
Abstract
Objectives
To develop and evaluate the Prosthodontic Workflow Tracking System (PWTS) for improving delivery efficiency and traceability in clinic–dental laboratory workflows across medical center branches.
Methods
From May 2022 to September 2023, prosthodontic work-item transfer episodes between clinics and a dental laboratory across medical center branches were prospectively recruited under routine clinical operations and managed using either PWTS (digital tracking) or a paper-based workflow. PWTS recorded time-stamped scans at predefined checkpoints and synchronized events to a cloud dashboard for real-time status visualization and automated overdue alerts. Delay was defined as the completion of any checkpoint after the scheduled due date. Delay incidence was compared using chi-square tests, and delayed days using the Mann–Whitney U test. Administrative workload was estimated using time–motion observation and system logs. Post-intervention user experience was assessed using 5-point Likert scales.
Results
A total of 154 transfer episodes were included (PWTS n = 84; paper-based n = 70). Delay incidence was lower in PWTS than in the paper-based workflow (17.9% vs 52.9%; χ2 = 19.38, p < 0.001). Cumulative delayed days were 262 (PWTS) versus 408 (paper-based), and mean delayed days per episode were 3.12 versus 5.83, respectively (p < 0.001). Administrative workload was estimated at 30 staff-hours per month. User experience indicated high perceived benefit (4.0–4.5/5), moderate satisfaction and continued-use intention (3.5/5), and lower usability for impression movement tracking (2.5/5).
Conclusion
PWTS was associated with lower delay incidence and delay burden than a paper-based workflow, and user-reported experience measures highlighted priorities for future system refinement.
Introduction
Oral and dental health are integral to overall well-being,1–4 with tooth loss associated with impaired mastication, reduced nutritional intake, and an elevated risk of systemic conditions such as cardiovascular disease, diabetes mellitus, malignancies and cognitive decline.5–9 Timely dental intervention and prosthetic rehabilitation are essential for maintaining both oral and systemic health. However, fabrication of fixed dental prostheses remains labor-intensive and time-consuming, typically requiring multiple clinic–laboratory exchanges (e.g., impression transfer, try-ins, and adjustments) over several weeks. This multi-step, distributed workflow is prone to incomplete or unclear prescriptions and communication errors, and it provides limited end-to-end traceability of dental models across handoffs. Consequently, additional clarification, rework, and coordination are often required, increasing administrative workload and contributing to delivery delays that may negatively affect the patient experience.10–12
Recent advances in wireless technologies such as Radio-Frequency Identification (RFID) and Near Field Communication (NFC) have demonstrated considerable potential in addressing operational inefficiencies within healthcare systems.13–15 RFID enables contactless wireless identification and tracking of physical items that have RFID tags attached via electromagnetic coupling between the tag and the reader, allowing passive data exchange. Because this approach provides rapid and reliable item-level identification, RFID has been widely used for logistics management, medical inventory control, and asset tracking.16,17 NFC enables secure, low-power, two-way communication within 10 cm, which has established it as a standard technology for authentication and payment applications.18,19 In clinical settings, NFC is increasingly adopted to enhance service efficiency by enabling rapid point-of-care verification and reducing manual data entry and administrative processing. It may also improve patient safety by strengthening identification accuracy and matching at critical steps (e.g., verifying the correct patient, item, or procedure) and by supporting clearer accountability through electronically recorded checks at handoff points.20–25
RFID and NFC technologies have been applied in healthcare to support real-time identification, traceability, and workflow visibility across medication safety, patient services, and healthcare logistics. Aldughayfiq and Sampalli 26 developed an NFC-based mobile application to reduce medication prescribing and dispensing errors and reported favorable user feedback and improved error identification compared with traditional approaches. Alzahrani and Alnfiai 27 proposed an NFC-based guidance system to deliver user-friendly, language-accessible prescription information for older adults and non-native speakers, with high satisfaction reported by both patients and pharmacists. During the COVID-19 pandemic, Ebere et al. 28 integrated NFC with mobile networks for patient identification and management and reported favorable usability and user acceptance based on a Technology Acceptance Model evaluation. Beyond patient-facing applications, tracking technologies have also been explored in healthcare supply chains. Nanda, Panda, and Dash 29 proposed the Novel Approach for Integrated IoT with Blockchain in Health Supply Chain (NAIBHSC) to enable real-time monitoring and decentralized tracking of medical products, demonstrating favorable performance in simulation settings. In addition, Patil et al. 29 presented an NFC-enabled smart pillbox design to support real-time medication inventory tracking, emphasizing usability for home-based care and telemedicine contexts.
