
Abstract
Background and aim
Previous studies have deemed pharmacists essential in the intensive care units (ICU) to provide quality healthcare and ensure medication safety. As the impact of pharmacists in ICU varies according to different factors, our study aims to characterise and evaluate the impact of pharmacists’ interventions in ICUs in Singapore, to enable the identification of areas of improvement in our critical care pharmacy practice.
Methods
We retrospectively evaluated 7 months of pharmacists’ interventions in five ICUs at Singapore General Hospital. Interventions were classified based on the medication-related problems (MRPs) addressed. The impact of pharmacists’ interventions was assessed by rating the severity of error in medication order, the clinical relevance of intervention, and the probability of adverse drug events (pADE) that would have occurred without pharmacists’ interventions.
Results
There were 619 interventions addressing 775 MRPs, of which 91.1% were accepted. The main MRP identified was inappropriate drug regimen (49.2%) and the medication class most frequently involved in MRPs was anti-infectives (56.9%). Majority of the interventions were rated as significant for both the severity of error (76.9%) and clinical relevance (72.4%). However, the pADE was deemed to be low (61.2%). The rating of pADE may be affected by the lack of information in patient profiles.
Conclusion
This study demonstrated the crucial role of pharmacists in ensuring medication safety in ICUs. Possible areas of service improvement include educating medical residents on common medication errors and empowering pharmacists towards collaborative prescribing.
Introduction
Medication errors were estimated to cause 44,000–98,000 deaths every year according to “To Err is Human” by the Institute of Medicine. 1 Bates et al. reported 5.3 medication errors for every 100 medication orders, 2 illustrating the inadequacies of healthcare provided to patients. Critically ill patients are more prone to medication errors and adverse drug events (ADEs) due to their complex conditions, use of multiple medications and constant changes in their pharmacokinetics and organ function.3–6 The rate of ADEs was found to be two times higher in intensive care units (ICUs) compared to non-ICU settings. 3 ADEs can adversely impact patient outcomes, leading to an increase in the length of hospital stay and the need for additional treatments which result in higher healthcare costs.7–10
The Society of Critical Care Medicine (SCCM) deemed pharmacists essential in ICU to provide quality healthcare and ensure medication safety.11,12 International studies done on the impact of critical care pharmacists demonstrated that pharmacists help to reduce patient harm,13–18 improve patient outcomes,19,20 and reduce medical costs in ICUs.13–17 A landmark study done by Leape et al. reported that pharmacists in ICUs resulted in a 66% reduction of ADEs. 14 However, such studies done on the impact of pharmacists in ICUs are largely from North America and Europe, with paucity of data from Southeast Asia. A Taiwanese study examined the pharmaceutical interventions made by clinical pharmacists in the ICU and their associated risk factors but not their impact on patient outcomes, 21 while a study conducted in Malaysia attempted to determine the value of pharmacists’ interventions in the management of clinically significant drug-drug interactions, of which majority were categorised as Type-C severity level. 22
In addition, the impact of pharmacists in ICUs can vary with different factors and in different settings. Firstly, the type of interventions can vary with different ICU settings. Bourne et al. reported significantly more interventions on patient safety in the neurology and cardiac ICUs compared to general ICUs (p ≤ .001). 23 Secondly, the impact of pharmacists depends on their knowledge, skills, and experiences.24–26 One study found that consultant pharmacists had a higher intervention rate (22.6%) than foundation level pharmacists (16.4%) and newly qualified pharmacists (11.1%). 24 Thirdly, the availability of weekend pharmacy services can influence the impact of pharmacists in ICU. The intervention rate was found to be two times higher on weekends (33.6%) compared to weekdays (16.1%) (p < .0001). 24
Hence, this study aims to evaluate pharmacists’ clinical impact in ICUs in Singapore, which will allow us to identify possible areas of improvement to enhance pharmacists’ impact on patient care, justify the resources used to train critical care pharmacists and expand critical care pharmacy practice.
Aim of the study
The objectives of this study are to (1) characterise the different types of pharmacists’ interventions, (2) rate the severity of error in medication orders and the clinical relevance of interventions, and (3) determine the probability of ADE (pADE) occurring without pharmacists’ interventions.
Ethics approval
This is a service evaluation study. The Singhealth Centralised Institutional Review Board has confirmed that no ethical approval is required.
