
Abstract
Background
Global population ageing has heightened mental health concerns among older adults. Traditional reminiscence therapy (RT) is effective but faces limitations in accessibility and scalability due to its reliance on clinical settings and professional guidance. Digital technologies, including multimedia platforms, virtual reality, and social robots, offer promising alternatives. The purpose of this study is to explore the perceptions, attitudes, needs, and concerns of older adults and healthcare providers regarding digital reminiscence technology.
Methods
A qualitative descriptive design was used, employing focus groups with 14 older adults from communities and nursing homes, and 10 healthcare providers from a tertiary hospital. Four focus groups were conducted between November and December 2024, following demonstrations of digital tools. Data were analyzed using conventional content analysis with NVivo 12.
Results
The analysis revealed three major categories: Integration of reminiscence and digital tools; Enhancing accessibility and usability; Ethical and social considerations in digital reminiscence.
Conclusion
Digital technologies can enrich RT by improving immersion and scalability, but challenges like affordability, usability, and ethical risks must be addressed. Findings from both older adults and healthcare providers in the Chinese cultural context highlight the need for affordable, simple, culturally sensitive, and ethically robust digital solutions, suggest that tailored strategies should be developed for family, community, and clinical settings to support the wellbeing of older adults.
Introduction
Global population ageing has intensified concerns about mental health challenges among older adults, including cognitive decline, depression, and loneliness, which substantial burdens on individuals and society. 1 Reminiscence as a psychological process enabling individuals to reexamine life experiences for meaning and value. 2 Reminiscence therapy (RT), grounded in Erikson's theory of achieving ego integrity through life review, 3 involves the structured recall of past experiences using photographs, objects, or narratives guided by professionals. 4 Evidence supports its efficacy in reducing depression and enhancing self-esteem, and quality of life.5–7 However, traditional RT has notable limitations: it is often confined to clinical settings such as hospitals or nursing homes, restricting accessibility, 8 and its dependence on trained therapists hinders scalability, particularly in resource-limited regions. 9
Emerging digital technologies offer innovative solutions to these constraints. Digital reminiscence platforms enable users to engage autonomously with their life narratives through multimedia,10–12 while gamified interventions integrate reminiscence into interactive experiences. 13 AI-driven social robots can simulate conversational reminiscence partners, accompanying older adults in recalling the past. 14 Virtual reality (VR), RT has demonstrated high feasibility in dementia care, significantly reducing behavioral and psychological symptoms (e.g. agitation, anxiety, and apathy) by recreating natural environments or nostalgic scenes to evoke positive emotions and enhance feelings of fulfillment and security. 15 These technologies also facilitate therapist monitoring of psychological states for personalized interventions, for instance, through real-time physiological sensors in VR systems (e.g. heart rate monitors, skin conductance sensors) or algorithms analyzing behavioral data (e.g. facial expression recognition, voice tone analysis, and eye-tracking) to track emotional indicators such as anxiety levels, mood fluctuations, or attention focus, thereby identifying potential negative responses or signs of cognitive improvement.16,17 Such innovations overcome the spatial and professional limitations of traditional RT by reducing the need for real-time therapists and improving scalability in areas with limited professional resources.
Despite these technological advancements, adoption barriers persist. Older adults show increasing interest in digital technologies but face challenges, including age-related cognitive changes (e.g. slower processing speed, reduced attention, and difficulties with multitasking), digital divides (e.g. accessibility, literacy, and anxiety), and personal factors (e.g. motivation and health status).18,19 Furthermore, due to unfamiliarity with new technologies, 20 older adults generally exhibit lower acceptance and adaptability to new technologies 21 ; factors such as interface design and privacy concerns also affect acceptance.22,23 Although digital interventions can promote engagement and provide cognitive stimulation, they may also cause physical discomfort (e.g. eye strain) and trigger negative emotional reactions, such as frustration due to operational difficulties.24,25 These potential risks have been documented in digital health research and should be considered when developing digital reminiscence technologies.
Existing studies mainly evaluate specific digital products such as VR systems or individual reminiscence apps, rather than examining older adults’ overall perspectives on the broader landscape of digital technologies used for reminiscence. Although RT primarily targets older adults, perspectives from healthcare providers can offer valuable insights into intervention feasibility, clinical safety, and operational processes in care settings. Frontline healthcare providers frequently observe older adults’ needs for emotional support, cognitive stimulation, and social interaction in daily practice. They possess practical experience in integrating reminiscence activities into care plans and mitigating potential risks. 26 This ensures that designed digital or traditional RTs not only align with older adults’ subjective needs but also guarantee clinical feasibility and safety.