Collectively, these studies indicate the feasibility of scan- or tag-based technologies for supporting coordination and traceability in handoff-intensive healthcare workflows. However, prosthodontic workflows—particularly clinic–laboratory transfers of prosthodontic work items such as impressions and restorations—remain largely dependent on paper-based documentation and conventional delivery processes. Such practices may limit information completeness, workflow visibility, and timely coordination across handoffs.10,11 To date, relatively few studies have examined event-based, real-time tracking approaches specifically applied to prosthodontic clinic–laboratory transfers. Therefore, the aims of this study were to develop and evaluate a prosthodontic workflow tracking system (PWTS) for clinic–laboratory transfers of prosthodontic work items. We assessed delivery efficiency by comparing delay incidence and delay burden (delayed days) between PWTS-managed and paper-based workflows. Post-implementation user experience among clinical staff was assessed using questionnaire-based ratings of satisfaction and perceived usability.
Methods
We developed and field-evaluated an NFC- and IoT-enabled prosthodontic workflow tracking system (PWTS) to support workflow traceability and delivery efficiency in clinic–dental laboratory transfers of prosthodontic work items across medical center branches. We conducted two sequential phases: (1) system development and (2) prospective field validation under routine operations.
Phase 1 System development
We designed and implemented PWTS as a scan-driven workflow tracking system for prosthodontic case transfers between dental clinics and a dental laboratory across medical center branches. The tracked unit was the case transfer bag used to carry work materials (e.g., impressions/case materials to the laboratory and laboratory outputs back to the clinic), which was identified using RFID/NFC tags. We defined standardized workflow checkpoints spanning clinic dispatch, laboratory intake, laboratory completion, clinic return, and case closure, and generated scan-triggered, time-stamped events at each checkpoint. These events were synchronized to a centralized cloud database and dashboard to enable real-time status visualization and automated overdue alerts.
Three-tier architecture
The system adopted a three-tier architecture (Figure 1)—Firmware Layer, Back-End Layer, and Front-End Layer to provide an integrated workflow for data acquisition, transmission, storage, and real-time interaction. At the Firmware Layer, RFID/NFC readers were deployed at clinical and laboratory workstations to capture contactless scan events. In our implementation, the tracked unit was the case transfer bag (tagged with an NFC label) used to transport case materials to the laboratory and to return laboratory outputs to the clinic for subsequent clinical steps and case closure. Each scan event automatically created or updated the corresponding case record with a time-stamped checkpoint, thereby enabling end-to-end traceability across handoffs. This automation reduced manual data entry, minimized workflow interruption, and maintained real-time synchronization with the back-end system, improving operational accuracy and efficiency in clinical logistics (Figure 2).

System architecture of the prosthodontic workflow tracking system.

Workflow-oriented architecture of the prosthodontic workflow tracking system.
The Back-End Layer was hosted on Amazon Lightsail (a cloud-based virtual private server) to support high availability and stable operation. The infrastructure used NGINX (Engine X) as a reverse proxy and load balancer to route requests efficiently, and all communications were protected by Hypertext Transfer Protocol Secure (HTTPS) for encrypted data transmission. Back-end services were executed by Gunicorn (Green Unicorn), a Python Web Server Gateway Interface (WSGI) server configured to handle concurrent requests, and implemented using Flask (a Python web framework) to provide Representational State Transfer application programming interfaces (REST APIs) for standardized data creation, update, and retrieval. Structured data were stored in PostgreSQL (Postgres Structured Query Language), a relational database with atomicity, consistency, isolation, and durability (ACID)-compliant transactions to ensure data integrity and reliability. LINE Notify (LINE notification service) was integrated to deliver real-time, token-authenticated notifications (e.g., status updates and return alerts). Network access was further restricted using Linux Internet Protocol Tables (iptables) to allow only whitelisted hospital IP addresses and block unauthorized external connections.
