
Abstract
Background:
Clinicopathological studies have revealed some distinct anatomical variations in the clinical presentation of oral leukoplakia (OL). Screening studies have shown that gingival leukoplakia (GL) to be more common among the Japanese.
Objective:
A hospital-based case-control study was undertaken among patients diagnosed with OL to compare clinico-pathological data between GL and OL affecting other sites (n-GL).
Methods:
One hundred fifty-one subjects attending four city hospitals in Japan diagnosed with OL were recruited to this study. OL was diagnosed by World Health Organization criteria. They were interviewed for risk factors, clinical presentations were charted and investigated by patch testing for allergy to dental materials and by biopsy for dysplasia.
Results:
Eighty-eight with GL and 63 with n-GL were included in the study. GL lesions were predominantly white (93%) though n-GL leukoplakia had red (speckled) foci in 26%. Eighty percent of GL were seen in association with prosthesis or restorations. There were no significant differences by age or in tobacco and alcohol use in the two groups. Metal allergy test was positive in 58% of the GL but was not significantly higher compared to the n-GL (41%). Histopathological features showed that inflammatory cell infiltrate was predominant in n-GL group (p = 0.021). Higher dysplasia grades were also found in n-GL (p = 0.018). During follow-up, nine oral cancers (14%) were detected in n-GL group and among GL cases four developed oral carcinomas (5%) (p = 0.043). Cox hazard regression analysis revealed that after adjusting for age and sex, GL group was found to have a lower malignant risk, with a hazard ratio of 0.89 (95% CI: 0.51–1.04) when compared to n-GL.
Conclusions:
GL was more benign compared to n-GL in Japanese subjects, though risk factors appear similar. Further study is warranted to ascertain whether trauma may play an important role for hyperkeratinization of gingival tissues and possible evolution of GL to proliferative verrucous leukoplakia in later years.
Introduction
Oral leukoplakia (OL) which during its natural history could develop to oral squamous cell carcinoma is classified as an oral potentially malignant disorder. 1 Several causal factors for this disease are known, smoking, excess alcohol drinking and betel quid chewing (among Asians) 2 ; the role of alcohol in the aetiology of OL, with particular reference to moderate alcohol drinking is still uncertain. 3 Chronic infections by fungi and viruses are being debated. 4 Moreover, published data suggest significant geographic differences. Some leukoplakias have an unknown cause (idiopathic) and are considered to have a higher risk for malignant transformation. 5,6 Gingival leukoplakia (GL) considered for this research may well fall into this category. Primary research on risk factors of this entity has been meagre. Although tobacco-associated OL may be effectively managed by smoking interventions 7–9 for idiopathic leukoplakia which occurs in non-smokers, quitting smoking is not a considered option.
In Europe, most prevalent sites of OL are the lateral borders of tongue, the commissure and/or the buccal mucosa. 10–12 However, according to an epidemiological study in Japan, gingivae/alveolar were more common sites and detected particularly among non-risk groups. 13 With regards to the prevalence of leukoplakia in 1990s, Ikeda et al. 14 performed pioneering works for mass screening of oral mucosal diseases in a selected Japanese population and concluded that gingival and alveolar ridge (34%) were most prevalent sites followed by buccal mucosa (28%) and labial commissures (11%). However, different site distributions for OL have been reported worldwide, 15–19 aetiological factors attributable to site-specific distribution has not been elucidated so far. Clinico-pathological features of GL have not been documented in any detailed study.
The objective of this study was to explore the risk factors of GL among a Japanese population. We investigated a cohort of patients with GL and their clinico-pathological features were compared by the case-control method with patients presenting with OL affecting other sites (n-GL) detected during the same time period.
