
Abstract
Areca nut and products made from the nut, evaluated by the International Agency for Research on Cancer as carcinogenic to humans since 2004, are being increasingly used in India and South East Asia and exported to many countries. There is thus an urgent need to identify best control policies and research gaps. On 1 February 2018, a group of experts shared their latest knowledge and perspectives on areca nut at Healis-Seksaria Institute for Public Health in Navi Mumbai, Maharashtra, India. By itself, areca nut has been implicated in oral and oesophageal cancer. Areca nut users are also at high risk of oral submucous fibrosis, a debilitating and potentially malignant condition. Users may also suffer adverse health outcomes due to smokeless tobacco, commonly mixed with areca nut. The use of areca nut commonly begins in childhood and often proceeds to use with tobacco. Gutka, a widely consumed, industrially made areca nut product containing tobacco, has been banned in all states and union territories of India, but it is still widely available. Areca nuts contain arecoline, an alkaloid that stimulates various brain receptors, promoting physical dependence. Areca nut alkaloids have also been implicated in carcinogenesis. Other chemicals, introduced during cultivation and processing of areca nuts, contribute to oral submucous fibrosis and cancer. The wide variety of products, different storage conditions and lack of regulation can lead to significant variation in the content of toxicants, carcinogens and alkaloids, making the psychological and physical dependence issues even more challenging. Regulation of product contents is needed as a part of control measures to supplement product bans.
Introduction
Areca nut, used by an estimated 600 million people globally, is the fourth most commonly abused addictive substance after nicotine, ethanol and caffeine. 1 Areca nuts (also called betel nuts in the literature and ‘supari’ in some local languages in India) are drupes from the palm tree Areca catechu, which grows naturally in South and South-East Asia and the Pacific Islands (Figure 1). The nuts and consumer products containing areca nut are not only increasingly being used by people in India and other countries in South and South East Asia, as well as in China and the Pacific, but are exported as well. Elsewhere, such as in the Gulf states, Europe and North America, areca nuts are used mainly by immigrants from Asian and Pacific countries. 2 The United States is one of the major destinations for these products, where they are available in Asian grocery stores.

The areca catechu palm, laden with drupe fruits.
There is an urgent need to identify the priority research gaps and potential best policy and regulatory measures in view of increased availability and consumption of areca nut products around the world and their associated health risks.
Taking inspiration from an earlier large, extensive meeting held in London, in November 2000, on the topic of areca nut, 1 a small meeting of experts on areca nut was convened in Navi Mumbai, Maharashtra, India, by Healis Sekhsaria Institute for Public Health on 1 February 2018 to share their latest knowledge and perspectives on areca nut. This article summarizes the key information presented at that symposium.