The Front-End Layer was implemented as a responsive web interface and mobile application, allowing users to operate the system on both desktop and mobile devices. Role-based user interfaces were designed to simplify workflows for clinicians and dental technicians. Users created electronic work orders, uploaded impression and instruction sheet images, tracked case progress, and managed dispatch, return, and closure tasks. The system consisted of five core modules: (1) Dispatch module for creating digital work orders and binding NFC tags; (2) return module for automatically notifying responsible clinicians of completed laboratory returns; (3) query module for filtering and tracking cases by date, site, status, or clinician; (4) closure module for resetting NFC tags after case completion to enable reuse; and (5) registration module allowing clinicians to link their LINE accounts for automated notification activation. The mobile interface extended accessibility, enabling users to review historical cases and real-time statuses anytime and anywhere. The workflow was fully digitized: clinicians and technicians uploaded scanned or photographed instruction sheets during the dispatch stage, and the system automatically linked documents to case records, replacing traditional paper forms and improving data accuracy and retrieval efficiency. The setup and digital workflow at clinical and laboratory sites are illustrated in Figure 3.
Clinic-side dispatch setup. A dental work order form and an NFC tag were placed together in a transparent transport pouch and positioned on an RFID reader pad for scanning, generating a time-stamped digital record for the transfer episode. Laboratory-side documentation setup. Completed dental casts were placed alongside a dental laboratory instruction form embedded with an NFC tag. An overhead document scanner was used to capture documentation images, which were linked to the corresponding transfer episode prior to return.

Scan-based workflow setup at the clinic and the dental laboratory.
User interface
The system implemented a stepwise workflow for documenting the dispatch and return of dental impressions. On the main interface, users selected the hospital site and workflow step, scanned the associated NFC tag, uploaded supporting documentation (e.g., scanned images of the impression and work order), and confirmed the transaction. After scanning, the interface generated a summary table displaying transfer records, including dispatch/return timestamps, procedure stages, operator identifiers, and institutional location data. A thumbnail of the uploaded documentation was displayed on the right-hand side of the interface, and users could open an enlarged view by double-clicking. All uploaded images were automatically stored in a secure cloud database, ensuring longitudinal traceability of each case. The system also provided query functions to filter records by operation type (dispatch or return), site, medical record number, date range, or case status (e.g., pending follow-up, closed).
In cases where errors were identified or data were incomplete, users retrieved and edited records through an integrated editing interface. Missing information such as dates, names, or supporting images, was amended and resubmitted. By entering the treating physician's staff ID, LINE-based automated notifications were enabled, allowing the system to send impression return alerts directly to the physician upon scan-in. As illustrated in Figure 4, users also exported completed case records as PDF files. These exported documents served as semi-formal medical documentation for record keeping and workflow traceability.
The main user interface of the dental impression system. Users selected the branch, scanned or captured dental impression data, uploaded documentation, and managed records using action buttons (Scan, Capture, Delete, Confirm). A real-time table displayed key tracking details, and a thumbnail of the uploaded image appears on the left for preview. b. Return page: Users tracked and confirmed returned detail impressions, including status, date, location, step, and receiver. c. Query page: Users searched and managed impression episodes. d. Edit page: Users selected the status link to edit or complete records. e. Closure Page: Users reviewed and modified key fields and exported records to complete case documentation.
