
Abstract
Objective
This study aims to explore the experiences of older adults in nursing homes located in megacities of China regarding the use of digital health tools. By examining their perceptions, challenges, and benefits, the study seeks to provide insights into how digital health technologies can be effectively integrated into elderly care in urban settings, ultimately contributing to improved health outcomes and quality of life for this population.
Methods
This study followed the Consolidated Criteria for Reporting Qualitative Research guidelines. The current study utilized descriptive qualitative research methodology, adopting the technology acceptance model as the theoretical framework. Purposive sampling was used to recruit older adults from a number of care facilities in Hangzhou. Data were collected through semi-structured interviews and analyzed using directed content analysis.
Results
A total of 12 older adults in Hangzhou were interviewed for the study. Analyses yielded two themes and eight sub-themes: perceived usefulness (inclusiveness and participation, dynamic interaction and rapid feedback, accuracy and reliability of information, and early warning alerts), and perceived ease of use (technology self-efficacy, information security and privacy, bridging physical barriers, technical support and experience sharing).
Conclusion
Although older adults generally recognize the potential value of digital health tools in health management, they continue to face many challenges in practical application. This study provides empirical support for the promotion and application of digital health tools for older adults in megacities, which is important for promoting active policies toward aging.
Background
China's population aging has become a global concern. According to the seventh national population census bulletin published by the National Bureau of Statistics, as of 1 November 2020, China's older adult population aged 65 and above has reached 190 million, accounting for 13.50% of the total population, a proportion close to the standard of a deeply aging society. 1 Globally, increases in population aging have become an irreversible trend, with this phenomenon being particularly significant in megacities. 2
The term “megacity” typically refers to a city with a permanent population of 10 million or more within an urban area. 3 The economy of megacities is developed, there are many elderly care institutions, and there are many educated elderly people.4–6 Compared with other cities, megacities face a more complex situation in coping with the aging problem, which is not only reflected in the rapid growth in the proportion of older individuals within the population, but also includes a huge demand for medical resources and services for older adults.7,8 Although previous studies have investigated the use of digital health tools among older adults, their user experiences are still not well understood. This study explores how older adults in a megacity use technology to manage their health issues, shedding light on their experiences and practices.
According to recent studies, digital health tools primarily include (1) wearable and “Internet of Things (IoT)” devices that use sensor technology to collect data on vital signs and home environment9–11; (2) smart devices that provide online health services, support remote monitoring and counseling, and make emergency calls12,13; (3) smart care robotics for older adults14,15; and (4) mobile health applications and electronic health records.16,17 According to Galvez et al., 18 digital health tools have significant positive effects on enhancing quality of life and cognitive health in older adults. Specifically, remote monitoring and mobile health apps enable older users to effectively manage chronic diseases and enhance self-care skills. Nevertheless, full realization of the benefits of these tools is limited by the level of digital literacy of users. According to a randomized controlled trial conducted by Schneider et al., 19 although Baby Boomers, aged 50–65 years, are generally less digitally literate than Millennials, aged 18–35 years, their acceptance and willingness to use digital health tools is increasing. In addition, a study by Ienca et al. 20 showed that participants generally demonstrated positive acceptance of digital health tools and perceived the application of such tools to be of significant benefit in enhancing their overall well-being, especially those tools that are designed with a user-centered approach.
Based on the theory of reasoned action, the technology acceptance model (TAM) was developed in the field of computer technology. The TAM is widely used to explain and predict adoption behavior toward new technologies and has been extensively tested within older populations. 21 According to the theory, an individual's intention to use (acceptance of the technology) and use behavior (actual use of the technology) depends on the individual's perception of the usefulness and ease of use of a particular technology. 22 In simple terms, users are more likely to adopt novel technologies that exhibit high-quality user experience design, characterized by usability, usefulness, desirability, and trustworthiness. The TAM also suggests that perceptions of usefulness and perceived ease of use are moderated by external variables, including individual differences, system characteristics, social influences, and facilitating conditions. The principle of TAM is shown in Figure 1.