Types of products
In India, dehusked areca nut is used by itself in raw or processed form (boiled, roasted, fermented and sweetened) and generally with tobacco. It is more often used as an ingredient in different products: in betel quid (pan), in mawa; or, in industrially manufactured items such as gutka and pan masala. 2 Sweet/scented supari contains areca nut, sugar and/or artificial sweeteners, often spices (e.g. cardamom, anise seed), other flavourings (such as mint), concentrated fragrances and often colouring substances. Betel quid is a mixture of areca nut pieces, catechu, spices, other condiments and often tobacco, all rolled up in fresh green ‘betel leaf’ of the vine Piper betle that is smeared with slaked lime. Mawa is a mixture of areca nut pieces, tobacco and slaked lime. Gutka and pan masala contain essentially these same ingredients as sweet/scented supari, plus the other usual ingredients of betel quid: slaked lime, catechu, tobacco (in gutka and some varieties of pan masala) and magnesium carbonate to prevent caking and to mask the dark colours of tobacco and catechu. In gutka and pan masala, the only major ingredient of betel quid which is missing is fresh betel leaves, although pieces of dehydrated betel leaves may be added in a few products. Gutka and pan masala, which are advertised as mouth fresheners, are currently the major forms of areca nut consumption in India. 3 Outside India, often whole (unhusked) fresh green nuts are used along with slaked lime and in betel quid as in many Pacific island countries, Southern China and Taiwan. In Taiwan, apart from betel leaf, alternatively betel inflorescence or stems may be used with the unripe areca nuts. In Hunan Province of China, dried unripe areca nuts are used. 4
Extent of areca nut use in India
Information on betel quid or areca nut use has generally been subsumed under the category of smokeless tobacco. According to the second round of the Global Adult Tobacco Survey in India or GATS 2 (2016–2017), 3 smokeless tobacco use among adults is 21.4%, down from 25.9% in GATS 1 (2009–2010). 5 The most common smokeless tobacco products or mixtures used by men are khaini (chewing tobacco containing slaked lime) and gutka. The products used the most by women are khaini and betel quid with tobacco. Clearly, areca nut is most commonly used with smokeless tobacco in India. Several months after this symposium, the complete report of the Global Adult Tobacco Use Survey for India came out and state-wise prevalence of separate products and mixtures became available. The countrywide prevalence and the minimum and maximum prevalence among states are shared in Table 1. For example, the prevalence of chewing betel quid with tobacco averages at 5.8% and varies from zero to 39.5% in the different states. For the first time in a national survey, prevalence of areca nut practices without tobacco was provided, also shown. 3 As yet, however, the prevalence of total overall areca nut use with and without tobacco has not been reported.
National prevalence of use of areca nut products or mixtures in India and lowest and highest prevalence among states.
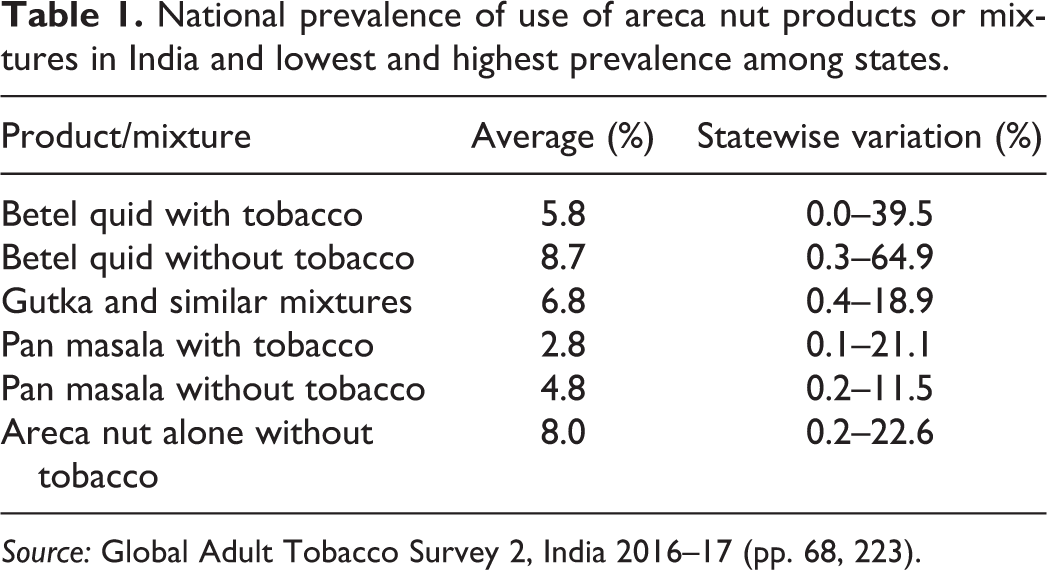
Source: Global Adult Tobacco Survey 2, India 2016–17 (pp. 68, 223).