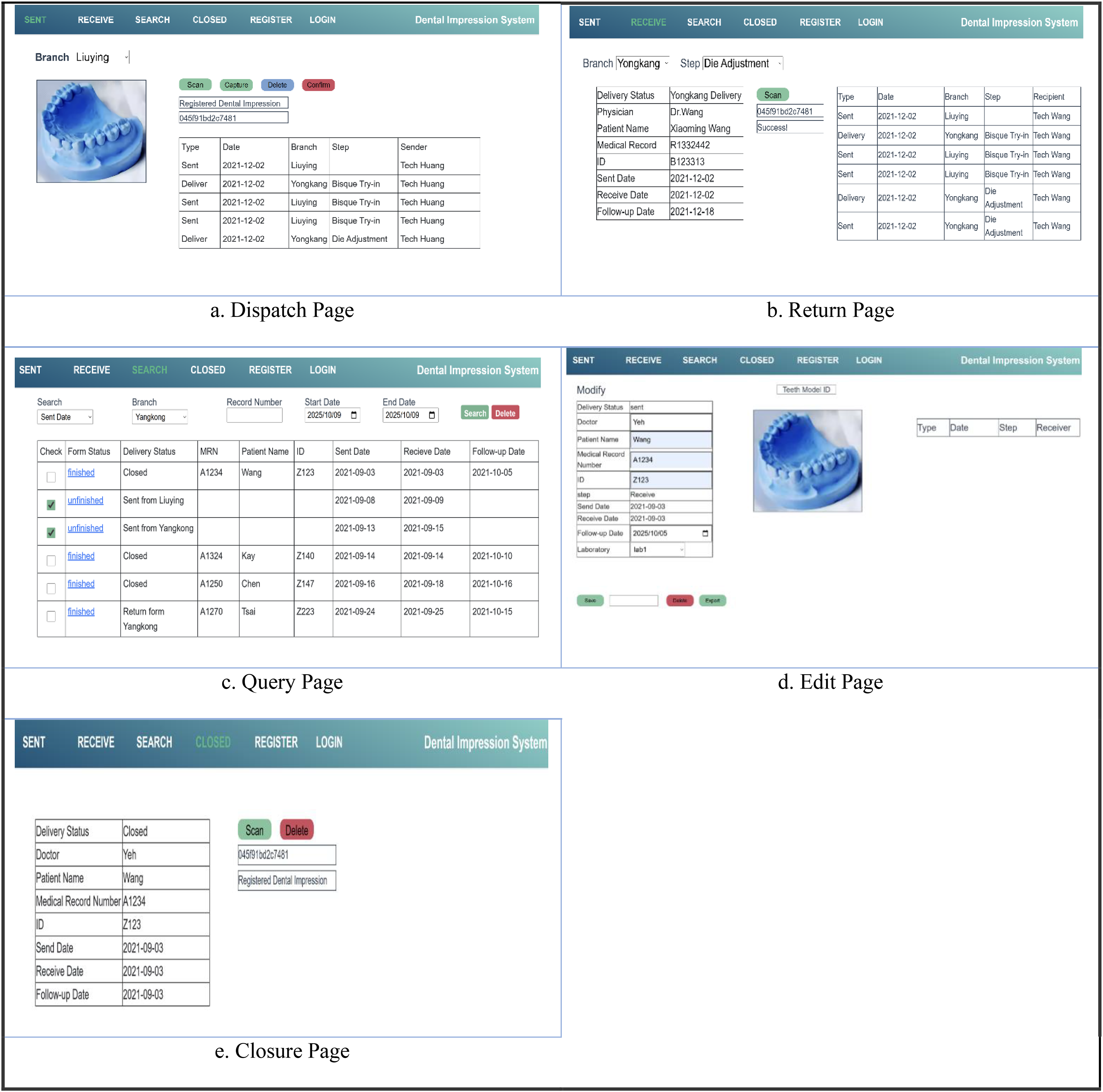
User interfaces of the prosthodontic workflow tracking system (PWTS).
LINE notify registration interface
To enhance real-time communication between clinical staff and the tracking system, a LINE Notify-based alert mechanism was integrated. Physicians completed the registration process by accessing the system via a secure URL and logging into their LINE account on a mobile device. Once registration was completed, the system associated each dental impression case with the registered physician. Upon scanning the returned impression, an automated LINE notification was triggered, providing relevant details such as the patient's name and the hospital site of arrival. This functionality supported prompt notification of case arrivals, even across geographically distributed facilities, as illustrated in Figure 5.
User authorization and subscription to LINE Notify for receiving system alerts. b. Physician registration interface used to link personnel information with the tracking system. c. Example of automated LINE notifications that were generated when a returned dental impression was scanned, showing key case information such as patient identifier and hospital site.

Line Notify registration and notification process
Phase 2 field validation
Study design
This study used a prospective field-validation design to examine clinic–dental laboratory transfer workflows across two branches of a medical center from May 2022 to September 2023. During routine operations, we evaluated transfer episodes managed under a PWTS-enabled digital workflow and those managed under the existing paper-based workflow. The study protocol was approved by the Institutional Review Board of Chi Mei Medical Center (IRB approval No. 11109-L01).