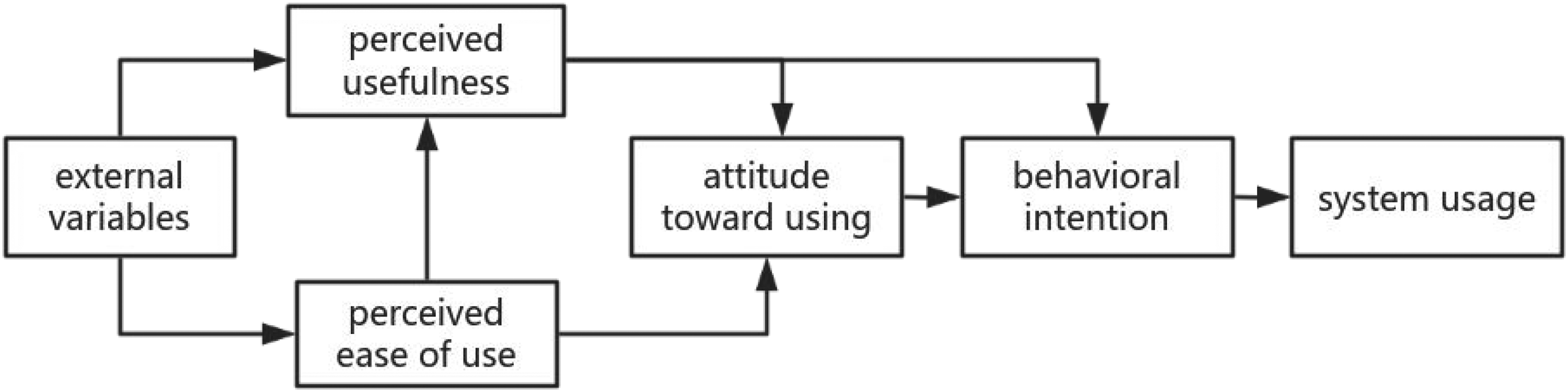
Technology acceptance model.
Materials and methods
The study followed the Consolidated Criteria for Reporting Qualitative Research guidelines. This study used a descriptive qualitative analysis design. The TAM was adopted as the theoretical framework, and directed content analysis was utilized as the research methodology in order to explore the experiences of older adults using digital health tools in a megacity retirement facility. Due process for this study was approved by the Academic Review Board of the first author's university (code: 20231117-11). Considering the focus on geriatric safety and practical usability in nursing homes, this study primarily investigated two categories of digital health tools: (1) smart devices and (2) mHealth apps. These tool types were selected based on their documented adoption in Chinese long-term care facilities, ensuring relevance to our nursing home context.
Participants
This study was conducted in Hangzhou from 20 November 2023 to 25 January 2024, using purposive sampling to recruit participants from a number of older adult care facilities in Hangzhou. Recruitment criteria were (1) 65 years of age and older; (2) long-term residence at the survey site for more than 6 months; (3) be willing to share the reasons and experiences for using or not using digital health tools; and (4) independent judgment and ability to communicate normally (except for those with severe mental and cognitive disorders). The number of participants was determined based on the criterion of reaching information saturation during the interview collection process. This basic research principle builds on previous qualitative research and it ensures the validity and reliability of the study. 23
Pre-data collection
A preliminary outline for the interviews was developed based on a systematic review of relevant research and an extensive discussion of the selected theoretical framework. To ensure both clinical and practical relevance, this outline was reviewed by a geriatrician and a digital health program manager. To pilot-test the tool, four participants took part in pre-interviews. During these sessions, we removed redundant questions and added new themes. Following the feedback from experts and the results of the pre-interviews, the outline was revised to better align with the study's objectives. By combining professional advice with practical experience, we aimed to make the current study more comprehensive and in-depth.
Data collection
Data were collected using face-to-face semi-structured interviews. In order to control the influence of cognitive bias of digital health tools on the experimental results, we explained the definition and types of digital health tools to each participant in the formal interview. The final interview outline included the following questions.
Have you ever used a digital health tool? How do you feel when using digital health tools? What difficulties or challenges have you encountered when using digital health tools? What positive or negative impacts do you think using digital health tools has had on your life? Do you share your experience of using digital health tools with people around you? What suggestions do you have for the improvement and development of digital health tools?
The interviews were conducted at locations that were convenient and private for participants by four female postgraduate nursing students (J.D., Y.R., J.X., and Q.H.) who had experience with studies using this descriptive qualitative approach. The locations of the interviews included restaurants, parks, and the rooms of the participants. The interviewer established a good relationship with the participants before starting the interview, and the respondents were fully informed of the purpose, methodology, and use of the study. All respondents volunteered to participate in the survey and signed a written informed consent form prior to their participation. No one else was present except the participants and the researchers. Respondents’ personal information was kept strictly confidential by replacing names with the letters A-R. Respondents had the right to withdraw from the study at any time without consequence.