Materials and methods
Among 204 subjects, newly diagnosed or those who previously diagnosed as OL and have been followed up regularly in four city hospital in Japan, from March 2009 to May 2012, 151 subjects were recruited to this study. The inclusion criteria were by World Health Organization (WHO) criteria, 1 clinically diagnosed as homogenous or non-homogenous leukoplakia and pathologically confirmed. Eighty-eight of 151 cases (58.3%) were GL and 63 cases (41.7%) were n-GL (Figure 1). The cases who were pathologically diagnosed as a carcinoma in situ or microinvasive carcinoma was excluded from the study. This study was performed in compliance with the Declaration of Helsinki, and written informed consent was obtained from all participants recruited to this study. Non-gingival sites or if OL predominantly affected other sites, these were regarded as n-GL (Figure 2). Any friction related keratosis observed on alveolar ridge (Figure 3) due to tooth brushing or another were excluded from the study, as per WHO definition for diagnosis of OL. 1

Clinical illustrations of subjects – Leukoplakia affecting gingivae/alveolar ridge. (a) 79-year female with no reported history of risk factors. Homogenous appearance, close to a metal crown. No epithelial dysplasia, fungal test+, patch test+ (zinc (Zn) and manganese (Mn)); (b) 70-year male who reported smoking and excess drinking. Homogenous appearance and contact to metal crown. No epithelial dysplasia, fungal test−, patch test+ (Zn, Mn, cobalt (Co), and mercury (Hg)); (c) 51-year male reporting smoking and drinking habits, homogenous appearance and showing contact with metal crown. No epithelial dysplasia, fungal test+, patch test+ (Zn and Co); (d) 60-year male who was an ex-smoker, regular drinker, homogenous appearance, multiple lesions, close to metal crown. No epithelial dysplasia, fungal test−, patch test+ (nickel, tin, Co, platinum, and chromium).

White patch extending from retromolar area to the hard palate in a 73-year male. He is regular drinker (>21 U/W) and quitted smoking 10 years ago. Epithelial dysplasia: mild; fungal test−, patch test−.

Bilateral alveolar ridge keratosis. Bilateral keratotic lesions on the retromolar regions associated with linea alba on the left buccal mucosa (a and b). This white lesion is thought to be frictional related clinically and excluded from the study.
Study subjects were interviewed on risk factors; smoking and drinking, investigated by patch testing for dental materials. Location of prosthetics and types of dental alloys were recorded. We documented risk factors for the GL and n-GL groups and compared demographic, clinical characteristics; lesion site, colour, size, clinical types and clinical diagnosis. The size of the lesions was determined by the measurement of any morphologically altered area that were clinically visible. 19 Calibrations for the clinical diagnoses and collecting the data have been made among the participating hospitals before starting the study. The study has been approved by the Institutional Review Board (IRB) in Okazaki City Hospital (IRB No. 162).
Relationship between dental prosthesis and target lesion, particularly presence or absence of amalgam fillings, crowns, prosthetic materials, resin denture or resin filling was charted. For some prosthesis, we were unable to specify the materials used. Metal prosthesis were divided into metal bond crown, metal crown and no crown. We divided alloys into gold metals (18 K ≤ or gold plus palladium) and others, including non-precious metals by colour tones of crowns, although it was rather difficult to identify materials used exactly. Metal allergy testing was performed among selected subjects who volunteered. Patch testing to dental materials was carried out in our dermatology departments in the hospitals or dental allergy clinic in the university hospital. The test substances were 2% cobalt chloride, 5%copper sulphate, 0.5% potassium dichromate, 2% iron sulphate, 1% manganese chloride, 1% molybdenum salt, 5% nickel sulphate, 1% titanium oxide, ammoniated mercury 1% and amalgam 5%. The first and second evaluations were performed 24 and 48 h after applying the patch, and if a mildly positive result was detected, the third evaluation was 1 week later to distinguish equivocal reactions. Laboratory tests for candidal colonization were done by taking a swab using a sterile cotton swab of the affected area which was placed onto an agar plate for culture of Candida albicans, and culture tests were performed.
All subjects had a diagnostic biopsy. If the lesions extended to two or more sites, we selected the biopsy site where the lesion was predominant and/or more severely affected site. Toluidine blue staining was used as an adjunct in some cases to evaluate the most affected area, representing the site for biopsy. Any dysplasia observed by microscopy was recorded using haematoxylin and eosin-stained sections. 20 Some clinico-pathological data were missing due to loss of samples. Two oral pathologists (HS and SM; co-authors) independently scored dysplasia grades in a blind fashion. If there were any differences, the assignment of a grade was agreed following discussion. The dysplasia grade was divided into: no dysplasia, mild, moderate and severe dysplasia. The presence of inflammatory cell infiltration was graded; none, perivascular, lichenoid and lymphocytic or plasmoid. The period for malignant transformation was determined from the time that a suspected lesion was clinically and pathologically diagnosed as a carcinoma from the time of initial diagnosis. Both microinvasive and invasive carcinomas in biopsy were defined as transformations. Those lost to follow-up were coded by the date of last visit to arrive at censored data. Observations were terminated on 31 March 2013.