Episodes and sample size
The study consecutively recruited eligible clinic–laboratory transfer episodes during routine operations. Sample size was determined by real-world case volume over the study period rather than by an a priori power calculation. Episodes from both medical center branches were included, and case handling followed either the paper-based workflow (control) or the PWTS workflow (digital tracking), according to routine staffing arrangements. To reduce workflow overlap, each workflow was supported by a dedicated team (two dentists and one dental technician), consistent with usual practice. Work items involved in each transfer episode included clinic-to-laboratory dispatch of impressions/records and laboratory-to-clinic return of outputs (e.g., working models and/or prostheses). Inclusion criteria were: (1) fixed prosthodontic cases requiring clinic–laboratory transfer; (2) a documented scheduled due date aligned with the planned follow-up visit; and (3) sufficient records to evaluate timeliness. Exclusion criteria were: (1) missing scheduled due dates; (2) cancellation before completion; and (3) incomplete records precluding delay assessment.
Outcomes
Two primary outcomes were evaluated. Delay incidence was defined per episode: an episode was classified as delayed if the completion/closure date occurred after the scheduled due date. Delay incidence was calculated as delayed episodes divided by total episodes and reported as a percentage. Delay burden was calculated as delayed days per episode: for delayed episodes, delayed days equaled the calendar-day difference between the completion/closure date and the scheduled due date; for non-delayed episodes, delayed days were set to 0. Delayed days were summarized across episodes (e.g., total and per-episode distribution) and compared between workflows. In addition, user-reported experience measures were collected only in the PWTS group after implementation using a brief questionnaire with 5-point Likert scales assessing perceived benefit, overall satisfaction, continued-use intention, and perceived ease of tracking transfer status across handoffs.
Statistical analysis
We summarized outcomes using descriptive statistics. Between-group comparisons were performed for delay incidence using the chi-square test and for delay burden using the Mann–Whitney U test due to non-normality. User-reported experience measures were collected in the PWTS group only and summarized descriptively using 5-point Likert scales.
Results
A clinical field validation was conducted between May 2022 and September 2023 at two branches of Chi Mei Medical Center. During the study period, all eligible prosthodontic transfer episodes requiring inter-unit transfer and meeting the predefined inclusion criteria were included, resulting in a total of 154 cases assigned to the PWTS group (n = 84) and the paper-based control group (n = 70).
In the PWTS group, 15 cases (17.9%) were delayed, with 262 cumulative delayed days. In the control group, 37 cases (52.9%) were delayed, with 408 cumulative delayed days. Delay incidence differed significantly between groups (χ2 = 19.38, p < 0.001). Mean delayed days per transfer episodes were 3.12 in the PWTS group and 5.83 in the control group (p < 0.001) (Table 1). In the control group, delays were most commonly observed in episodes involving coordination and documentation steps, including work items returned to clinicians without timely confirmation, misdelivery to an incorrect branch, and unclear or incomplete work-order instructions. In the PWTS group, delayed episodes were uncommon and mainly reflected identifiable operational exceptions, including misdelivery to an incorrect branch and instances in which the responsible operator was not on duty on the scheduled day.
Delay outcomes between PWTS and paper-based workflows.

User-reported experience in the PWTS group after implementation showed a mean score of 2.5 for ease of tracking transfer status across handoffs. Higher mean scores were reported for workflow-related items, including improved production flow (4.0), reduced delivery delays (4.0), ease of completing daily tasks (4.5), alignment with practical needs (4.5), and facilitated record review (4.0). Overall satisfaction and continued-use intention were both 3.5. In addition, implementation of the scan-based workflow was associated with an estimated reduction of approximately 30 staff-hours per month in administrative workload (Table 2).
User-reported usability and workflow support following PWTS implementation.

Discussion
The present findings showed a significant difference in transfer timeliness between workflows managed with PWTS and those managed with a conventional paper-based process. Delay incidence was lower in the PWTS group (17.9%) than in the paper-based workflow (52.9%), with fewer delayed days per case (3.12 vs 5.83). Within the evaluated setting, these results describe process-level differences in clinic–laboratory transfer timeliness under a scan-based workflow with time-stamped checkpoints.
