
Abstract
Background:
The first consultation with a health-care professional is crucial to make the correct diagnosis particularly with respect to narrating the symptoms encountered by the patient. Yet, currently, no information is available concerning the primary symptoms documented by patients with oral submucous fibrosis (OSF).
Materials and Methods:
A total of 158 OSF patients visiting outdoor patient departments (OSF-OPDs) and 104 pan shop customers (PSCs) were investigated. OSF-OPD cases and relevant PSCs cases were investigated to discover the chief complaints (CCs) leading to dental visits. Detailed demographic data, patient histories concerning relevant habits (with duration), and socioeconomic status were recorded. OSF cases were graded based on the degree of mouth opening.
Results:
Out of 158 OSF-OPD patients, only 43 (26.58%) reported relevant disease symptoms of OSF: in stage III, 28.57%, or stage IV, 38.09%. One hundred and sixteen patients (73.41%) reported CCs unrelated to OSF, and all of these cases were diagnosed with an early stage of OSF (stage I: 47.05% and stage II: 22.5%). Out of the total 104 PSCs, 66 PSCs have had prior dental consultations, but only five (4.80%) individuals had visited a health-care professional due to OSF-related CCs.
Conclusion:
A significant number of CCs made by OSF patients were unrelated to their disease signs and symptoms. There is a lack of awareness of OSF symptoms by pan chewers, thus hindering early detection.
Keywords
Introduction
Oral submucous fibrosis (OSF) is a chronic, progressive disease characterized by fibrosis of the connective tissue stroma. OSF is caused by areca nut/areca nut quid chewing habit, which is quite common in Asian countries. 1 In India, the prevalence of OSF ranges from 0.62% to 6.42%. 2,3 One recent study with a relatively large cohort of 99 cases of OSF reported a 3.72% malignant transformation rate of OSF, with an average duration of 37.42 months. 4 Moreover, OSF has been found to be associated with an impaired quality of life (QoL), along with a significant trend of increasing effects with advanced stages of the disease. 5 -7 Due to its high probability of malignant transformation, OSF is considered a disease with a significant mortality rate. Worldwide, oral cancer has one of the poorest prognoses and lowest survival rates and this remains unchanged despite recent therapeutic advances. Thus, early detection of oral squamous cell carcinoma (OSCC) associated with OSF by clinical examination is the key for better patient prognoses.
Reducing diagnostic delays to achieve early detection is a cornerstone to improving the QoL and survival of OSF patients by minimizing their risk of oral cancer progression. The early detection of OSF and OSCC arising from OSF requires a meticulous clinical examination, which is the ultimate key for a better prognosis. 8 Therefore, routine screening is encouraged and follow-up of OSF patients is of paramount value. However, a patient’s visit to a specialized/specialist health-care professional becomes the dependent parameter for the identification of the disease and subsequent follow-ups. Currently, however, no information is available in the scientific literature that details OSF patients’ symptoms. Moreover, we also speculated that there could be a significant number of OSF patients in the population who have never visited a dental hospital, irrespective of their knowledge about OSF and its consequences.
Objectives
To investigate the knowledge of presenting symptoms of OSF patients in the central region of India. To further complement the findings, surveys were conducted at pan shops to uncover the pattern of dental visits of PSCs.
Material and methods
The present study was carried out in a government tertiary care general hospital setting (Department of Dentistry, Indira Gandhi Government Medical College and Hospital, Nagpur, Maharashtra, India). The cross-sectional study enrolled a total of 158 clinically diagnosed OSF patients from the outpatient department from January 2017 to December 2018 by a convenience sampling method. All participants provided written informed consent. Ethics approval was obtained from the institutional ethics committee of the Government Dental College and Hospital, Nagpur, Maharashtra, India (ref no. GDCH/ethical/4506/10-08-2017).
Patients with OSF (OSF-outdoor patient department (OPD) patients) were identified during screening procedures and invited to participate in the study based on the following clinical criteria: intolerance to hot and spicy foods, pale oral mucosa, palpable fibrotic bands, and chronic, progressive trismus. 9 Detailed demographic data and a history of relevant habits, with duration information, were recorded. The socioeconomic status (SES) of each participant was determined by a modified Kuppuswamy’s SES scale. 10 This scale is based on a composite score that considers the education and occupation of the head of the family along with the monthly income of the family and yields a score between 3 and 29. This scale classifies the study populations into higher (I), middle (II, III), and lower SES (IV, V).