Statistical calculations were carried out using the statistical package, JMP version 8.0.2 for Windows (SAS Institute, Cary, North Carolina, USA). Each item was evaluated between GL and n-GL group with the χ 2 (Fisher’s exact test) and Student’s t-test. We assessed the cancer risk between two groups with odds ratio and Cox proportional hazards regression model. All statistical tests were two-sided, and a significance level of 0.05 was used throughout.
Results
Demographic characteristics of the subjects showed no significant differences in smoking and drinking habits in the two groups (Table 1). In neither group, did they report regular use of alcohol containing mouth washes nor the use of smokeless tobacco products.
Demographic and clinical characteristics between GL and n-GL.
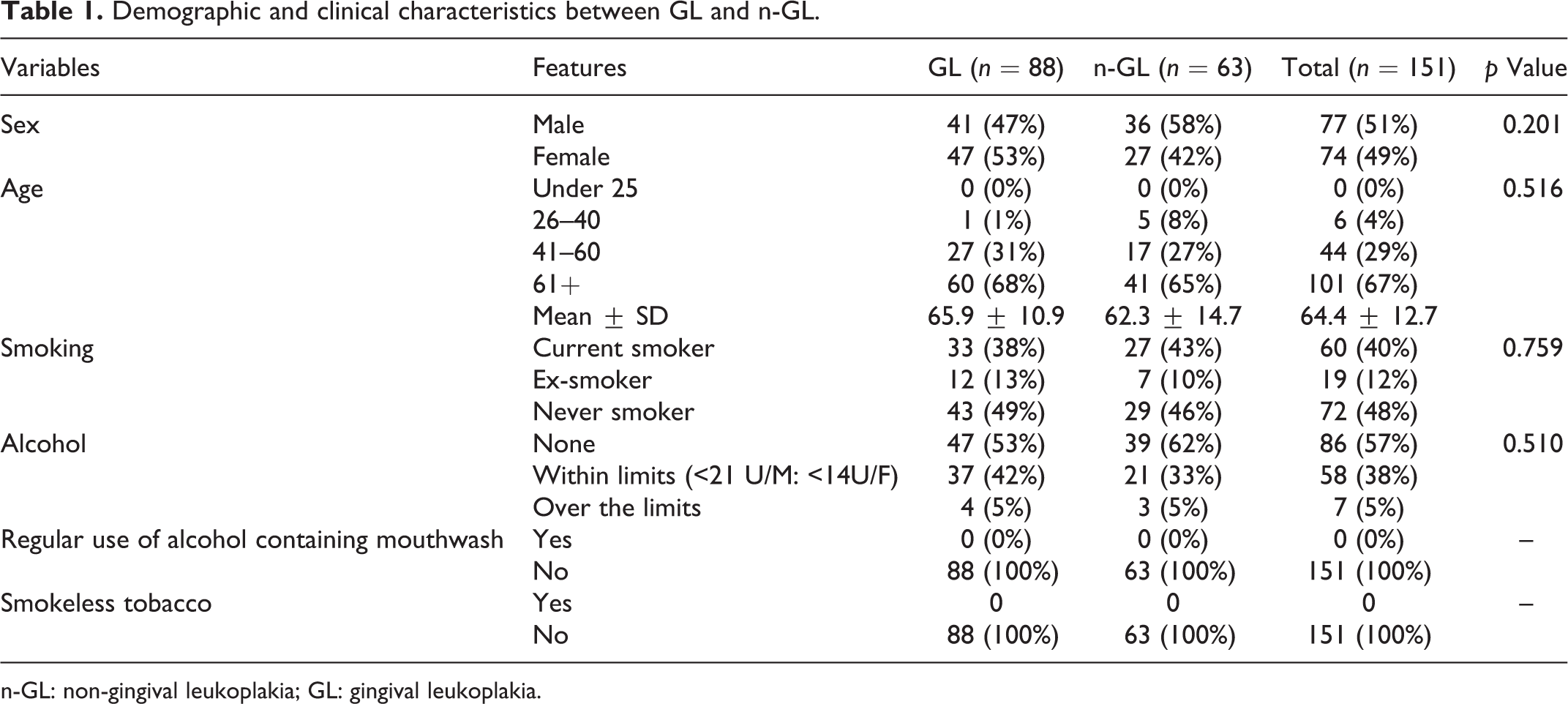
n-GL: non-gingival leukoplakia; GL: gingival leukoplakia.