Disease risks associated with areca nut use
It is well established that areca nut used in any form causes oral cancer in humans. 4,6 Many studies have also found betel quid, with or without tobacco, linked to cancers of the pharynx and its subsites. Chewing of betel quid, both with and without tobacco, is also clearly implicated in oesophageal cancer. In studies from Taiwan, links between betel quid without tobacco and liver cancer have also been found; however, confounding with other factors could not be ruled out. 4
Areca nut also has a variety of other health consequences: altered blood sugar, heart rate and blood pressure, and it may worsen asthma. 4 As areca nut is frequently used with smokeless tobacco, adverse health effects are commonly reported for combined use. Smokeless tobacco use plays an important role in causing death from heart disease, 7,8 lung disease and tuberculosis 7 as well as oral cancer. 4 If used by pregnant women, smokeless tobacco causes low birth weight, reduced gestational period, increased still births 9 and anaemia. 10 The use of gutka, as it contains tobacco, is also a strong risk factor for these diseases. There are indications that areca nut, even when used without tobacco, would cause similar health effects. Currently, an epidemic of mouth cancer among young persons is growing at an explosive rate in India, almost entirely due to use of gutka and pan masala with tobacco. The rises in oral cancer incidence were apparent in 2010 and are, anecdotally, continuing. 11 Hence, the widespread availability of areca nut-based products is currently a serious public health issue. Oral cancer incidence is very high and increasing in several Asian countries, including India, Pakistan and Taiwan, places where areca nut use has been increasing in recent years. 12
Oral manifestations of areca nut and carcinogenicity
Areca nut is implicated in a variety of oral disease processes. There is a strong link between areca nut use and the development of oral submucous fibrosis, which is the severe scarring of the inner cheek and soft palate, in which fibrous bands form directly under the mucosal surface. 13 In severe cases, this extends throughout the oral cavity, the hypo-pharynx and the oesophagus. This scarring worsens over time, such that areca nut users begin to suffer great pain and are progressively unable to open their mouths. 14,15 Oral submucous fibrosis is a highly debilitating disease with no known cure and requires surgical excision to address symptoms. Postsurgical recurrence is common, particularly if areca use continues, exacerbated by scarring as part of wound healing. In addition, areca nut users are at a very high risk for developing mouth cancer. 15,16 Users at risk include those who use areca nut without tobacco, as shown in a study from Pakistan. 17 In Taiwan, betel quid chewers do not add tobacco and some still develop oral cancer; however, most chewers also smoke cigarettes. 18 The more often areca nut is used, and the longer the duration, the higher the risk of mouth cancer. The less educated are the most likely to present with late stage cancer, which has a high mortality. Those using areca nut products daily have an extremely high risk of mouth cancer in their lifetime. In a case–control study with 134 cases of oral cancer and 268 controls, adjusted odds ratios for getting oral cancer were 5.1 for gutka consumption, 11.4 for supari, 6.4 for betel quid and 6.0 for chewing tobacco, all with significance at the level of p < 0.0001. 19
Use of areca nut products by children
Children usually begin chewing habits with areca nut products, especially sweetened and flavoured areca nut (supari), but many move on to using tobacco. Thus, areca nut acts as a gateway product for tobacco. 20 Areca nut users among school children are eight times more likely to be tobacco users than are nonusers of areca nut. 21
A study conducted in 2014 among 1053 students in the eighth and ninth grades (mean age 14.2 years ± 1.2 years) in 16 municipal schools in Mumbai found 18% of students reporting ever use of areca nut, 22 although a later study in 2016 among students in grades seventh through ninth (mean age 13.4 ± 1.3 years) in 12 schools reported 32% ever use of areca nut. 21 This shows that areca nut use is also a paediatric problem. Over 40% of school students are unaware of the harmful effects of areca nut. 22 Areca nut products are available in India at low prices, have product packaging designs similar to those of smokeless tobacco and are positioned at stores and kiosks frequented by children. 23
Effective areca nut interventions
Cessation of tobacco and areca nut use among 13–15-year-old school children using areca nut and/or tobacco in Mumbai is being attempted in a programme called LifeFirst. 24 The LifeFirst programme consists of sensitization of the principals and teachers to the need for such a programme, orientation for all the students of seventh, eighth and ninth standards (age 12–15 years) by providing awareness of the harmfulness of areca nut and tobacco and giving users a chance to voluntarily register for the service designed to help them quit. This service includes theme-based interactive group counselling sessions and individual sessions according to the need and are conducted during school hours. During the course of the session, students acquire refusal skills, coping mechanisms and develop confidence to say ‘no’ to peers. The students are counselled in a child friendly way with the help of games, activities, role plays and audiovisual aids. Periodic monitoring and follow-up help to ensure the success of this programme.