The chief complaint (CC) of each participant was carefully recorded and categorized into (a) those related to OSF and (b) those not related to OSF. The CCs like reduced mouth opening, burning sensation, and vesicle or ulcer formation (in the background of reduced mouth opening) were considered as OSF related CCs. After a thorough clinical examination, at the pan shop itself, the interincisal mouth opening of each patient was measured using a digital Vernier caliper and patients were graded into stage I to stage IV OSF as described by Lai et al. 11
The most likely place to find individuals with OSF in the general population are at local pan shops (establishments selling kharra/ghutka, mawa, pan masala, tobacco, etc.). Five known pan shop vendors from Nagpur (3) and Pune (2) district of India were selected for the current study. Individuals with OSF who visited these shops (PSC patients) were personally interviewed by AG, SG, and SS. They were asked about dental visits to any specialist health-care professional and the reason behind the visit. Additionally, data related to age, sex, occupation, education, household monthly income, relevant habits, and mouth opening measurements were also obtained. All mouth examinations and interviews were performed at the site of pan shop.
Statistical analysis
Data were analyzed using the Statistical Package for the Social Sciences, version 17.0 (SPSS Inc., Chicago, Illinois, USA). Chi-squared and t-tests were used, as appropriate, to calculate p-values. The level of statistical significance was p < 0.05.
Results
Demographic data (OSF-OPD patients)
The age of the participants ranged from 13 years to 54 years with a mean of 32.34 (±8.63) years. A male majority was observed with a male:female ratio of 3.78:1. Out of 158 patients, 85 (53.7%) patients with OSF had a habit of kharra (areca nut quid) chewing, 45 (28.48%) chewed areca nut and kharra, and 28 (17.72%) had a habit of chewing areca nuts only. The mean duration and frequency of these habits were 10.58 (±6.13) years and 8.39 (±3.48) times per day, respectively (Table 1). Kharra was kept in the oral cavity, mainly in the lower buccal vestibule, for 5–25 min while the areca nut was chewed for 3–15 min. The majority of OSF patients (32.27%) visiting an OPD had grade I disease followed by grade III (27.84%), grade II (21.51%), and grade IV (18.35%). A majority of OSF patients had a lower SES (90; 56.96%), followed by a middle SES (58; 36.70%) and a higher SES (10; 6.32%; Table 1).
Demographic details of OSF-OPD patients and pan shop customers.

OSF-OPD: oral submucous fibrosis patients from outdoor patient department; PSC: customers at pan shop having oral submucous fibrosis.
CC analysis of OSF-OPD patients
Interestingly, close to three-fourth (73.42%) of the OSF-OPD patients expressed CCs that were not related to OSF, and only 42 (26.58%) patients described OSF related CCs. A significantly higher number of OSF patients with grade IV disease (16; 38.09%) reported OSF-related CCs compared to others in the grade I disease group (7; 16.66%) (p < 0.001; Table 2).
Oral submucous fibrosis related and not-related chief complaints in OSF-OPD patients.

OSF-OPD: oral submucous fibrosis patients from an outdoor patient department.
Among 158 OSF patients, the most commonly reported CC was a sudden difficulty in opening the mouth due to pain in the third molar region (pericoronitis) (48; 30.37%), followed by a reduction in the mouth opening (25; 15.82%), whereas pain in the pre-auricular region (4; 2.53%) and nonhealing oral ulcers (4; 2.53%) were the least common CCs. Among OSF-related CCs, a progressive reduction in mouth opening (25; 59.52%) was the most common, followed by burning sensations (10; 23.80%) and frequent ulcerations (7; 16.66%). Among, non-OSF-related CCs, pain in the third molar region (pericoronitis) (48; 41.37%) was the most common, followed by toothache (24; 20.68%) and tooth stains (14; 12.06%). There were a few other non-OSF-related CCs including mobility of teeth (7; 6.03%), redness of gums (5; 4.31%), tooth sensitivity (5; 4.31%), traumatic ulcers (5; 4.31%), pain in the pre-auricular area (TMJ pain) (4; 3.44%), and non-healing oral ulcers (4; 3.44%; Table 3).
