
Abstract
Patients in the intensive care unit (ICU) are often on potent medications. According to Norwegian medication administration regulations, all intravenous medications should be subject to double-checking before patient administration. The aim of this study was to explore Norwegian ICU nurses’ perceptions of how medication double-checking is practiced in the ICU. We chose a qualitative and explorative design, used the COREQ reporting guideline and performed two focus group interviews in two ICUs. This study found that barriers to performing double-checking included understaffing, physical unit design and a lack of written medication orders. In clinical practice, informal guidelines exist as to which medications should always be double-checked and which medications can be administered without a prior double-check. The informants felt reluctant to administer medications without prior double-checking. The graded approach to medication double-checking practiced in our two ICUs is not in agreement with Norwegian regulations but is more in line with international recommendations.
Introduction
In 2020, more than 17,000 patients were admitted to Norwegian intensive care units (ICUs). 1 The most common reasons for admission were a need for mechanical ventilation or for infusion of vasoactive medications. 1 Intensive care patients on mechanical ventilation and/or advanced supportive treatment often require potent medications including analgesia, sedation and/or vasoactive infusions. 2 Despite mandatory use of adverse event reporting systems, there is a lack of knowledge about the extent of medication errors in Norwegian ICUs. 3 However, a large multinational study identified 74.5 errors in the administration of parenteral medications per 100 ICU patient days. 4 Errors in the administration of potent medications may have fatal consequences for the already vulnerable ICU patient population. Thus, ensuring safe medication administration practices is an important part of ICU nurses’ responsibility, and the intensive care nurse must be familiar with existing regulations and guidelines. In the Norwegian regulations for medication administration §3, medication double-checking is defined as two persons independently (manually or electronically) confirming by signature that a task has been performed correctly and according to procedure. 5 In clinical practice, double-checking is performed during the preparation stage of the medication administration process. The nurse conducting the double-check performs an independent control of the dilution and admixing of the medication, the dosage, administration route and infusion rate and compares it to the doctor's order.6,7 The medication administration regulations state that medication double-checking should be performed in the most error-prone situations and in situations in which double-checking may reduce the risk of error, but leaves it up to individual hospitals to define the specific circumstances for which double-checking is required. 8 The medication administration regulations recommend that double-checking should be performed when preparing medications for injection or infusion, for narcotics and when diluting or admixing medications. 8 The largest Norwegian university hospitals have taken on board these recommendations and made them mandatory.6,7
Still, in Norwegian health care, double-checking is performed to an insufficient extent. 9 In a Norwegian survey, only half of respondents reported that they always performed double-checking according to the guidelines. 9 Reasons for not following the guidelines included difficulties in getting hold of a second nurse (82%), that double-checking is time consuming (20%), a lack of unit support (10%) and that they trust their colleagues (5%). 9 The survey did not investigate how double-checking is practiced in Norwegian ICUs.
Two large systematic reviews concluded that there is no evidence to support the idea that double-checking reduces medication errors.10,11 Other studies indicate that double-checking may be an effective measure to limit the risk of error in selected situations.12–15 However, the beneficial effect is reduced when the nurse who is double-checking is in a hurry or if he/she performs double-checking frequently enough to be on ‘autopilot’, meaning that the nurse is not doing a thorough assessment but only throws a superficial glance. 16 Performing double-checking is a resource-intensive task and often results in a colleague having to interrupt or pause the task that he/she is doing.
ICUs differ from other parts of the health care system, as the nurse-to-patient ratio is usually at least 1:1, and there is frequent administration of medications that require double-checking. 5 There is a lack of research on how the unique ICU context influences the way double-checking is being practiced. Furthermore, the frequent administration of potent medications requiring double-checking may result in recurring interruptions in the ICU workflow.10,11 It is unclear how intensive care nurses are affected in their work by these frequent interruptions or how they prioritise double-checking against other necessary and important tasks. 11 Thus, the aim of this study was to explore intensive care nurses’ experiences and perceptions of medication double-checking. The research question was: What experiences do intensive care nurses have of practicing medication double-checking in the ICU?