Of the 3158 students aged 13–15 years who enrolled in the LifeFirst cessation programme and were interviewed during 2012–2017, 84% were exclusive areca nut users (no tobacco use). Among these, 62% quit using areca nut at the end of the programme. A lower success rate was achieved among students who used areca nut in various combinations with tobacco, as a smokeless or smoked product (13% of students enrolled in the programme also used tobacco: among these, 42% stopped their usage at the end of the programme). Lastly, 2% and 1% were exclusive smokeless or smoked tobacco users respectively: among them 51% and 44% students, respectively, stopped using tobacco at the end of the programme. These results suggest that the addictive practices are more difficult to quit if areca nut and tobacco are being used simultaneously. Nevertheless, a total of 1845 students (58%) reported stopping their areca nut and/or tobacco habit at the end of this programme, indicating that such interventions can be effective in reducing the prevalence of use associated with these products, and corroborating earlier observations that such interventions can be effective.
Earlier, a 10-year prospective intervention study in a defined cohort of 12,212 tobacco users, selected in a baseline survey conducted in 1977–1978 from a population of about 48,000, aged 15 years and above, in 23 villages in Ernakulam District in Kerala, consisted of a strong health education component on tobacco and areca nut chewing. In this population, chewing of betel quid with tobacco was highly prevalent and 6341 of the cohort chewed betel quid (3809 in the controls). Each year, each individual was exposed to personal communication on the need and way to stop their tobacco use by social scientists and dentists at the time of an annual interview and oral examination. They were also exposed to mass media communication in the form of films, radio spots, newspaper articles, posters and cinema slides on the issue. After 5 years of intervention, 13% of the intervention group stopped or reduced their chewing habit compared to 4% in the control group. After the 10-year intervention,11 new cases of oral submucous fibrosis were seen among 6341 chewers giving annual incidence rate per 100,000 as 8.0 among men and 29.0 among women. In the control cohort, the annual incidence rate of oral submucous fibrosis (OSF) per 100,000 among 3809 chewers, based on 11 new cases, was 21.3 among men and 45.7 among women. However, the differences were not statistically significant due to the low number of cases. 25 It is notable that during that period, only betel quid was chewed in these populations, not gutka or pan masala.
Dependence and psychotropic effects
The most obvious indication of areca nut use, apparent to both the user and the observer, is the production of copious amounts of saliva, brownish-red in colour due to pigments in the nut. The user is often compelled to leave enduring evidence of the habit in the form of brownish-red stains on the ground or walls from their expectorations. The stimulation of saliva is due to the presence of an alkaloid, arecoline, which mimics acetylcholine, the ‘rest and digest’ hormone of the autonomic nervous system. 26 In 2015, it was discovered that arecoline is also a weak activator of the same brain receptors that cause nicotine addiction. It is, therefore, likely that the nicotinic receptor activity of arecoline primes users for the addicting effects of nicotine, encouraging the addition of tobacco to areca nut. 27 While this leads to dependence, areca nut by itself also affects various other brain receptors including those targeted by narcotic drugs. 28 Areca nut users variously report that they perceive it as being a stimulant, like coffee, or a sedative, like alcohol. These effects appear to be associated with unidentified compounds in areca nut. Nonetheless, as physical dependence, which leads to withdrawal symptoms, comes from the nicotine-like activity of arecoline, treatment for areca nut addiction may draw on work from the field of nicotine addiction and use replacement therapies such as nicotine gum or possibly an approach that would incorporate the use of safe arecoline replacement products.