Details of chief complaint and stages of OSF in OSF-OPD.

OSF-OPD: oral submucous fibrosis patients from outdoor patient department.
In relation to SES, a significantly higher number of OSF patients with an upper SES reported OSF related CCs (8; 80.00%). In contrast, participants with middle and lower SESs reported non-OSF-related CCs ((51; 87.93%) and (63; 70.00%); Table 4).
Oral submucous fibrosis related and not related chief complaints and socioeconomic status in OSF-OPD.

OSF-OPD: oral submucous fibrosis patients from outdoor patient department.
Analysis of CCs made by PSC patients
All of the 104 individuals at pan shops who were included in the study were males. Due to social norms, women do not visit pan shops in most parts of India. The PSC patients’ ages ranged from 16 years to 70 years, with a mean of 36.67 (±11.49) years. A majority of the individuals had stage III disease (46; 44.23%) OSF, followed by stage II (32; 30.76%), stage IV (19; 18.26%), and stage I (7; 6.73%). Out of 104 individuals, 38 (36.53%) had not visited a dental health-care professional in their lifetime (Table 1). Among 66 individuals with a prior dental consultation, 61 (92.42%) had made visits for non-OSF-related CCs, including stains on teeth (49.18%), toothache (40.98%), pain in third molar region(4.91%), and other CCs (4.91%).Only five (7.58%) individuals had OSF-related CCs (Table 5).
Details of chief complaint and stages of OSF in pan shop customers.
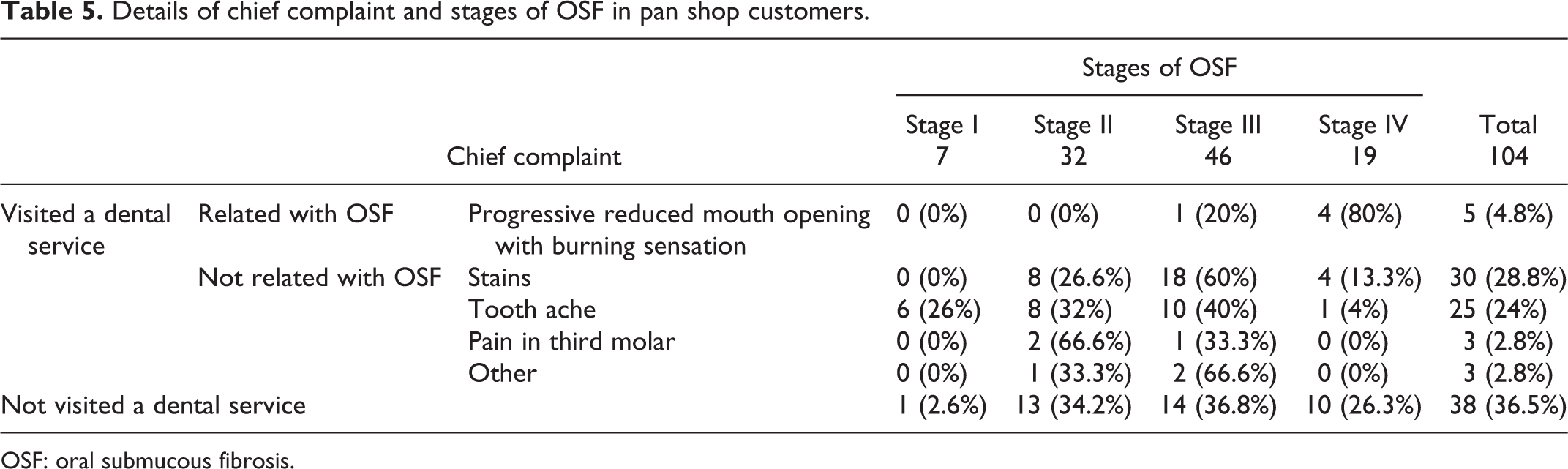
OSF: oral submucous fibrosis.