Method
Study setting
This retrospective study was conducted in Singapore General Hospital, the oldest and largest academic and tertiary acute care hospital in Singapore. There are eight ICU pharmacists covering a total of 54 ICU beds in five ICUs (surgical, medical, neurosurgical, cardiothoracic, and burns) daily. These pharmacists have varying levels of ICU working experience but most of them had either in-house critical care training or 1-year residency training in ICU. The medical staff in ICU consist of mainly intensivists and residents. ICU pharmacists are available every Monday to Friday and Saturday mornings. Medication orders and drug enquiries from ICUs on weekends and public holidays are verified by general pharmacists. ICU pharmacists review medication orders and patient charts to assess the appropriateness of each prescribed medication, perform medication reconciliation, therapeutic drug monitoring, and go on ward rounds. Any detected errors in the medication orders are discussed with intensivists and the interventions are documented in the Sunrise Clinical Manager system (SCM), which is an electronic patient record and prescribing platform.
Data collection
Intensive care units pharmacists’ interventions for 7 months in 2020 were extracted from SCM. The following data were collected: age and gender of patient, type of medication-related problem (MRPs), type of pharmacist’s recommendation, how medication error was identified, prescribed order, description of intervention, significance of intervention, intervention acceptance, and amount of time spent in making the intervention.
Outcome measures
The impact of pharmacists’ interventions in ICU was assessed by (1) rating the severity of error in medication order and the clinical relevance of intervention using the method by Overhage et al. 27 and (2) determining the pADE occurring without pharmacist’s intervention using the method by Nesbit et al. 28
Intervention classification
Interventions were categorised into MRPs and FASTHUGS-BID. The MRPs (Table S1) were adapted from the studies by Hepler and Strand and Cipolle et al.29,30 FASTHUGS-BID (Table S2) is a mnemonic that emphasises the essential aspects of patient care in ICU.31,32 By classifying interventions into MRPs and FASTHUGS-BID, it illustrates the impact of pharmacists in addressing the needs of critically ill patients. Medications involved in MRPs were classified according to the anatomical therapeutic chemical classification system (ATC). The pharmacist who made the intervention classified the MRP. This classification was reviewed by an investigator and an ICU pharmacist to ensure accuracy.
Evaluation of interventions
Interventions were rated on the severity of error in medication order on a scale of A to E and the clinical relevance of intervention on a scale of one to six using the method by Overhage et al. 27 This is a validated method that is widely used by other studies. The rating value was assigned based on information in Table S3 provided by Overhage et al. and other studies that adopted this method.16,33,34
Interventions were analysed to determine the pADE occurring without pharmacists’ interventions. The pADE was set at 0, 0.01, 0.1, 0.4, or 0.6, using the method by Nesbit et al., with a maximum of 0.6 to maintain conservative bias. 28 The assumption was that no interventions would increase the pADE. The pADE was assigned using the information in Table S4 provided by Nesbit et al. and other studies that adopted this method.16,17,33,34 If no information was available, the assignment was based on clinical judgment.
Rating of interventions
A total of 50 unique interventions were selected using stratified random sampling based on MRP. The proportion of MRP in this sample was representative of that in the total interventions evaluated. This sample was rated by the investigator, ICU pharmacist, and intensivist independently. Inter-rater reliability assessment was performed to determine the degree of agreement between the evaluators. 35 Differences in the rating were discussed among the evaluators to reach a consensus. If there was a moderate or higher level of agreement, the investigator would proceed to rate the remaining interventions based on the derived consensus. A list of standardised intervention codes similar to that developed by Overhage et al. was created to serve as a guide for the investigator to rate the remaining interventions (Table S5).
Statistical analysis
All pharmacy interventions were recorded in an Excel database from which descriptive data statistics were performed. Fleiss’ Kappa statistics were calculated using IBM SPSS Statistic (Version 26) software to determine the inter-rater reliability.
Results
There were 619 pharmacists’ interventions and 91.1% were accepted by the intensivists. 5.0% of the interventions were not accepted and 3.9% had unknown acceptance outcomes.
Number and proportion of medication-related problems identified.

Number and proportion of interventions classified according to FASTHUGS-BID.

Medications classified according to ATC classification system.

The Fleiss’ Kappa for the inter-rater reliability between the investigator, ICU pharmacist, and ICU intensivist for the sample of 50 interventions were 0.50, 0.64 and 0.57 for severity of error, clinical relevance and pADE, respectively (p < .001). As this represented a moderate strength of agreement among the 3 raters, the investigator rated the remaining interventions.