Harmful chemicals in areca nut products
Addictive, toxic and cancer-causing chemicals present in areca nut-containing products are believed to be responsible for the devastating health outcomes associated with their use. Some of these chemicals are naturally present in areca nut; for instance, areca-specific alkaloids are arecoline, guvacine, arecaidine and guvacoline have been implicated in both the addictiveness and carcinogenicity of areca nut. 6,29,30 Some areca nut polyphenols (e.g. flavonols and tannins) also play a causative role in the oral submucous fibrosis disease process. 6 Copper, in the form of sulphate, an ingredient of Bordeaux mixture, commonly sprayed on the areca nut crop to prevent fungal infection, increases the copper content of the nuts. 31 Copper has been implicated in the formation of collagen bands in the oral mucosa of chewers. 32,33 Other harmful chemicals may be introduced when areca nut is processed or when products like betel quid, gutka or pan masala are made; examples of such substances include polycyclic aromatic hydrocarbons, which can be formed when areca nut is roasted, calcium hydroxide (aka slaked lime) that is added to increase the alkalinity of the product, nicotine that is contained in tobacco, and potentially other toxic chemicals that may be added with flavouring and colouring ingredients. In addition, certain harmful chemicals can be produced while the product is chewed. For instance, areca alkaloids can react with nitrite present in saliva (which is formed through the conversion of dietary nitrate) to form areca-derived nitrosamines N-nitrosoguvacoline, N-nitrosoguvacine and 3-methylnitrosamino-propionitrile, which have the potential to damage DNA. 34 -36 If the product also contains tobacco, then a similar process can lead to the formation of tobacco-specific N-nitrosamines in the mouth that are known to be highly carcinogenic, adding to harmful exposures, DNA damage and cancer risk in users. 37 -39 The highly alkaline pH of many products, due to the addition of calcium hydroxide, is an additional risk factor as it contributes to tissue damage and inflammation. Because of the wide variety of areca nut products and the lack of proper regulation of their content, the levels of all these important toxicants and carcinogens vary significantly across different products. 40 Storage conditions can also have an impact on the levels of many such chemicals. Therefore, even the same product purchased from different vendors can provide different levels of toxic exposure. Thus, some users may be exposed to quite high levels of harmful chemicals. Control measures aimed at areca nut products should include regulation of product contents and education of consumers and health professionals.
Agricultural and economic policies in India
The areca nut has been the focus of policy intervention in India since 1947, when major areca nut producing areas were partitioned away from India. By 1965, India again became self-sufficient in areca nut production. 41 Subsequent overproduction, leading to low prices, was overcome by the appearance on the market in 1973 of a value-added product, pan masala. This was sold in two versions: one with and one without tobacco. Since 1985, manufactured areca nut products began to be sold in individual portion packages, which greatly increased sales. The number of manufacturers has swelled into hundreds making pan masala, gutka and sweet-scented supari and vendor-made areca nut mixtures, containing tobacco (mawa, kharra), became a lucrative business. This has further stimulated areca nut production and rewarded farmers. The manufactured products are subject to excise taxes, which, however, are in large measure, evaded. Using available data, during 1961 through 2016 in India, area under areca nut cultivation nearly tripled, while its production increased five times. 42 From 1995, with increasing demand, the industry began to import low-cost areca nut, leading to reduced domestic prices. In 2002, in response to complaints from farmers incurring losses, the Government of Karnataka included areca nut under the Market Intervention Scheme of the Central Government, which includes application of a Minimum Support Price. However, there is a short window of time for sale of areca nut under the scheme, and many farmers were unable to realize such prices due to various market inefficiencies. 43 Two economic studies in 2011 reported that areca nut cultivation had become unremunerative due to low market prices. 43 Since 2012, government regulated minimum import prices (introduced in 2008) have increased over 333% from INR 75 to INR 251 per kg. According to the multistate cooperative for procurement and marketing of areca nut and other horticultural products, Campco, Ltd, about 20% of the areca nut produced is consumed as ripe nuts. This statement seems to infer that the remaining nearly 80% of the crop consists of unripe nuts that get processed into to red boiled type, which typically go into the gutka and pan masala industry. 44 Although gutka and pan masala containing tobacco began to be banned in different states and union territories from mid-2012 onwards and are currently banned in all states, yet manufacturers have continued to make and sell such products locally in the guise of exports, typically evading taxes. Exported areca nut products have been reaching 59 countries. 45 As a strategy to evade the ban on gutka, areca nut and tobacco are now being mixed by retail vendors and small manufacturers in the informal sector. Agricultural production of areca nut has continued to increase, yet a few farmers have replaced their areca nut plantations with other crops with the help of government subsidies 46 as is also slowly happening in Taiwan. 47 Entrepreneurs are trying to make new areca nut-based, tobacco free products such as drinks and mouth fresheners, keeping them outside of the bans. In this situation, the manufacturers and vendors/retailers gain at the expense of the consumers, who get addicted to these products, damage their health and may even lose their lives.