The specific research questions guiding this study were:
The present qualitative study explored the perceptions, needs, and concerns of older adults and healthcare providers regarding digital RT. A summary of diverse implementation suggestions for digital technologies across various settings will inform the design optimizations and strategies for future digital RTs.
Methods
Design
A qualitative descriptive design was employed to provide a straightforward description of participants’ perspectives on digital reminiscence technology and to elicit their needs and attitudes. 27 This approach is grounded in naturalism, with findings that entail a low degree of interpretation. The study's methodology is based on conventional content analysis for data analysis, which aligns with the qualitative descriptive paradigm by emphasizing inductive, semantic-level analysis. 28 Focus groups were selected as the data collection method because interaction can produce a “chain” effect, where the speech of one participant stimulates the ideas and memories of others, thereby enriching the discussion content. 29 The focus group approach allowed for a more comprehensive discussion of participants’ views on digital reminiscence technology. The study adhered to the Standards for Reporting Qualitative Research. 30
Participants
This study employed purposive sampling to select participants, ensuring they had relevant experience to provide insights.
Inclusion criteria for older adult participants were: (1) age ≥60 years; (2) experience in participating in simple reminiscence or life-review therapies, to ensure they could form opinions on digital reminiscence technology based on personal experiences. Exclusion criteria were: (1) current participation in other clinical studies or psychological intervention programs; (2) severe dementia or psychiatric disorders that would prevent normal communication.
Inclusion criteria for healthcare providers were: (1) at least five years of clinical experience in hospital inpatient wards (e.g. geriatrics) including physicians, nurses, therapists to ensure they could understand the real experiences, emotional needs, and practical challenges of older patients in geriatric care; (2) experience in clinical application, learning, or exposure to digital health technologies (e.g. computer-based cognitive interventions); (3) previously studied, participated in, or implemented RT. Exclusion criteria were: practitioners whose clinical medical or nursing work did not involve older populations (e.g. pediatricians).
Sample and setting
This study's focus groups included a total of 24 participants, comprising 14 older adult participants and 10 healthcare providers. Among the 14 older adult participants, seven were from community service centers and seven from nursing homes, all located in urban areas. Older adults were assessed as cognitively healthy via MMSE (scores ≥24), with normal functional levels and local Chinese-speaking cultural backgrounds. The older adult focus groups were conducted in the nursing homes and community service centers, respectively, in environments familiar to the participants to reduce discomfort.
The 10 healthcare providers included four physicians, five nurses, and one physical therapist, all from the same local largest tertiary hospital (approximately 5000 beds), affiliated with the geriatrics, neurology, and cardiology inpatient departments in care settings. Although the providers were from the same hospital, the distribution across different departments facilitated the collection of diverse perspectives, supporting research data diversity (e.g. neurology provided insights on cognition, cardiology on emotional support). The healthcare provider focus groups were conducted in hospital meeting rooms. Detailed background information on participants is provided in Appendix 1.
Two focus groups were conducted for older adults and two for healthcare providers, totaling four sessions. Each focus group consisted of 5–7 participants and was moderated by the first author (a male PhD in nursing). The research team also included holders of PhD and master's degrees in nursing, responsible for assisting with recording and observation. All researchers completed four hours of specialized training provided by an experienced qualitative researcher prior to the start of the study. Training covered focus group moderation skills, ethical principles, and management of researcher bias. Team members had prior practice and research experience in RT. The study was conducted from 28 November to 25 December 2024.
Procedure
Recruitment was conducted by an independent research assistant who explained the study purpose, procedures, informed consent process, and requirement to complete a brief demographic questionnaire. Participants provided verbal consent and then signed written informed consent forms. Data saturation was considered throughout the study using a dynamic assessment strategy.31,32 After each session was transcribed the research team met to discuss the data and decide whether additional groups were necessary.