Figure 1 summarises the rating of pharmacists’ interventions. The majority of interventions were rated as significant for both the severity of error (76.9%) and clinical relevance (72.4%). Pharmacists’ interventions were largely determined to have a low pADE (61.2%). None of the interventions were considered to be potentially lethal, extremely significant, or have a high pADE. (a) Ratings of pharmacists’ interventions for the severity of error in medication errors. (b) Ratings of pharmacists’ interventions for clinical relevance. (c) Ratings of pharmacists’ interventions for probability of adverse drug event.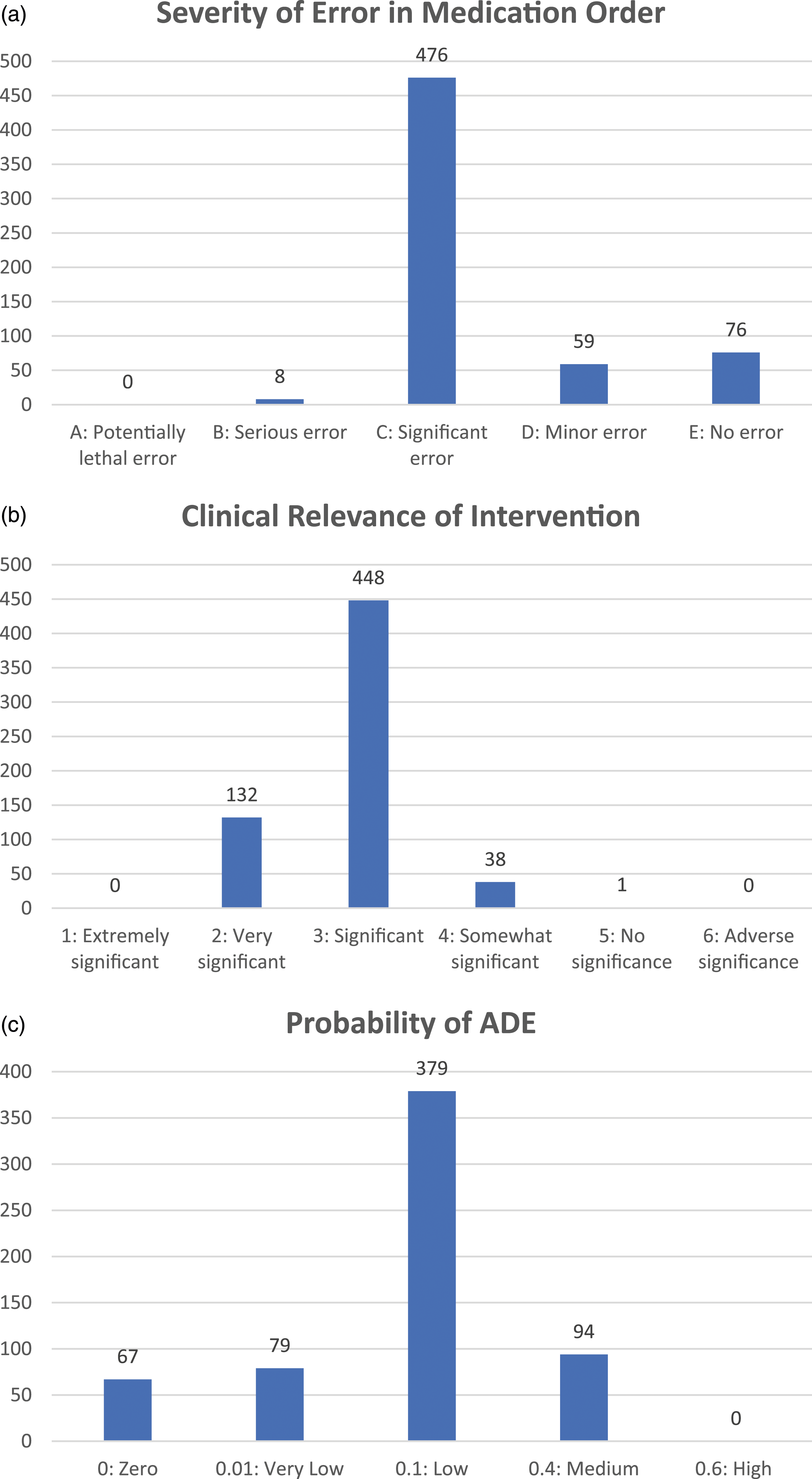
Discussion
In this study, we evaluated the clinical impact of pharmacists’ interventions in the ICUs in our institution. A significant number of interventions and MRPs were addressed by the pharmacists without which patient care would have been compromised. The level of acceptance was high (91.1%) and is comparable to other studies, such as that by Bourne et al. who reported 90% acceptance. 23 This demonstrates that intensivists highly valued pharmacists’ interventions.