Method
The study used a qualitative, explorative design with focus group interviews as the data collection method, and data were analysed using systematic text condensation. 17 Qualitative methods are suitable for exploring experiences in areas where knowledge is scarce. 18 The interviews took place in February–March 2021 at two secondary care hospital ICUs in central eastern Norway. The study adheres to the COREQ guideline for reporting of qualitative data. 19
Participant selection and recruitment
We invited five Norwegian ICUs to be included in the study. Two units agreed to participate and received written study information that was distributed among nurses who were on day or night shifts on the prespecified day of the interview. The participant inclusion criteria included critical care nurses working in an ICU. Nurse educators or unit administrators served as a link between the researchers and informants in the recruitment process. The two focus group interviews were performed during regular work time, with four and five informants, respectively. The informants had between a few months and more than 20 years of experience as intensive care nurses. There was no prior relationship between the researchers and the informants.
Data collection
The focus group interviews had a duration of 90 minutes. The first author was moderator and led the conversation while the last author observed and took field notes. In line with Krueger and Casey, we developed a semi-structured interview guide that was used as an aid to start the conversations and provide some structure. 20 The semi-structured interview guide design is suitable for explorative studies, as it allows for detours and new aspects to be persecuted. 20 The interview guide included themes such as how double-checking influences workflow and planning, and the practical procedure of medication double-checking in the ICU. The conversations were carried out relatively independently of the guide, and both focus group interviews were recorded on electronic audiotape. The recordings were transferred to an encrypted memory stick, erased from the recording device and transcribed verbatim by the first author.
Ethical considerations
Participation in the study was voluntary, and the informants received written and verbal information about the study and data handling and gave their written consent to participate. The study was approved by the Norwegian Centre for Research Data (NSD) (reference number 492940) and the privacy legislation authorities at the two hospitals where the interviews were performed.
Analysis
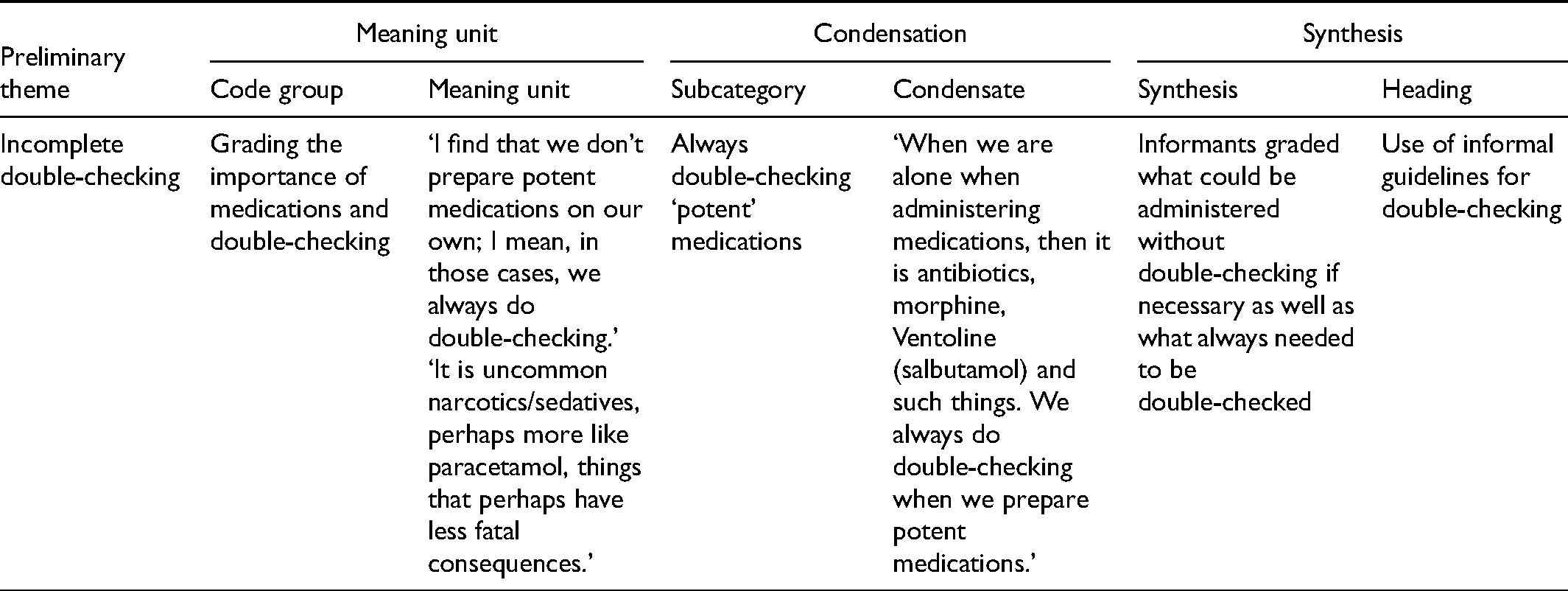
We used systematic text condensation to analyse the transcribed interviews. Systematic text condensation is a descriptive and explorative method for thematic and cross-case analysis. 17 Following Malterud, 17 a four-step analysis process was performed. The first and last author separately read the transcribed material thoroughly and identified preliminary themes independently. The transcripts were read multiple times to gain an understanding of the content. There was a high level of agreement about the preliminary themes. In the second step, meaning units in the text were identified, coded and grouped manually into categories and subcategories with the themes from step 1 as a point of departure. In step 3, the content of the categories and subcategories was decontextualised, reduced and summarised in a short text condensate that carried with it the main meaning of each category. In step 4, each category was recontextualised in a coherent text (presented in the Results section). The step-by-step process was not as straight forward as the description may indicate, it was rather a back-and-forth reflection and negotiation process resulting in the final analysis. All three authors agreed upon the final results (see Table 1).