Before each focus group, the moderator introduced a range of digital reminiscence technologies and devices using neutral language and tone. Demonstrations included VR equipment, social robots, digital photo albums, dedicated RT applications and websites. The potential benefits and current limitations of each technology were described and clarifying questions were posed to ensure that both older adults and health care providers had sufficient understanding. The introduction followed a fixed procedure and script to ensure all groups received consistent information.
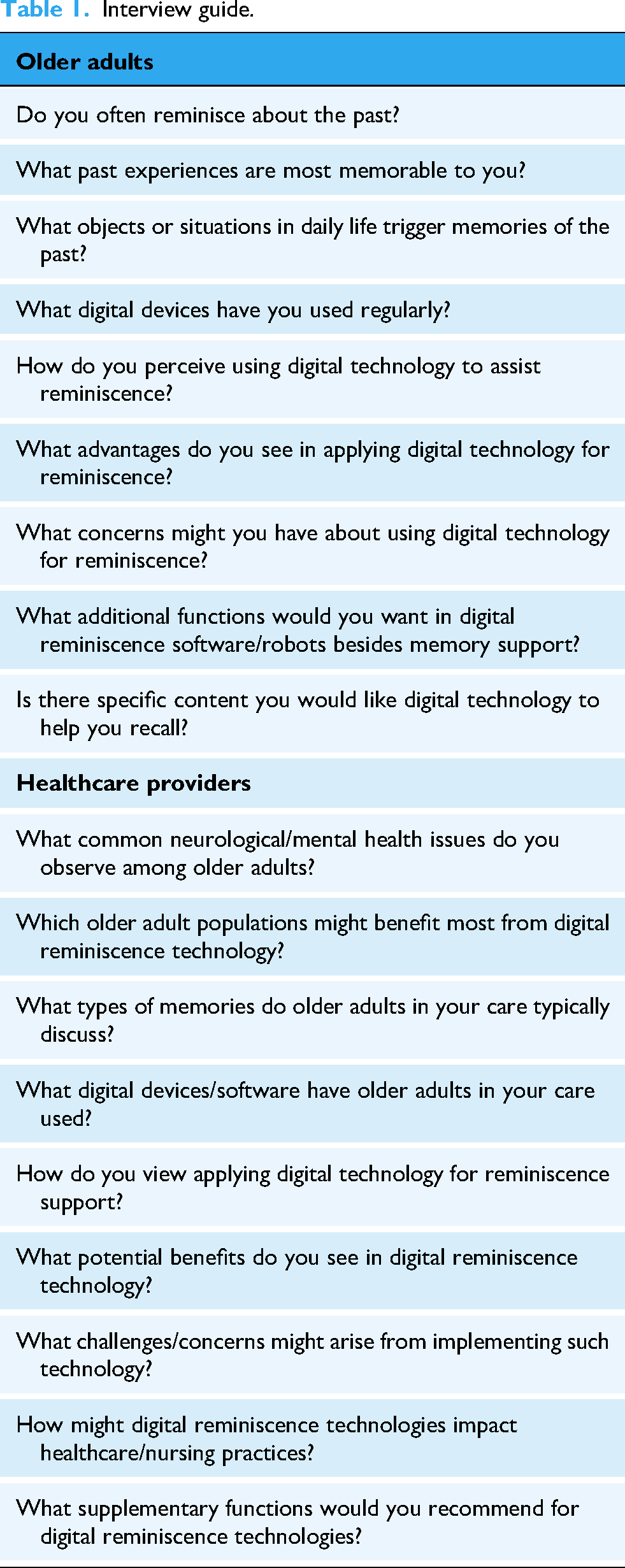
The research team developed a semistructured interview guide focusing on comprehension, willingness to use, concerns, and suggestions regarding digital reminiscence technology. A structured topic guide was prepared to facilitate discussion and to outline core areas while allowing the group to move beyond preset questions and engage in open exploration. Group rules were established including turn taking to ensure equal opportunity to speak and moderator use of neutral prompts to encourage expression of negative views. Two pilot interviews with community-dwelling older adults were conducted and feedback was used to refine the topic guide for clarity. The focus group topic framework is shown in Table 1.
Interview guide.