In GL group, 70 of 88 cases (80%) were single lesions (Table 2). Among those, 75% were gingival alone. Thirteen percent of GL cases also had other affected oral sites additional to gingivae/alveolar lesions. Most prevalent sites of the n-GL was tongue followed by buccal, palate and floor of mouth. Seven cases of oral lichen planus were included in the n-GL group. These cases were atypical and clinically presented as plaque like OL. Histopathologically, these cases were classified as hyperkeratosis, with a lichenoid reaction with or without dysplasia.
Clinical characteristics between GL and n-GL.

[]: number of multiple, duplicate+; n-GL: non-gingival leukoplakia; GL: gingival leukoplakia; N/A: not applicable; DLE: Discoid lupus erythematosus.
GL lesions were predominantly white (93%) compared to n-GL (74%) (p = 0.002). Most of the GL affected buccal sites (73%). Clinically, 93% of GL were more homogenous than found in n-GL (66%; p < 0.0001). N-GL was likely to have red foci or speckled (26%) compared to GL (7%). GL was smaller (<200 mm 2 ) in extent (81%) than in n-GL (43%) (p < 0.0001).
In a sub group of patients, the frequency of the positive candida test was higher in n-GL (34%) than in GL (27%; p = 0.525; Table 3). Metal allergy test was positive in 58% of the GL group but was not significantly higher compared to the n-GL group (41%). Eighty percent of GL were seen in association with prosthesis (p = 0.248) and 26% were close to amalgam fillings. Any presence of metal prosthesis in the mouth was higher in GL (85%) than in n-GL (75%) but this was not statistically significant. Gold plus palladium metals closest to lesions were predominantly found in GL (81%) than in n-GL (70%; p = 0.486). Closeness to resin denture or resin filling was higher in GL (13%) than in n-GL (9%) but not statistically significant.
Dental characteristics between GL and n-GL.a

Pd: palladium; n-GL: non-gingival leukoplakia; GL: gingival leukoplakia.
aCandida and metal allergy test are performed in selected subjects who accepted it. Some prosthetics are not able to specify materials used clinically.
The frequency of any epithelial dysplasia was higher in n-GL (55%) than in GL (37%) (Table 4). The epithelial dysplasia score was significantly different between two groups (p = 0.018). Histopathological features showed that inflammatory cell infiltrate was frequently observed in n-GL group (100%) than in the GL group (89%) (p = 0.021). For the inflammation pattern, lymphocytic or plasmoid was higher in n-GL (55%) than in GL (42%; p = 0.030). Among lesions that were close to restorations or prosthesis, there was no significant difference in lichenoid inflammatory cell infiltrate between two groups; 31% (22/70) in GL and 33% (15/45) in non-GL, respectively. With regard to malignant transformation of OL, n-GL group developed nine cases of oral cancer (14.3%) with a mean observation period of 79 months. On the other hand, the GL group had four cases (4.5%) with mean observation period of 27.5 months. (p = 0.043). Figures 4(a) and (b) illustrate a case that developed squamous cell carcinoma arising from GL.
Pathological results between GL and n-GL.


A case of malignant transformation of gingivae/alveolar ridge leukoplakia. A 78-year female who had no risk factors. Clinically homogenous leukoplakia with a smooth surface (a). Epithelial dysplasia: none, fungal test+, patch test: N/A, close to metal crown. Thirty-six months later, malignant change has developed on the attached gingiva (b).
Under the median observation periods of 55.9 months in GL and 62.6 months in n-GL group, the estimation of odds ratio for malignant transformation of GL group was 0.82 (95% CI: 0.58–1.16) when compared to n-GL group. Cox proportional hazard regression analysis revealed that after adjusting for age and sex, GL group was found to have a low malignant risk, with a odds ratio of 0.89 (95% CI: 0.51–1.04) when compared to n-GL group.
In the subgroup analysis for GL, we divided them clinically into homogenous, non-homogenous and verrucous types, and evaluated them by these variables. There were significant differences in frequency of malignant change, clinical diagnosis, lesion colour, clinical size and positive candida test (Table 5). Non-homogenous type was likely to present with more red foci, larger size, more frequent candidal colonization and the malignant transformation rate was higher compared to homogenous type.
Relationship between clinical type of gingival leukoplakia and variables.

Pd: palladium.