Excerpts from the analysis.
Results
An overarching result of the study was that the informants experienced several barriers to performing medication double-checking. The informants talked about how they needed to adapt to the unit workload and had to prioritise double-checking against other important tasks. The data analysis revealed three main themes: ‘Organisational restraints’, ‘Using informal guidelines for double-checking’ and ‘Intensive care nurses lower their standards’. For confidentiality reasons, quotations are marked with an anonymous identifier, e.g. ‘Informant 2’.
Organisational restraints
A recurring theme in the data was ICU understaffing. The informants described a work environment with a frequent occurrence of having too few intensive care nurses to perform the designated tasks. Thus, double-checking was often not prioritised, particularly on evening and night shifts. The informants experienced barriers to double-checking all the medications that a patient was receiving. The medication preparation area was situated far from the patient rooms, and it was difficult to get another nurse to perform double-checking in the medication preparation area. One informant expressed, We don’t have time to stand in there [the medication preparation area] to get the double-checking done. Perhaps I left my patient's bedside, something that I shouldn’t have done in the first place. (Informant 3)
The informants were alone in the medication preparation area and felt that it was not always possible to get hold of a colleague who could perform double-checking. The physical location of single-patient rooms in relation to the other patient rooms, where other nurses were available, also influenced the ease with which help could be obtained in a single-patient room.
Double-checking requires planning
A prominent category under this theme is how the informants used planning to compensate for the lack of available colleagues. At both hospitals, it was common practice to have as many of the shift's medications as possible double-checked at the beginning of the shift. In particular, in the single-patient rooms, good planning was required in order to get the double-checking done because of difficulties in getting hold of a colleague at the time the medication was due: If you are in a room a bit further away from the rest of the staff … then, I think that you perhaps plan a bit better, that you get the double-checking done at the beginning of the shift. (Informant 7)
The nurse would get hold of a colleague and together they would prepare and double-check as much as possible of the medication for the whole shift. The informants also considered it to be good practice to prepare the medications for the first hours of the following shift and perform the double-checking during handover. That way, nurses on the next shift did not have to start their shift by retrieving medications from the medication preparation area.