Each focus group lasted approximately 40–60 min and was audio recorded. Field notes were taken concurrently. To mitigate power imbalances older adults and health care providers were placed in separate groups. The first author allowed natural transitions between topics after participants completed discussion of a theme rather than directing the discussion. Participants were encouraged to express views and reminded that participation was voluntary and that they could decline to respond or withdraw at any time without consequence. Seating arrangements dispersed older adult participants to reduce the risk of marginalizing any individual voice. Audio recordings were anonymized and encrypted for storage by the first author. Access to raw data was limited to the first author and two designated team members. Data were stored on a secure cloud server with password protected software and will be securely destroyed after five years.
Qualitative analysis
Data were analyzed using conventional content analysis method. The specific steps were as follows: (1) Within 24 h of each focus group, the first author and another team member completed verbatim transcription, which included nonverbal information for example participant’ actions and facial expressions. These elements were recorded in the interview record forms to assist coding for example a hesitating tone that suggested discomfort and to enhance contextual understanding of semantic codes. (2) All transcripts were read repeatedly by the coders to achieve immersion and obtain a sense of the whole. (3) Transcripts were then read word by word to derive initial codes, highlighting exact words or phrases that captured key thoughts or concepts. (4) NVivo 12 software was used for coding and category development. Coding was conducted independently by the first author (a PhD in nursing with three years of experience in geriatric medicine and digital reminiscence research) and an independent team member (a PhD in nursing with five years of related experience); both coders had received formal training in qualitative data analysis. (5) An inductive approach was employed to generate codes directly from the data, with analysis conducted at the semantic level to stay close to the original content. (6) The process of moving from codes to categories involved sorting codes into meaningful clusters based on their relationships and links, combining or subdividing codes as needed; definitions were developed for each category, subcategory, and code, ensuring they represented recurring patterns relevant to the research questions. (7) Discrepancies between coders were resolved through repeated discussions to reach consensus, and exemplars from the data were identified for each category. (8) To enhance credibility, reflexive memos were maintained during transcription and coding to document emotional responses and potential biases (e.g. when participants expressed concerns about technology, the researcher reflected on a personal preference for innovation and adjusted interpretations to prioritize participants’ voices); additional measures included negative case analysis and triangulation with field notes.
Ethical approval and consent
The study was approved by the Ethics Institutional Review Board of the School of Nursing, Jilin University (Approval No. 2024112025). The date of approval of the ethics application was 20 November 2024. It was registered with the Chinese Clinical Trial Center (Reg No. ChiCTR2500106840). Researchers informed participants of the research objectives, interview process, and privacy protection measures, and all participants signed informed consent forms. Participants could withdraw from the study at any time, and all personal information and interview content were kept strictly confidential, stored only on the first author's computer and used solely for research purposes.
Results
Participant demographics
The study recruited 24 participants, including 14 older adult participants and 10 healthcare providers. Among the older adult participants, the mean age was 65.9 ± 3.2 years, with eight men and six women. For education levels, one had primary education, seven had secondary education, and six had bachelor's degrees. Healthcare providers had a mean age of 36.6 ± 4.7 years and average work experience of 10.1 ± 5.4 years, with three men and seven women. Professional categories included four doctors/chief physicians, four nurses/head nurses, and one therapist. Regarding education levels, three had bachelor's degrees and seven had postgraduate degrees. See Table 2 for details.
Demographic characteristics of study participants.

Content analysis
The content analysis identified three main categories, each with 2–3 subcategories, see Figure 1 for details. Each quotation is followed by the person who made the point, A for older adult participants and B for healthcare providers.

Perspectives of older adults and healthcare providers on digital technology for reminiscence.
Integration of reminiscence and digital tools
Older adult participants and healthcare providers summarized a complex interplay between their attachment to the past and their adaptation to modern digital technologies. This category, “Integration of reminiscence and digital tools” is divided into two subcategories: “Reminiscence as emotional anchor” and “Digital tools as interaction facilitators.”
Reminiscence as emotional anchor
For older adult participants, memories transcend simple recollection, acting as a profound emotional lifeline that ties them to their sense of self and community. One participant vividly captured this sentiment: “Back then, social order was better, relationships between people were harmonious; it was an era of mutual help” (A12).
Another participant shared a cherished memory: “What I loved most about childhood was the New Year, when we could eat candy and good food, and have new clothes to wear. During New Year, parents would bring out treats to share with everyone” (A2).
However, the past is not always a sanctuary. As one participant observed: “But when you talk about remembering, it's inevitable to recall sad things. Life was poor then, not knowing if there would be food for the next meal” (A8). The emotional weight of these recollections underscores their role as both a refuge and a mirror to lived experiences.