Multiple workflow-level factors may contribute to these differences. In paper-based workflows, progress and coordination typically rely on manual documentation, phone calls, and individuals’ awareness of case status, which may increase variability when information is incomplete or when completion is not promptly recognized. By contrast, PWTS records predefined checkpoint events via scans and synchronizes time-stamped statuses to a dashboard, which may reduce ambiguity regarding whether a transfer has occurred and when it occurred. Importantly, PWTS was implemented to document and visualize workflow events rather than to modify clinical decisions or laboratory fabrication procedures.
These observations are consistent with prior work indicating that information technology systems can support clinic–laboratory communication by improving the completeness, organization, and retention of case-related information. 12 In this context, PWTS provides a mechanism for time-stamped event capture and workflow visibility to support status awareness and coordination across clinic–laboratory transfers.
Post-implementation user-reported experience showed generally favorable ratings across several workflow-related domains, particularly items related to practical fit and support for daily work, while overall satisfaction and intention to continue use were moderate. By contrast, ease of tracking transfer status across handoffs was rated lower, indicating a usability and information-presentation gap that warrants attention. This pattern can be discussed in relation to technology acceptance literature. Studies grounded in the Technology Acceptance Model (TAM) indicate that perceived ease of use and perceived usefulness are positively associated with intention to use, and may mediate the relationship between system characteristics and use intention. 30 Prior work also links user-friendly interfaces with greater adoption or continued-use intention, and suggests that systems perceived as understandable, user-friendly, and valuable may progressively motivate users to adopt and accept new technologies. 31 In this context, the lower rating for cross-handoff status tracking suggests that refinement efforts may focus on clearer dashboard information hierarchy and status visibility, more explicit handoff or branch-level signaling, and more intuitive search and notification flows to improve perceived usability in routine workflow use. PWTS implementation was also accompanied by a reduction in administrative workload in the evaluated setting. Further multicenter evaluations using standardized usability measures and broader outcome indicators, with longer follow-up, would help to examine generalizability and longer-term implementation performance.
Several limitations should be noted. First, the study was performed at two branches of a single medical center, which may limit the generalizability of findings to institutions. Future research could expand to multicenter settings. Second, user-reported experience measures were collected only in the PWTS group and only after system implementation. Future work may incorporate theoretical models such as the Technology Acceptance Model (TAM)32,33or System Usability Scale (SUS)34,35 to assess usability and adoption. Finally, PWTS tracked transfer events and linked documentation but did not capture detailed clinical decision-making processes or prosthodontic treatment outcomes. Future studies could extend the system to integrate selected clinical data elements or outcome indicators, enabling concurrent examination of workflow processes and downstream clinical outcomes.
Conclusion
This study recorded lower delay incidence and delay burden in PWTS-managed episodes than in a paper-based workflow within the evaluated setting. PWTS captures time-stamped checkpoint events and provides workflow visualization for real-time status display and operational monitoring in prosthodontic clinic–laboratory transfers. User-reported experience ratings indicated favorable perceptions for selected system functions and identified priorities for usability refinement. Further multicenter evaluations using standardized usability measures and broader outcome indicators are needed to examine generalizability and longer-term implementation performance. 36
Footnotes
Acknowledgments
The authors would like to thank Jia-Yu Yang for administrative support and Chi-Mei Medical Center for their assistance and support throughout the study.
ORCID iDs
Ethical considerations
This study was reviewed and approved by the Institutional Review Board of Chi Mei Medical Center, IRB Serial No. 11109-L01.
Authors’ contributions
Y.H. Tsai drafted the initial manuscript. T.C. Kuo and C.L. Chiou contributed to system development and data analysis. S.Y. Ye, W.F. Chiang, and Y.F. Huang coordinated clinical data collection and validation. C.H. Chuang conceptualized the study and supervised the entire research process. All authors reviewed the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by Chi Mei hospital, Liouying, Taiwan under grant numbers CLFHR11008 and CLFHR11124, covering a two-year funding period.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Guarantor
Cheng-Hsin Chuang