Challenges of acute situations
In situations that called for fast action and medication changes, there was no room for planning, and performing double-checking was not always an option. The informants said that they often chose to administer medications without prior double-checking because they experienced that colleagues were unavailable and there was no time to wait for help. They described such a situation as a choice between waiting for double-checking and providing the patient with lifesaving and time-critical medications, e.g. vasopressor or midazolam. A delay in medication administration would in such cases be a threat to patient safety: You are in a situation where you can’t leave the patient, and you don’t have anyone with you. You have to give medications now, because you can’t wait. (Informant 5)
In situations of sudden changes in the patients’ conditions, the doctors frequently gave verbal orders that were heard by only one nurse, either face to face or on the phone. Despite using the mandatory closed-loop communication when giving and receiving verbal orders, the person who was designated to perform double-checking could not verify whether an order had actually been given. The use of verbal orders was described as relatively frequent, particularly on evening and night shifts. Several informants perceived this not to be safe. One informant expressed: And then the nurse performing double-checking together with me has to trust that what I am saying is correct, because only I heard it or received the order on the phone. (Informant 3)
The informants expressed that they trusted their colleagues and that they signed off the double-check despite the lack of a written order. The trust between colleagues was particularly important on night shifts, when fewer intensive care nurses were present.
Having to adjust to the unit's pace
The informants adjusted the standard of medication administration to the number of people on the shift and the unit's workload. By omitting the double-checking of less potent medications, a better flow in patient care could be achieved. The threshold for asking for help with double-checking was higher if colleagues were busy. At the same time, the nurses expressed that being interrupted was part of their job and was thus to be expected. One informant described the situation as follows: I feel that people seldom sit down; people are out and about, keeping busy, and there is perhaps a greater barrier to interrupting them [and asking for help with double-checking] then. (Informant 6)
Double-checking was often performed when retrieving opioids from the narcotics storage. However, double-checking upon preparation and administration was often omitted. One reason for not performing double-checking was the need for titrating with many small doses. Another drug that I think that we seldom double-check is IV OxyNorm [oxycodon], because maybe you prepare a syringe, and then you are giving two to three milligrams, then you use the same syringe. (Informant 8)
For a newly graduated intensive care nurse, the threshold was high to administer medications without double-checking. However, this threshold decreased as time went by and the nurse gained more confidence in his/her job.
Using informal guidelines for double-checking
This category describes how the informants use informal guidelines for when to perform double-checking and how these informal guidelines relate to the unit's double-checking procedure. The informants did not actively apply the units’ procedures for medication double-checking. One of the units had, according to the informants, no updated procedure for medication double-checking. In the other unit, several informants had not read the procedure or had done so several years ago and did not know the content of it. Some informants felt that a procedure for double-checking was not needed, as they had good knowledge of medication administration and double-checking was a basic procedure that all nurses should be familiar with: When you have finished three years of undergraduate [bachelor] studies, then it is expected that people know how to check a medication. … And then I think that you almost don’t need a procedure, because it's in your education. (Informant 6)
In both focus groups, there was a general agreement that it was not always possible to get all medications double-checked. Some medications had to be administered without double-checking because the patient's condition did not allow for a delay in medication administration, due to either clinical deterioration, pain or discomfort. The informants graded what could be administered without double-checking if necessary and what always needed to be double-checked. These informal guidelines resulted in potent medications in infusion pumps, such as sedation and noradrenaline, always being double-checked whereas medications such as ipratropium bromide and salbutamol, opioid boluses for pain relief, IV paracetamol and antibiotics could, according to several informants, be administered without double-checking if it was difficult getting hold of a colleague or if the unit was busy.
Some informants said that they sometimes experienced that their colleagues asked for a signature so that the records looked right, but that the medication, in fact, had not been double-checked: Sometimes, I feel that we want that signature just to get a signature, sort of. (Informant 6)
In these cases, the medication could already have been administered or prepared, and thus, it was not possible to perform proper double-checking.
Intensive care nurses lower their standards
This category describes the informants’ discomfort when feeling forced to skip double-checking when administering medications that they think should be double-checked. The informants said that they were afraid of making mistakes and that double-checking felt safe. Several informants had experienced situations in which errors had been made and said that double-checking was necessary and good practice to ensure safe medication administration. The informants experienced discomfort when not getting medications double-checked in the way that they wished, and several described a situation of lowering their standards, something that threatened their feeling of integrity. Skipping double-checking felt unpleasant and unsafe. However, in some situations, the alternative was perceived as not being an option: If my patient is in major pain at 3:00 a.m., and a ready-prepared syringe with morphine is there, and I have a doctor's order, then I would have felt a lot more discomfort as a nurse, thinking that, no, I have to wait until a colleague finishes with patient care in 20 min before you can get pain relief; to me, it is an obvious choice to give the morphine. (Informant 3)
The informants described a strong obligation towards their patients who were in acute need of medications but said that it felt unpleasant and unsafe to administer medications without double-checking. They said that not performing double-checking put the patient at risk. However, the patient's need for medication was often perceived as more important.