Discussion
OSF is characterized by symptoms such as burning sensations, trismus, ulceration, and xerostomia, and it causes a significant impairment in an individual’s QoL. 12 Hence, it is imperative that these patients visit dental facility when disease problems occur. Surprisingly, only about one-fourth (26.58%) of the patients had visited for OSF-related problems per se, while the majority had visited due to symptoms that were unrelated to OSF.
To further complement the results obtained from the CC analysis of OSF-OPD patients, we investigated the dental visit patterns of pan shop customers (PSCs) with OSF disease. Remarkably, only 5 (4.80%) PSCs had earlier consulted a dental health-care professional for OSF-related symptoms. These results strongly suggest that there could be a larger population with OSF in the community who may have never visited dental hospitals/health-care professionals for any OSF-related or non-OSF-related symptoms of dental origin and thus have not been considered. This may be attributable to a lack of awareness about the disease and limited knowledge about its serious potential for malignant transformation. Unfortunately, there are no committed Indian studies on OSF awareness and knowledge. Hence, there is a dire need for such studies to explore the seriousness of the situation so appropriate measures can be initiated. If this situation is not addressed, then it raises serious concerns about OSCC early detection strategies, as OSCC has a better prognosis at early stages.
The most commonly reported CC in OSF patients was sudden difficulty in opening the mouth due to the impaction of the third mandibular molar and associated pericoronitis (48; 30.37%). Interestingly, this was also the most common complaint among non-OSF-related CCs (41.37%). In these patients, OSF was noticed incidentally and comprised clinical features including blanched buccal mucosa, atrophic uvula, and a history of burning sensations and a progressively reduced mouth opening. We believe that OSF aggravates pericoronitis in patients with impacted mandibular third molars. Individuals with pericoronitis have difficulty performing oral hygiene maintenance due to a limited ability to open the mouth. The sudden limited mouth opening in pericoronitis results from the involvement of the submasseteric space causing a reflex muscle spasm. As OSF is characterized by a progressively reduced mouth opening, it exacerbates difficulties in opening the mouth and further oral hygiene maintenance in patients with pericoronitis becomes difficult. Furthermore, the pericoronal flap around the last mandibular molar may be more firm and resilient in patients with OSF, thus preventing adequate cleaning. As pericoronitis involves pain that is acute and severe in intensity (unlike OSF, which is often associated with tolerable symptoms), many patients in the present study reported pericoronitis associated with third mandibular molar impaction (40.66%). Thus, it is noteworthy to consider that OSF patients with pericoronitis experience aggravated symptoms of both conditions resulting in functional limitations, including limitations to tooth brushing and chewing, which further deteriorates both the oral and general health of the patients. Therefore, management of impacted last mandibular molars and associated pericoronitis in OSF patients may improve their QoL.
Due to a lack of dental and oral health awareness in the Indian population, regular checkups at dental clinics or hospitals are uncommon. Unless and until there is significant impairment of functional capability, individuals do not visit dentists. The most common reason for impairment of functional capability is severe pain associated with dental caries and pulpitis. Accordingly, 20.68% of the participants in this study visited dental hospitals with a CC of toothache due to dental caries, with or without periapical infection.
In the present study, 14 patients (12.06%) made dental visits for the removal of tobacco stains on the teeth. Most of these patients were in the second and third decades of their lives. Generally, individuals in these age groups are more conscious aware of their social lives and appearance. These findings suggest that even family members of the patients were unaware of the potentially malignant nature of OSF.