The main MRPs identified by pharmacists were inappropriate drug regimens, where common interventions involved dose adjustment according to the mode of dialysis and renal function. This is similar to what has been reported in some studies.15,21,36–38 Critically ill patients often experience changes in their pharmacokinetics and renal function. This is where pharmacists are crucial in effecting prompt adjustments to the medication therapies of these patients. The study conducted in Taiwan found that patients with renal dysfunction required more pharmaceutical interventions than patients with normal renal function (odds ratio = 1.63; 95% confidence interval 1.31–2.01). 21 In contrast, there are other studies such as Leape et al. who found that 45% of interventions involved clarification of orders. 14 In our study, most of the interventions that were originally classified as clarification of drug orders were reclassified to better reflect the MRPs. The different types of interventions reported by various studies may be due to the lack of standardised definitions to classify pharmacists’ interventions.
The medication class most commonly involved in MRPs was antibiotics and this is consistent with multiple studies.15,17,21,36,37 Vincent et al. reported that 70% of patients received antibiotic treatment during their stay in ICU. 39 Hence, as a frequently prescribed medication in ICU, it is more likely for antibiotics to be associated with MRPs. Pharmacists commonly intervened to adjust the dose of antibiotics, to stop antibiotics when no longer indicated, to remove duplicate antibiotic therapies, and to de-escalate antibiotics based on culture results. This demonstrates the role of pharmacists in ICU as advocates for antimicrobial stewardship to promote optimal use of antimicrobial agents.
The majority of pharmacists’ interventions were rated as significant for both the severity of error and clinical relevance, which is also seen in the study by Bosma et al. 16 The pADE scores were largely low and medium, similar to findings obtained in other studies.13,16,33,34 However, Gallagher et al. found that 2.8% of the interventions had high pADE. These mainly involved omissions of essential medications such as anti-epileptic drugs or serious drug interactions e.g., no dose adjustment of digoxin when amiodarone was initiated. 34 In comparison, none of the interventions in this study were evaluated to have high pADE. Such recommendations may have been made during ward rounds with changes effected on the spot and hence not documented.
There were limited number of pharmacists’ interventions related to FASTHUGS-BID. This could be due to the fact that FASTHUGS-BID is currently included as a checklist for our doctors to review when making plans for our ICU patients daily. For example, most patients would already be placed on stress ulcer prophylaxis by the doctors after reviewing the checklist, with pharmacists’ interventions focusing mostly on switching to oral options and discontinuing them where appropriate. Moreover, de-escalation of antibiotics requires considerations of multiple factors and hence such recommendations by our pharmacists are likely to be made during ward rounds, and may not be captured as interventions. There were no interventions relating to head of the bed elevation, spontaneous breathing trial, and indwelling catheter removal. This reveals areas where pharmacists can be more proactive in enhancing their impact on patient care. In a study looking at pharmacists’ leadership in ICU quality improvement, Stollings and colleagues reported that the inclusion of pharmacists in awakening and breathing trials for critically ill patients led to a significant increase in compliance with the guidelines. 40 The Awakening and Breathing Coordination, Delirium monitoring/management, and Early exercise/mobility (ABCDE) bundle is an example of an interprofessional, evidence-based, multicomponent ICU management strategy aimed at reducing sedation exposure, duration of mechanical ventilation, and ICU-acquired delirium and weakness. 41 Future studies may want to explore pharmacists’ role in the ABCDE bundle.
Areas of service improvement
Identifying common MRPs in ICUs will allow pharmacists to take a step further in preventing ADEs and optimising patient safety. One example is to develop and implement drug therapy protocols to facilitate safe prescribing by the ICU medical residents. Another example is to provide education to new ICU residents on the common MRPs in ICU such as appropriate dose adjustment of medications according to the patients’ clinical condition and renal function. Kessemeier et al. reported significantly lesser prescribing errors after pharmacists conducted weekly educational sessions and sent reminder emails to physicians on the prescribing errors. 18 This ensures continuous learning and helps to improve patient safety.
