Candida can influence malignant transformation in OL. p53 and Ki-67 are markers of cellular proliferation, and their over-expression is well established in malignant lesions. 43 COX-2 is an enzyme associated with release of prostaglandins, and is markedly increased in inflammatory sites. A study by Sobolewski et al. identifies COX-2 as a contributing factor in the development of tumours through its influence on cell proliferation, cell death, and tumour invasion. 44 A study in this review by Nakazawa et al. found the presence of Candida was associated with a significant increase in p53, Ki-67, COX-2 and DNA aneuploidy in OL lesions. 24 While a causative relationship could not be established, these results strongly implicate the role candidal infection plays in the malignant transformation of OL through the upregulation of inflammatory and proliferative changes in the epithelium.
A number of methodological disparities among the studies included in this review were identified. Several studies failed to define terms and classification criteria, affecting the consistency of analysis between studies included in this review. As mentioned in the methodology, studies relating to CHC were excluded from our review. Three articles were removed purely on the basis of analysing CHC rather than Candida in OL. Of these, Lopez et al. 45 noted dysplastic changes in 42.1% of CHC lesions, and suggested that CHC lesions have malignant potential. However, they recognized a difference between lesions with a primary aetiology of candidal infection and OL lesions which were secondarily infected with Candida. The authors noted that Candida may be isolated and eliminated from non-homogenous cases of leukoplakia, which often leads to a transformation from a high-risk (non-homogenous) to a low-risk (homogenous) form. The second excluded paper by Darling et al. 46 found elevated levels of p53 in CHC lesions that did not show any signs of dysplasia or malignancy. Their findings suggested that CHC lesions had increased potential for malignant change, however the authors recommended further clinical studies to support their findings. The final paper by Arruda 8 analysed predisposing factors for CHC, but did not provide any data on cellular changes or malignant transformation.
The authors acknowledge that excluding CHC from this review may have caused under-reporting of candidal infection in OL as the lesions are often clinically indistinguishable and are erroneously reported interchangeably. 47 We plan to undertake a separate review analysing the malignant potential of CHC lesions to account for this discrepancy in the literature. A study by Gracia et al. notes that CHC lesions should completely resolve with antifungal treatment, whereas OL lesions will usually persist afterwards, thus verifying the conditions as separate. 17 In terms of clinical practice, treatment with topical or systemic antifungal agents (e.g. nystatin, miconazole) may be of use in separating CHC from OL lesions, allowing for the OL to be managed as appropriate.
Additional terms that were used inconsistently between studies included: epithelial atypia, cellular changes and dysplasia. 23,24,32,33 One study defined epithelial atypia as lesions with varying degrees of hyperparakeratosis, inflammation, oedema, hyperplasia, acanthosis, dyskeratosis and atrophy. 32 However, this is not consistent with other studies that used the term epithelial atypia. 23,28,31 Similarly, there were inconsistencies between the histological classification of OL lesions. As the publication dates of the included articles spanned numerous decades, the terminology used to describe OL varied, which reduced uniformity in their evaluation. Classification of OL included simplex, speckled, erythroleukoplakia, erosive, verrucous and homogenous or non-homogenous. 26,29,31 As these terms were not used consistently, it made comparison difficult and limited the ability to assess extent of cellular and malignant changes in OL as a result of Candida invasion.
Limitations
Limitations of this review include lack of follow-up data detailing malignant transformation, weak methodology of included studies, inconsistences in the terminology and heterogeneity in analysis. We also limited the studies to papers published in English language only and this limits interpretation and representation of global literature on the topic. Only three of the 16 studies included in this systematic review identified OL lesions progressing to malignant transformation. Most studies did not provide follow-up data of patients. Therefore, definite association between Candida associated dysplastic changes and progression to malignancy is difficult to establish. Furthermore, while most studies isolated C. albicans in samples, there was limited analysis regarding other species of Candida that may play a role in dysplastic and malignant changes. As indicated by the quality analysis most of the studies included are of poor quality in terms of bias. This limits the interpretations of the findings.
Conclusions
To the best of our knowledge, this is the first systematic review conducted on the influence of leukoplakia Candida infection on their malignant transformation of leukoplakia lesions. The results of this review suggest that candidal infection may play a role in dysplastic and malignant transformation of OL lesions. However, further follow-up studies are required to confirm this finding. In terms of clinical practice, the authors suggest possible benefit to investigating OL lesions for candidal invasion, and controlling the infection with appropriate antifungal therapy to reduce risk of malignant and dysplastic changes.
Footnotes
Acknowledgements
The authors would like to thank James Cook University and to JCU College of Medicine and Dentistry staff for assisting with the sourcing of articles.
Author contributions
All authors contributed to the development of the study protocol, literature search, review and writing the manuscript. The senior author (AA) supervised the study and edited the manuscript. All authors reviewed the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.