It has been reported that periodontal disease may be an independent, causal risk factor for OSCC. 13 Therefore, chronic periodontitis may be a clinical, high-risk factor in OSF for malignant transformations. 14 Oral ulcers resulting from chronic trauma caused by buccally placed third molars and sharp edges of attrited posterior teeth may be an additional cause for malignant transformations in OSF. 15 In the present study, OSF patients reported CCs including mobility of teeth (periodontitis) (6.03%), redness of gingiva (4.31%), sensitivity (due to attrition) (4.31%), and traumatic ulcers (4.31%). Thus, the management and prevention of the abovementioned conditions in OSF patients is necessary to reduce the risk of malignant transformation. Four patients reported a CC of chronic nonhealing ulcers (with the potential for malignant change), two of whom had grade III and the other two of whom had grade IV OSF. Of the four patients, three consented to incisional biopsy. Two cases were histopathologically well-differentiated squamous cell carcinomas, and one was a case of severe epithelial dysplasia. The findings of the present study support the evidence of an increasing trend of OSF-associated OSCC, as well as the increasing malignant potential of OSF. 15
Four stage I OSF (3.44%) patients reported a CC of pain in the pre-auricular region (TMJ). This pain could be due to severe tooth attrition, which leads to reduced vertical occlusal height, forward movement of the mandible and pulling of the TMJ ligaments. However, there is nothing in the literature suggesting a correlation between OSF and TMJ pain or myofacial pain dysfunction syndrome.
In this study, OSF was diagnosed as an incidental finding in 73.41% of patients with non-OSF-related CCs. A noteworthy finding is that approximately two-thirds of the patients (69.55%) had early-stage OSF (stage I (47.05%) and stage II (22.5%)). Among 42 (26.58%) patients who reported disease symptoms, two-thirds of the OSF patients had moderately advanced and advanced stages of the disease (stage III (20.58%) and stage (IV 4.41%)). Reports in the literature have suggested that the degree of mouth opening has no correlation with epithelial dysplasia or the malignant transformation of OSF (even early-stage OSF can transform into OSCC). 16 In the current study, while two-thirds of the patients were identified to have stage I and stage II OSF, these have the potential to develop into OSCC. Hence, we believe that early detection strategies must be applied during the early stages to reduce the burden of oral cancer and further complications.
In the current study, a large number of OSF patients had a low SES (56.96%) or middle SES (36.70%). Only 6.32% had an affluent background. These findings are in accordance with a recent study that suggested a higher prevalence of OSF, especially in the advanced stages, in patients with a low SES. 17 The higher prevalence of OSF in lower SES groups may be attributed to the lower purchasing power of these patients, even though therapeutic options are available. 18 Lower educational levels and employment type may also be important factors in the causation and progression of OSF. As education level determines occupation, lower SES individuals usually have lower educational achievements in combination with nonprofessional occupations. In the central part of India (where the study population resides), the majority of lower SES individuals frequently consume kharra/gutkha and other products containing areca nuts during their working hours. Moreover, these individuals have a limited knowledge and awareness of OSF and its complications.
In this study, a significantly higher number of OSF patients with middle (70%) and low SESs (87.93%) had non-OSF-related CCs in contrast to those with an upper SES (20%). These results support our previous investigation, which demonstrated a strong association between lack of awareness of OSF and SES. 17
Conclusion
The main strength of the current study is a realistic presentation of the patterns of dental visits made by OSF patients, which can directly or indirectly affect the early detection and prevention of OSCC associated with OSF. These findings are highly suggestive that many patients’ visits pertaining to OSF are incidental in nature (at least in the early stages), which emphasizes serious negligence by the population. However, conclusions drawn from the present hospital-based study cannot be generalized, as routine dental checkups and oral health awareness varies from country to country and from one region to another. Future multicentric studies covering different regions would provide a better understanding of this situation in India and worldwide. There is a dire need to generate large-scale public awareness campaigns and introduce basic knowledge about OSF and its inherent malignancy risks through posters, awareness campaigns at schools (particularly important in economically developing countries where patients are frequently seen at pediatric ages) and at the corporate organization level, and awareness marathons and advertisements in social media and television for the general public. 7 There should also be publicity regarding the carcinogenic potential of areca nuts, similar to the publicity given to tobacco products. The rural population is the most vulnerable group and has a higher risk of areca nut addiction than the urban population. There is also a need for thorough clinical examinations of every patient, despite their CCs, and it is essential to maintain follow-up records at all hospitals. Above all, banning areca nuts through strict government policy may be the most beneficial action that could be undertaken.
Footnotes
Acknowledgments
We thank all pan shop owners and managers for giving us permission to carry out interviews at their pan shops. We highly appreciate the wholehearted and committed support extended by them during the study period.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.