Discussion
This study was focussed on the anatomical site distribution of OL in this Japanese population seen in Oral and Maxillofacial clinics. Table 6 shows a summary of the prevalent sites of OL previously published by other authors around the globe. Apart from two Japanese studies that scored gingival location and alveolar ridge as the highest prevalent oral sites for OL only, one other study has recorded similar findings. This was a cohort study carried out in the United States on 16,128 adults recording 38.8% had GL. 21 In this US study, Sheifele et al. 21 suggested that there was significant relationship between use of smokeless tobacco and GL in their cohort. In our study, none of our population had smokeless tobacco habits. Comparing anatomical locations recorded in population-based studies in United States, it is interesting to note some discordant results; Bouquot et al. 18 reporting lip vermillion as the prevalent site of OL which is not apparent in the Sheifele et al. study, published 17 years later.
Prevalent site of oral leukoplakia.

PS: prevalent site.
In a further national survey in United States, 22 examinations were performed on 17,235 people aged 17 years and older, of whom 4801 (27.9%) had white (keratotic) lesions. Among those, frictional white lesions were frequent (2.67%). The result suggests that some frictional lesions might be included in a screening examination and miscoded as OL. Excessive tooth brushing, movement of oral prostheses or constant mastication on alveolar ridges may produce frictional keratoses. It is not clear whether previous epidemiological studies from Japan 13,14 had included frictional keratoses of gingivae among their category of OL diagnosis, resulting in a high prevalence of GL. This anomaly is elegantly highlighted by Mignogna et al., 23 in a study of 159 subjects in Italy in whom 14 (9%) had frictional keratoses of gingivae. In all 14, these keratoses disappeared on discontinuing their frictional habits. It is also noted that the alveolar ridge keratosis, with a similar appearance to GL (Figure 3) is related to friction or mechanical irritation but may mimic tobacco–associated leukoplakia in smokers. 24
In our study population, smoking rates in both GL and n-GL are higher than those in the national data (2009 – male smokers 38.2% and female smokers 10.9%). 25 On the other hand, alcohol consumption rates are somewhat lower than those of the national data 26 : National data (in 2009) indicate alcohol consumption within guidelines among 68.7% men and 32.7% women (total: 49.8%) and alcohol drinking above guidelines by 8.6% men and 5.4% women (total: 7.4%). Lower drinking levels in this study population could be attributable to higher age groups recruited to the study. No differences in smoking rates were found in the GL group in comparison with n-GL group.
In this study, we hypothesized that gingival keratosis often diagnosed as GL was related to the oral environment such as dental prosthesis and some metabolic effects rather than traditional risk factors; smoking and alcohol misuse. However, there were no significant differences in the number of cases that were close to prosthetics as well as the presence or frequency of the lichenoid inflammatory cell infiltration between GL and non-GL.
Hypersensitivity to dental materials was the most suspected factor. However, there are only few reports related to OL with regards to amalgam or other metals restorations and resin filling or dentures, though numerous studies have been reported and elucidated an association with lichenoid contact lesions or atypical oral lichen planus. 27,28 Lichenoid reactions comprise clinical manifestations of contact hypersensitivity (type IV) of oral mucosa. 27 Skin patch test and blood tests such as lymphocyte stimulation test and memory lymphocyte immunostimulation assay test confirm delayed (type IV) hypersensitivity to metals. There is no gold standard for tests of specific allergens of dental materials other than patch tests which have limited use due to poor sensitivity and specificity. Nevertheless, patch testing is still the first line to identify any allergens to dental materials in clinical practice. Patch testing has recently been shown to be of benefit for the prediction of any mucosal lichenoid reactions. 29
The presence of more than one dental alloy in the oral cavity often causes galvanic currents and voltage affecting the oral mucosa. 30 Over 80 years ago, electrogalvanic currents generated in the oral cavity as a cause of OL was proposed by Ullmann. 31 Bánóczy et al. 32 examined 128 patients with OL and 326 patients with oral lichen planus for electrogalvanically induced oral white lesions and indicated that the term electrogalvanic white lesions is suggested as a common denominator for these mucosal changes, which seem to take the presentation of lichen planus more often than that of leukoplakia. Korraah et al. 33 investigated physiologic reactions of OL cells in vitro to electric fields and indicated that electric field strength of 1–10 V/m led to upregulation of cell proliferation rate from 10.6% to 44.1%. They concluded that oral galvanism induces subcellular changes in oral precancer cells in vitro. 33 Wartenberg et al. 34 investigated the mechanisms of apoptosis of oral mucosal cells in response to electromagnetic fields and suggested that apoptosis in oral mucosal cells is initiated by generation of reactive oxygen species in response to direct current and field treatment. Further studies are needed to prove the mechanisms of metal-induced oral keratotic lesions.