Digital tools as interaction facilitators
Digital technologies captivated participants with their ability to transform reminiscence into a dynamic, sensory-rich experience, forging an emotional link to bygone days. Far from static aids, technologies like photo archives and video simulations elicited wonder and connection. One participant exclaimed:
“Now with these new technologies, we can put together photos from youth, and if it simulates the scenes from back then, it feels like returning to the past; it is remarkable” (A5).
A healthcare provider elaborated on its potential: “Previously, reminiscence might just be chatting between people, but now with music, pictures, videos, this kind of multi-sensory stimulation might have unique effects for the older adult participants” (B22).
Yet, not all reactions were unequivocally positive. One participant expressed unease: “Machines don’t have expressions … humans have expressions, they’re not cold machines; I don’t like communicating with machines because they lack human touch” (A7).
Enhancing accessibility and usability
A strong desire for digital reminiscence tools that are both accessible and practical wove through participants’ narratives, reflecting their vision for technology that fits seamlessly into daily life. This category, “Enhancing Accessibility and Usability,” highlights the barriers and aspirations tied to adopting such innovations.
Technological accessibility barriers
The promise of digital technologies often clashed with practical realities, as participants pinpointed multiple obstacles to their use. Cost identified as a formidable hurdle, with one older adult participant noting:
“Buying a VR device or robot is too expensive; we can’t afford it. We might only use it if it's a free app” (A11).
This financial constraint suggests that without affordable options, such as low-cost or subsidized applications, many older adult participants may be excluded from technological benefits. Another participant stressed simplicity:
“This robot or app should only need one button press to start conversation; otherwise, we can’t learn all those other things” (A14).
A clinical nurse reinforced this perspective: “Many older adult patients in our wards only know how to use basic phones, not smartphones. I think the operation needs to be simple, without complex procedures” (B21).
Immersive reminiscence experience
Older adult participants described how technology-enhanced reminiscence provided a more engaging and vivid way to relive past memories, transforming traditional conversations into multisensory interactions. One participant highlighted the companion-like nature of robotic tools:
“This little robot is quite fun, just like a child accompanying us to chat, and it can talk about past things, and it won’t get impatient” (A9).
Another participant enhancements: “Before, chatting just relied on thinking, it was all fuzzy. Now with this (technology), the scenes and sounds are right in front of you, it's simply like living it all over again” (A12).
A healthcare provider further elaborated on the multisensory aspects: “The great thing about this immersive experience is that it's not a single stimulus; it's sounds and visuals together, fully activating the participant's senses and memories in all directions. The effect is indeed much stronger than just chatting with words” (B19).
Practical functional needs
Participants envisioned digital technologies that extend beyond reminiscence to address everyday needs, particularly in health and independence. This subcategory underscores the value of functionality in making technology indispensable. A healthcare provider emphasized a key feature:
“Medication reminders, this is the most needed function clinically. It's about reminding older adults when it's time to take their medicine” (B23). Another participant highlighted broader applications:
“I think we can focus on health education. For instance, how to prevent hypertension? Prevent cerebrovascular diseases, these chronic diseases and others; these are very important for the older adults” (B22).
Integrating educational content could empower older adult participants to take proactive steps in their care.
Ethical and social considerations in digital reminiscence
As digital technologies infiltrate reminiscence practices, ethical and social implications loomed large in participants’ discussions. This category probes these complexities, encompassing three subcategories: “Ethical and Privacy Concerns,” “Technology Dependence and Side Effects,” and “Human-Machine Interaction and Humanized Care.”
Ethical and privacy concerns
Safeguarding privacy and ensuring ethical use identified as paramount concerns, shaping participants’ trust in digital reminiscence technologies. One participant voiced a common apprehension:
“Whether this digital product involves cybersecurity issues needs careful consideration, after all, it involves older adult personal information and privacy” (B18). This worry reflects the vulnerability of sharing personal histories in a digital space, where breaches could erode confidence.
“Many of us are afraid to use new electronic products, one reason being fear of fraud” (A6). This fear of exploitation ties ethical concerns to broader social dynamics, such as trust in institutions offering these technologies.