The number of participants was determined once information saturation was reached during the interview process, which occurred when no new topics emerged and duplicate responses were noted. Saturation was inferred from the data of the tenth interview, with two additional interviews further confirming this finding. This approach aligns with fundamental research principles established in previous qualitative studies. 23 Each interview was audio-recorded to document the data, with careful attention paid to the interviewee's body language and facial expressions. The duration of each interview was approximately 30 min, ranging from 27 to 35 min, and field notes were taken immediately after each session.
Data analysis
Interview recordings were transcribed verbatim within 24 h after each interview, and the transcribed files were returned to participants for verification to ensure data accuracy. Since this study employed the TAM theoretical framework, the collected qualitative data was more structured. Therefore, the research team adopted directed content analysis to capture participants’ opinions and experiences. The entire data analysis process utilized de-identified text.
Firstly, four researchers (J.D., Y.R., J.X., and Q.H.) repeatedly read through the data to immerse themselves in the content and independently gained a comprehensive understanding of the participants’ interviews.
Secondly, the research team developed a coding manual based on the TAM theory, which included definitions and application criteria for key TAM constructs (e.g. user intention, use behavior, perceived usefulness, perceived ease of use), as well as a “not applicable” option to avoid forcing data into the theoretical framework.
Thirdly, the four team members independently coded all transcribed texts using NVivo14 software, with revisions to the coding manual made through team consensus when necessary. Any discrepancies or differences among the four coders were resolved through discussions and consultations with the expert (T.C.). Weekly meetings were held to discuss coding decisions and emerging themes, ensuring consensus on all interpretive differences.
Finally, supporting quotes were selected from the interviews. Data collection and analysis were conducted concurrently. Saturation was determined when the four coders observed repetitive participant responses and no new themes related to older adults in megacities’ experiences with digital health tools emerged. This procedure was guided by a female qualitative nursing expert with a PhD (T.C.), who is a university faculty member dedicated to geriatric nursing and qualitative research for many years. Chinese was the language used in the coding process. The coding and quotes in this report were subsequently translated into English.
Quality control methods
The interviewers comprised four female experienced master's students specializing in qualitative research, who had completed systematic training in qualitative methodologies and demonstrated advanced interviewing skills under the supervision of an associate professor proficient in qualitative research design. Researchers have a deep interest in qualitative research and the field of digital health and have accumulated certain experience. The researcher communicated with interviewees after each interview to confirm findings, reflected and summarized in a timely manner, and adjusted and improved the interview outline to ensure the accuracy and completeness of the data.
Results
A total of 12 respondents were recruited for this study, four males and eight females, ranging in age from 65 to 92 years. None of the participants left halfway and no repeated interviews were conducted in this study. Detailed demographic information is shown in Table 1. The analysis produced two themes and eight sub-themes, as shown in Table 2.
Demographic characteristics participants.

Themes and sub-themes of the study.

Perceived usefulness
The perceptions of older individuals regarding the usefulness of digital health tools were holistic evaluations that continue throughout the duration of tool use. They tended to assess whether specific digital health technology is able to fulfill the intended functions and outcomes and whether it matches their needs. If the use of the new technology can better meet their needs and provide more convenience and benefits than in the past, participants reported being more willing to accept and recognize the tool's usefulness.
Inclusiveness and participation
Respondent I: “I’ve only been to primary school and I don’t know a few words, typing is even more impossible, but even illiterate people like me can use it (laughs). This device has a voice command function, I just have to ask and I can know my health information so that even we illiterate people can enjoy the digitalization of our times.”
Respondent K: “I am now almost completely inseparable from my smart blood pressure monitor at home. I’ve had high blood pressure for years and I have to measure my blood pressure at least three times a day. I feel as if it was customized for me and has become completely involved in my daily life.”
Dynamic interaction and rapid feedback
Respondent A: “I sometimes contact a remote diagnosis service when I don’t feel well, and the doctors on it are all very professional. I can talk to the doctor directly on the platform via video screen, which saves time in traveling and waiting, and enables me to communicate with a doctor quickly (nods).”
Respondent C: “Once I felt I had a fever, I called the caregivers and they came right away to take my temperature, I remember it took less than three minutes (laughs). And now sometimes when it's quite cold outside and I’m too lazy to go out, I use this call host to talk to my old girlfriends, quite practical, otherwise, I’m too lonely alone.”
Accuracy and reliability of information
Respondent Q: “I’ve got a smartwatch that I bought actually to measure my blood sugar, and I thought it would be nice not to have to stick my finger in it. But you know, it's not accurate at all. Once I measured my blood glucose at the hospital and it was 11.1, but the watch only measured 5.2, which is not useful at all, so I don’t dare to trust it anymore.”