Discussion
The aim of this study was to explore Norwegian ICU nurses’ perceptions about the practicing of medication double-checking in the ICU. The informants were faced with difficult dilemmas with conflicting requirements and considerations. Time constraints, understaffing and the resulting high workload create a need to prioritise between double-checking and other important tasks. The informants described dilemmas in which the patient's need for medications may sometimes conflict with safe medication administration and double-checking procedures. The informants lowered their standards when they performed actions that are not considered good practice according to Norwegian medication administration regulations. Intensive care nurses found that administration of medications without double-checking felt unpleasant and unsafe.
Organisational restraints
Time constraints and difficulties in getting hold of a colleague were common reasons for not performing double-checking. This is in agreement with nurses’ reports from other areas of Norwegian health care. 9 Also, internationally, lack of time and understaffing are known barriers to performing double-checking. 16 The informants wanted to perform double-checking consistently but often experienced that it was not possible. Understaffing and time constraints are not only barriers to double-checking but also reduce the quality of the double-checking that is actually performed. 16 The Covid-19 pandemic made the shortage of intensive care nurses evident through a vicious circle of vacant shifts, which resulted in increased stress, sick leaves and more understaffing. Understaffing and stress in the workplace have been reported to be the main causes of nurses leaving their jobs. 21 The informants in the study experienced feelings of discomfort and insecurity when having to omit double-checking. They felt that they had to lower their standards and perform a suboptimal job, another common reason for nurses to leave their jobs. 21
Planning ahead made the informants able to perform double-checking even when they were in a single-patient room and when the unit was busy. Still, an unpredictable work day with acute and critically sick patients and a frequent need for administering non-prescribed medications or at not predetermined times were factors that made double-checking less feasible. In these acute situations, the risk of error is higher, and double-checking should be performed. 22 When the level of staffing does not allow for performing double-checking, organisations do not practice in agreement with the medication administration regulations. These regulations state that the head of an organisation is responsible for a safe medication administration practice and that the organisation should be organised in a way that allows staff to fulfil their duties as required by law.5,23 The informants described the challenges of performing double-checking in single-patient rooms and this should be accounted for when planning new hospital buildings and ICUs. The physical unit design should allow for easy access to medication double-checking.
Use of informal guidelines is not in agreement with Norwegian regulations but with international recommendations
The informants felt that they were often forced to skip medication double-checking. Double-checking in the ICU context can be challenging due to the acute and unpredictable nature of the critically ill patient and the resulting frequent need for changes in multiple medications. However, in specific situations, double-checking was always performed. In that respect, informal guidelines existed as to which medications were important in terms of double-checking, and which were not. The informal guidelines implied that all medications that were administered via infusion pump, e.g. sedation and vasopressors, were always double-checked.
The existence of informal guidelines may explain why the informants did not have a perceived need for a unit procedure for double-checking. The practice was well established in the unit culture. Another possibility is that a procedure seemed less relevant, as it potentially would not reflect real life and what was perceived as feasible and relevant to intensive care nurses. It is, however, interesting that informants at both units were not familiar with the existence of a local procedure. This is not in agreement with medication administration regulations that state that such procedures should be known to everyone working in the unit. 5 The law regulating health care workers’ practice includes a requirement that health care workers keep up to date with current knowledge and best practice guidelines. 23
The internal and informal guidelines for determining which medications need double-checking violate the recommendations of the Norwegian medication administration regulations as well as local procedures at the larger Norwegian hospitals. These university hospital guidelines state that most medications that are administered to intensive care patients should be double-checked. Interestingly, a graded approach to double-checking is in agreement with international recommendations.5–7,24 The Institute for Safe Medication Practices (ISMP) is an organisation that works for the safe use of medications and the prevention of medication administration errors. Contrary to Norwegian regulations, ISMP recommends that double-checking be reserved for selected medications associated with a particularly high risk. The ISMP recommendations resemble the practice described by our informants: that double-checking is always performed only with the most potent medications.5,24,25 Still, the informants strove to work in compliance with the Norwegian regulations, although they, unfortunately, felt obligated to practice in disagreement with the regulations on many of their shifts. To allow ICU staff to practice according to Norwegian medication administration regulations, options could include increasing staffing or adjusting the regulations towards the recommendations from ISMP.