Candida test was positive in 30% in our study population, and it was lower in the GL group. In previous studies, Wu et al. 35 showed that 15.9% with OL were infected by candida by examining biopsy samples. Barrett et al. 36 suggested that there was a significant negative association of fungal infection with benign hyperkeratosis and the frequency of infection on tongue was significantly higher than that of others. Hongal et al. 37 analysed the prevalence of fungal hyphae in biopsies of patients with clinically diagnosed cases of premalignant lesions and conditions. They reported that the estimated prevalence of fungal hyphae in cases with or without dysplasia in leukoplakia was 41.4%, lichen planus 36% and submucous fibrosis 25%, and there was a significant association between degree of epithelial dysplasia with presence or absence of fungal hyphae in all the study groups. Abdulrahim et al. 38 reported that the buccal mucosa was the most prevalent lesional site in the histopathologically defined candida leukoplakia group (22/31; 71%), followed by the tongue (4/31; 12.9%), palate (3/31; 9.7%), gingivae (1/31; 3.2%) and alveolar ridge (1/31; 3.2%). Although GL mimics chronic hyperplastic candidosis, we could not confirm this to be a causative factor.
In our study, GL had a rather benign appearance microscopically. Cases that transformed in this group were among non-smokers and non-alcohol drinkers. Three of four cases were homogenous and had no epithelial dysplasia. In a previous hospital-based study from Japan, 39,40 gingival location was predominant in both localized and widespread multiple OLs. There was a high malignant transformation rate in widespread multiple lesions. The authors discussed whether their cohort may have included some cases of proliferative verrucous leukoplakia (PVL) or not, but argued otherwise. Considering verrucous appearance of GL and the benign pathology noted in microscopy, it is prudent to observe GL over long periods and to assess whether these cases would evolve to PVL. It is important to recognize that PVL often occurs on gingival locations, as noted by Fetting et al. 41 (100%) and Bagan et al. 42 (89%).
Frequency of dental treatment by restorations in Japan has been known to be higher, than undertaking prevention by dentists. 43 National health insurance in Japan covers the costs of medical and dental care; amounting to 70–100% depending on the health and social background. However, in case of dental restorations, choice of metals for dental restoration and crowns are limited and dentists are only allowed to use alloys; these consists of gold (12% or over)–silver–palladium metals, which are widely used in Japan. Furthermore, health insurance covers a little preventive care in general. Hence the frequencies of dental restorations among Japanese are likely to be higher under the Japan medical care system. The higher rate of dental restorations using metals among Japanese might be related to higher metal allergic reactions found in this study in both GL and n-GL groups. We could not, however, confirm any statistical association between GL and dental materials clinically or by patch testing. In this study, we were not able to specify the materials used in some prosthesis or crowns. Evaluation of the clinical relevance of patch test results has been always difficult for clinical dentists and requires an interdisciplinary approach in further studies.
Some of the limitations of this study were mainly related to the small sample size, despite this being a multicentre study. High prevalence of dental metal restorations in Japanese was found in both sub groups (GL and n-GL), which makes the case-control design inappropriate for such comparisons. Friction to gingivae compared to other sites was not inquired in detail in this study. The presence of prostheses may play an important role for hyperkeratinization of gingival tissues and our inquiry on this factor could have been broadened by inclusion of a metallurgist in our research.
In conclusion, leukoplakia affecting gingivae was more benign compared to n-GL histologically. There was no significant association with metal allergy in GL as revealed by patch testing. This study did not elucidate a particular risk factor for GL. Lower dysplasia scores were noted in GL compared to n-GL. Scully and Bagan 44 remarked that cancer cannot be excluded with confidence in potentially malignant disorders. Most GL so far seen are verrucous in appearance, and could have a higher risk, and this requires to be factored in our pathology investigations. Although seemingly benign, four of our cases (5%) transformed. Careful follow-up of GL is needed to determine whether these persons are at risk of developing PVL. Our results warrant further investigation of leukoplakia with a larger sample size in order to elucidate its natural history.
Footnotes
Acknowledgement
We thank Dr Tatematsu T and Dr Takahashi A for collecting the clinical data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Butterfield Award for UK–Japan collaboration in Medicine and Health to SW from of the Sasakawa Foundation of Great Britain (2010).