Technology dependence and side effects
Concerns about overreliance on technology sparked debate, with participants weighing its benefits against potential drawbacks. A healthcare provider pondered cognitive risks:
“Using such digital technology, especially highly intelligent AI, helps people think. But over time, won’t people's own brains deteriorate? I feel myself getting lazy about thinking after using TikTok too much” (A3).
Emotional risks also surfaced: “AI is a very powerful technology, possibly better than ordinary programs or software for helping older adult participants reminisce, but might it make older adult participants become too obsessed with the past?” (B17). Such fixation could distance users from present realities, impacting social engagement.
Human–machine interaction and humanized care
The interplay between technology and human connection summarized a deep-seated need to preserve empathy in care. One participant articulated this tension:
“We don’t want to trouble our families or you. At this old age, people fear becoming family burdens most” (A10). This preference for human warmth underscores technology's limitations in replicating emotional nuance.
A nurse offered a view: “From a nurse's perspective, I’ve found in my daily work that older adults who are discriminated against, neglected by their children, disabled, or physically restricted need digital technology more to help them reminisce” (B23).
These perspectives highlight the importance of designing technologies that enhance, rather than replace, humanized care, ensuring older adult participants receive both technical support and emotional resonance.
Discussion
This study provides an integrated understanding of how older adults and healthcare providers perceive the use of digital technologies in RT. First, reminiscence remains an emotionally significant activity for older adults, characterized by both nostalgic comfort and potentially distressing memories. Second, participants valued digital technologies for their immersive and multisensory features, yet raised concerns about affordability, usability, privacy, and potential overreliance. Third, perspectives from healthcare providers complemented those of older adults by highlighting clinical feasibility, safety, and workflow-related considerations. Together, these findings illustrate the practical, emotional, and ethical complexity of digitizing RT.
Central to older adult participants’ narratives was balancing past and present experiences. They recalled childhood celebrations, traditional festivals, and strong social bonds—memories that often served as an emotional anchor for mood and mental well-being. Existing research supports the alleviation of loneliness and depressive moods. 33 Such memories could, however, evoke distress when related to difficult life periods, highlighting the need for careful facilitation. 34 Older adults often feel ambivalence, seeking emotional comfort from positive memories but fearing negative triggers.35,36 Digital technologies should thus include emotional regulation features, like prompts for positive recollections or personalized filters, to establish effective mechanisms.
Compared to traditional interpersonal reminiscence, digital tools preserve more materials and create immersive, multisensory experiences via photo archives and VR simulations, enhancing engagement. 37 Multimedia integration and scenario recreation can create more engaging reminiscence experiences,38,39 and VR-based therapy reduces apathy in aged care. 40 Furthermore, AI integration enables personalized interactions, easing caregiver burdens and supporting scalable alternatives. 41 However, participants noted machines’ “cold” nature, stressing that digital tech should supplement, not replace human warmth to preserve interpersonal connections.
Digital reminiscence technologies face barriers like financial costs, operational complexity, and digital literacy gaps, with older adult participants advocating for affordable, one-button interfaces. 20 Echoing prior research, these include pricing, usability, privacy/security risks, and health impacts, creating multilayered accessibility issues.41,42 Older adult participants expressed concerns about privacy and cybersecurity, particularly regarding personal memories stored on digital platforms. Healthcare providers emphasized the need for intuitive interfaces and practical functions in clinical and daily life (e.g. medication reminders and health education), indicating substantial room for optimization in the field of digital health.
Healthcare providers raised concerns that excessive reliance on digital technologies may impair cognitive function or foster fixation on the past, also posing significant challenges to older adults’ physical health, such as vision strain. During the focus group discussions, potential risks brought by digital technologies were highlighted, along with the impact of the AI era on humanity—these concerns extend to broader questions about the impact of emerging technologies on human relationships. 43 Participants emphasized that human-machine interaction should preserve empathy and human-centered care. Participants valued human warmth over technological interfaces. Balancing technological innovation with human subjectivity remains a key challenge in digital RT.