Secondly, collaborative prescribing in ICUs can help to improve efficiency in patient care. Many interventions in this study involved dose adjustment according to patient’s renal function and mode of dialysis. These interventions were usually accepted and rated as clinically significant. Hence, empowering critical care pharmacists to make independent dose adjustments may potentially improve safe prescribing and allow critically ill patients receive their appropriate medication therapy promptly.
Study limitations
Firstly, as this is a retrospective study, there is possibility of incomplete and inaccurate data. Not all pharmacists’ interventions were documented. Interventions from ward rounds were often not documented because pharmacists viewed their recommendations as part of the multidisciplinary team discussion rather than an intervention to correct an error. Hence, this study may have underestimated pharmacists’ impact in ICU. Additionally, there was a lack of contextual details to evaluate pharmacists’ interventions. The evaluators assessed the interventions based on what was documented in SCM, which was dependent on how detailed and accurate the pharmacists documented their interventions. Information on the patient profile such as the severity of illness and comorbidities was not provided. Hence, this could have affected the accuracy of the assessment.
Secondly, the level of agreement was lower than desired (Kappa ≥0.6).35,42 The rating of interventions can be difficult when assigned based on clinical judgement and lack of contextual details. Previously published studies reported similar Kappa results.13,33 Kopp et al. found Kappa to be 0.25 for the severity of error and 0.41 for pADE. This shows the difficulty in achieving high levels of agreement. Thus, it is crucial for the evaluators to discuss the differences in ratings when these arise to come to a mutual understanding and agreement. A list of standardised intervention codes was also created to guide the investigator in the rating of the remaining interventions to help ensure appropriate and consistent ratings.
Thirdly, the evaluation of pharmacists’ impact in ICUs using pADE was limited by the assumption that the MRPs were only be identified by pharmacists and hence no interventions would increase pADE. Hence, the pADE in this study might be overestimated. Separately, this study could be strengthened by performing an economic assessment on pharmacists’ impact in ICUs. 43 Bosma et al. reported that pharmacists’ interventions resulted in a cost avoidance of €28,000 and that the use of ADE costs from different studies led to a large difference in the resulting cost-benefit ratio. 16 The cost-benefit ratio increased from 3.34 to 18.98 when the cost of ADE from Bates et al. 44 was used instead of that from Rottenkolber et al. 45
Finally, this was a single-centre study performed during COVID-19 pandemic. However, conducting the study during non-pandemic times is unlikely going to change the study results as pharmacists’ services in ICUs in SGH remained the same throughout the COVID-19 pandemic. To fully reflect the impact of critical care pharmacists in Singapore, future studies involving ICUs from multiple centres are needed. Utilising a standardised method to classify pharmacists’ interventions in ICU would also allow easier comparison across different studies.
Conclusion
In this study, we characterised and evaluated pharmacists’ interventions in the ICU by looking at the severity of error, the clinical relevance, and the pADE. Our findings revealed that pharmacists' interventions were mainly targeted at inappropriate drug regimens, and antibiotics were commonly involved in MRPs. Pharmacists’ interventions were evaluated to have addressed significant errors in medication orders and were clinically relevant to patient care. However, the pADE was deemed to be low.
This study provides insight into the vital roles that pharmacists play in the ICU team to ensure appropriate medication therapy and advocate for antimicrobial stewardship. However, there are areas where pharmacists can improve to further enhance their impact in ICU. Such areas include expanding pharmacists’ roles in other aspects of ICU care e.g., the ABCDE bundle, educating the residents on common errors in medication orders, and empowering pharmacists towards collaborative prescribing.
Supplemental Material
Supplemental Material - Clinical impact of pharmacists’ interventions in intensive care units in a tertiary institution in Singapore – A retrospective cohort study
Supplemental Material for Clinical impact of pharmacists’ interventions in intensive care units in a tertiary institution in Singapore – A retrospective cohort study by Jie Lin Soong, Lee Yi Ang, Jeremy Lin En Chan and Sui An Lie in Proceedings of Singapore Healthcare
Data availability statement
All data generated or analysed during this study are included in this published article.
Footnotes
Author contributions
Jie Lin Soong first proposed the study idea and all authors contributed to the final study design. Data collection and analysis were performed by Lee Yi Ang, Jeremy Chan, and Jie Lin Soong. The first draft of the manuscript was written by Lee Yi Ang and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.