In both focus groups the consensus was that double-checking was an important and required measure for patient safety. This finding is in disagreement with studies that found that nurses perceived double-checking to be of bad quality and performed as an automated action and that double-checking was only a means to reduce nurses’ individual responsibility.16,22,26 This discrepancy may be explained by the ICU nurses working in an environment with more frequent use of potent medications or that the practice is rooted in the unit culture in such a way that nobody questions it.
Strong obligation towards the patient
In situations in which a delay in medication administration could result in deterioration of the patient's condition or prolonging of the patient's pain or discomfort, the intensive care nurses prioritised administration of potent medications without double-checking. We interpret this pattern of actions as being in agreement with the nurse care philosophy and the nurse's unique responsibility as the one closest to the patient. In this situation, an ethical obligation makes the nurse defy procedures and regulations to ensure that the patient's need for alleviation and curation is addressed. 27 However, medication administration without double-checking created a feeling of insecurity and discomfort in the informants, as it carried with it a risk of harm as a result of errors in the administration of potent medications. The intensive care nurse puts him/herself at risk of experiencing the psychological burden associated with medication administration error. 22
Strengths and limitations
This study provides a valuable insight into intensive care nurses’ experiences with and attitudes towards double-checking in Norwegian ICUs. This has not previously been explored in the literature. The study may provide food for thought and discussion about the practice of double-checking in the ICU as well as unit design and the revision of procedures for double-checking. The two focus group interviews together included nine informants, who provided rich data with a high degree of agreement between the two interviews.
The data collection was performed in the winter of 2021, and the study's finding of organisational barriers to performing double-checking could have been influenced by a higher than usual activity level in the ICU during the Covid-19 pandemic. The data collection was performed in ICUs located at secondary care hospitals, which might indicate that staffing (but also complexity and workload) is lower than in university hospital ICUs. 28 The focus group interviews were performed during working hours which limited the number of participants from a single shift who could participate. This may limit the relevance of some of the findings.
Conclusion
The study uncovers a mismatch between laws and regulations about medication double-checking and what intensive care nurses perceive as being feasible in a busy and understaffed work reality. Medication administration is being practiced in agreement with international guidelines that recommend a graded approach to double-checking. Compliance with the Norwegian medication administration regulations and procedures from the large university hospitals does not seem feasible in the two study ICUs, particularly on evening and night shifts. Thus, ICU nurses have adapted their culture and use informal guidelines for what medications to double-check. A further discussion about potential reasons for the discrepancy in medication double-checking between the Norwegian medication administration regulations and the practice found in this study is needed. It seems necessary to specifying feasible requirements for ICU double-checking and increased staffing. Together, such changes could contribute to reducing the stress and insecurity associated with the lowering of standards that ICU nurses in the study experienced. Furthermore, this could contribute to keeping nurses in intensive care and preventing them from changing their workplace to a less stressful environment. Future research should aim to clarify whether the challenges identified in this study apply to ICUs nationwide and how they best can be resolved.
Footnotes
Author contributions
The first and last authors (Vegard Sletten Ek (VSE) and Marianne Trygg Solberg (MTS)) chose the design and method and agreed on a progress plan. VSE and MTS planned the focus group interviews and interview guide. VSE was the moderator and MTS was observer and took notes. VSE and MTS performed the stepwise data analysis, supported by Anne Lee Solevåg (ALS). With substantial contributions from ALS and MTS, VSE interpretated the data and results. VSE wrote the article, MTS and ALS has co-written the final version of the manuscript. All the authors (VSE, ALS and MTS) contributed to critically revising the manuscript for content and have given final approval to publish in the Nordic Journal of Nursing Research.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for profit sectors.