This study provides information based on the perspective of Chinese culture, older adults repeatedly referred to collective memories of communal life, traditional festivals, and intergenerational roles, reflecting the importance of shared cultural narratives in shaping reminiscence content. Furthermore, participants’ fear of online fraud, reluctance to trouble family members, and preference for interpersonal warmth are consistent with findings from studies showing that digital engagement among Chinese older adults is strongly influenced by concerns about trustworthiness and family support. 44 These culturally grounded attitudes suggest that digital reminiscence tools designed for this population must incorporate culturally meaningful media, transparent privacy safeguards, and options that involve family members in co-creating or supervising digital reminiscence content. 45
An important contribution of the present study is its integration of perspectives from both older adults and healthcare providers, yielding a more nuanced understanding of barriers to digital RT implementation. Older adult participants prioritized emotional resonance, interface simplicity, and preservation of human companionship, whereas healthcare providers emphasized clinical safety, functional utility (e.g. integration of medication reminders and health monitoring), and seamless incorporation into existing workflows. This dual viewpoint revealed a broader spectrum of design requirements than previously documented in studies focusing on a single stakeholder group.
In light of these findings, we propose the following tailored implementation strategies: (1) In home environments, prioritize low-cost smartphone apps or voice-activated chatbots, 46 which enable autonomous use, personalize reminiscence content, involve family members, and reduce caregiver burden while addressing social isolation. (2) In community centers or nursing homes, deploy reusable intelligent VR devices if costs allow, 47 as staff guidance enhances immersion, fosters social interactions, and builds digital confidence among older adults. (3) In clinical settings, 26 integrate digital platforms that retain partial patient data to align with needs, easing provider workloads; use them as supplementary tools to extract reminiscence preferences, build rapport, and facilitate discussions. Both older adult participants and providers preferred accessible options like free apps and simple chatbots over complex technologies, though cost and usability challenges hinder widespread adoption, requiring industry-wide efforts.
Limitations
This study has several limitations. First, the research sample was primarily from urban areas, which may not fully reflect rural needs. Second, this study explores the overall perspectives and attitudes of older adults and healthcare providers toward digital reminiscence technology, participants may exhibit immediate reactions when presented with new digital technologies, which may not fully reflect their preexisting attitudes. Requiring healthcare providers to have at least five years of clinical experience excluded the perspectives of early-career professionals, which may limit the diversity of views on integrating new technologies into existing workflows. Future studies should include providers with varying levels of experience.
Conclusions
This study explores the perspectives of older adults and healthcare providers on digital reminiscence technologies and offers several implications. It emphasizes that digital technologies have the potential to enhance RT through immersive experiences and enriched content, while also presenting challenges such as high costs and operational complexity. This study summarizes diverse settings for applying digital technologies in different scenarios; future development should consider both diversity and practicality, developing user-friendly tools that accommodate older adults’ limitations.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076261426310 - Supplemental material for Perspectives of older adults and healthcare providers on digital technologies in reminiscence therapy: A qualitative study
Supplemental material, sj-docx-1-dhj-10.1177_20552076261426310 for Perspectives of older adults and healthcare providers on digital technologies in reminiscence therapy: A qualitative study by Haiqi Yang, Yongliang Jiao, Qiqing Zhong, Kexin Huang, Rendong He, Yong Jia and Li Chen in DIGITAL HEALTH
Supplemental Material
sj-pdf-2-dhj-10.1177_20552076261426310 - Supplemental material for Perspectives of older adults and healthcare providers on digital technologies in reminiscence therapy: A qualitative study
Supplemental material, sj-pdf-2-dhj-10.1177_20552076261426310 for Perspectives of older adults and healthcare providers on digital technologies in reminiscence therapy: A qualitative study by Haiqi Yang, Yongliang Jiao, Qiqing Zhong, Kexin Huang, Rendong He, Yong Jia and Li Chen in DIGITAL HEALTH
Footnotes
Ethical approval
The study was approved by the Ethics Institutional Review Board of the School of Nursing, Jilin University (Approval No. 2024112025).
Contributorship
Haiqi Yang: conceptualization, writing-original draft, formal analysis, data curation, and validation; Yongliang Jiao: writing-original draft, formal analysis, and data curation; Qiqing Zhong: writing-original draft; Kexin Huang: writing-original draft; Rendong He: formal analysis; Yong Jia: supervision, writing-review and editing; Li Chen: supervision, writing-review and editing. All authors reviewed the final draft, and were willing to take responsibility for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Jilin Provincial Department of Education Doctoral Student Research and Innovation Ability Enhancement Project (Grant No. JJKH20250228BS).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Clinical trial registration
China Clinical Trial Centre Registration No. ChiCTR2500106840.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.