Health policies and regulatory framework needed
Proper implementation of existing laws prohibiting the sale of tobacco products to minors and in the vicinity of schools would help to prevent the products containing areca nut or areca nut and tobacco from being used by children. 48 School-based tobacco control programmes should address areca nut use to effectively prevent its harmful effects and also prevent the initiation of tobacco products – something that should not be left entirely to non-government agencies.
Early health policies in India specifically on areca nut (without tobacco) have aimed to make manufacturers warn potential consumers on the package (under the Prevention of Food Adulteration Act, 1954) of the dangers of consuming areca nut products through simple text warnings in small font, generally in English. Despite these warnings, consumption of areca nut products has reached high levels and more recent policies have banned the manufacture and sale of products containing areca nut with tobacco or nicotine (Food Safety and Standards (Prohibition and Restrictions on Sales) Regulation, 2011, No. 2.3.4), 49 and food products containing magnesium carbonate in excess of the legal level (Food Safety and Standards (Food Products Standards & Food Additives) Regulations 2011, No. 3.1.7). 50 Wherever laws have been enforced effectively, studies have shown that these policies have helped some users quit and to a limited extent, prevented children from accessing the products. However, unfortunately, these policies have not been uniformly enforced in all states, enforcement being a local state issue. In many areas, vendors have been legally selling the areca nut products separately from the tobacco products. In some states (Maharashtra, Bihar and Himachal Pradesh), areca nut products have also been banned as unsafe food products under provisions of the original Food Safety and Standards Act, 2006. 51 However, these bans have not been enforced effectively. Hence, some other strong control measures are required for areca nut, just as for tobacco. 21 Although the Cigarettes and Other Tobacco Products Act, 2003 (COTPA) 48 regulates tobacco products, which include areca nut products containing tobacco, there is no regulatory framework on areca nut products as such. For example, legislation is needed to get more effective warnings, including graphical, on areca nut-only products. For this to happen, policymakers need to be sensitized to the issues. As most states appear reluctant to enforce notified bans of areca nut products containing tobacco or to ban areca nut-only products, areca nut requires a regulatory framework, similar to that for tobacco. A whole of government policy solution prioritizing public health in relation to areca nut is an urgent need. It is hoped that in the not too distant future, an international policy framework will come into being, along the lines of that for tobacco. 52
Conclusions
The international community needs to be aware of the widespread increasing use of areca nut and the related issues and developments, as the health of current and potential consumers is at stake, including that of children and women of reproductive ages. Users of areca nut tend to eventually add tobacco. It would be useful to have the overall prevalence of any areca nut use and as the prevalence of areca nut with and without tobacco for monitoring purposes. To protect the public from the harms of areca nut, legislation is required to regulate and control the use of areca nut products within countries.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflict of interest with respect to the research work described, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
{kind=link}