Respondent G: “Once, I saw an online platform that said older adults should eat fat-free food, which keeps our blood vessels cleaner. I thought this was right and was scared to eat anything with fat. Later, when I went to the hospital for a routine medical check-up, I consulted my doctor, who said that there was no need to pursue fat-free food specifically at all, but to choose healthy sources of fat, and that moderate fat intake was very important to the health of our senior citizens. Then I am now afraid to trust these health platforms completely, unlike what the doctor said.”
Early warning alerts
Respondent I: “I usually like outdoor sports, and once, probably because I was exercising too strenuously, my blood pressure and heart rate rose very high at once, and the bracelet alarmed me. Now I think it's lucky that I had my smart bracelet with me at that time, otherwise, I don’t know if I would have had an accident. I never paid attention to the intensity of exercise before, now I shift, we older people still have to exercise moderately, not too strenuous.”
Perceived ease of use
Older people's perception of the ease of use of technology is a key factor influencing their adoption of digital health tools. They assess whether using the tool is within their capabilities, whether they feel comfortable and confident in using it, and whether they need too much external guidance or assistance to determine whether they can easily interact with the tool to access health information.
Technological self-efficacy
Respondent F: “I’m not interested in using these ‘high techs’, my son bought them for me and taught me how to use them, but I just can’t learn them, and I’m a very slow learner at my age. Even if I can use it, I may not be able to read the data in it, it's all very specialized, and it's too difficult for me (shakes his head).”
Respondent D: “I'm illiterate – can't read or write at all, not even my own name. How could I possibly use those tech tools you're talking about? I can't even read a book!”
Information security and privacy
Respondent I: “Before using these tools, I was prompted as to what sensors, devices, or apps were being used to collect my health information, and sometimes I have been asked for advice on whether or not I would like my data to be anonymized and shared with research organizations for research purposes. I think these are still doing a pretty good job of making me feel like I have the right to decide and control my own data.”
Respondent E: “There are times when I’m a little bit worried that these health data are private to me and they might be compromised, and I generally don’t want people to know that I’ve had cancer, right, understandably. I’ve heard from my daughter that you can set up privacy security but it's too difficult for me to find out where it is, there's nothing I can do about it.”
Addressing physical barriers
Respondent G: “I think smart tools nowadays are very nifty and easy to use for us older people. For example, on the smart bracelet, the characters on the display were so small that I got dizzy, but then my son helped me to set the ‘care version’ and the font was enlarged, which made it much easier for us older people to use.”
Respondent C: “I am completely blind, but I can use some digital products to help me with my life and also to manage my physical health. Some of the devices have raised markings on the touch interface or I can operate them with some specific gestures, which is very thoughtful, and I feel that they [digital health tools] compensate to some extent for the visual impairment that we blind people have, and allow us to be more independent.”
Technical support and experience sharing
Respondent L: “I used to run into all sorts of problems when using smart technology, it was so difficult that I was going to give up and forget about it. But then a course was set up and a teacher was dedicated to teaching us, for example, how to use the health app on your phone, how to register on your phone if you are sick. That it's a lot easier to use when you have someone to guide you.”
Respondent R: “I wasn’t sure what functions my smartwatch had, so I would go on the forum or WeChat and ask people, and they would tell me how to use it, and I’m still interested now that I learnt that there are very many functions.”
Discussion
Perceived usefulness analysis
This study demonstrated that when older adults experienced the advantages of new technologies over traditional methods in meeting their health needs, their perceived usefulness of these tools significantly increased, which is consistent with findings reported a previous study by Yu et al. 24 It has also been argued that smart technologies are emerging as a new favorite among the individuals in the older population, thanks to their prospective role in health management.25,26 These technologies are not only able to provide early warning of potential health problems before they become apparent or worsen, but can also effectively prevent risky behaviors from occurring through real-time monitoring, which is in line with the views reported by some of the participants.27–29
It should be noted that this evaluation is not only influenced by the performance of the tools themselves, but is also closely related to the personal experiences of older adults. Individuals’ health status, education, digital literacy, and technological experience all influence their evaluation of these tools to some extent.30,31 In addition, the psychological expectations of older adults play an equally important role. A deeper understanding of the psychological expectations of older adults is essential to accurately capture their evaluation of the perceived usefulness of digital health tools.32,33 Older adults’ perceived usefulness of digital health tools is often based on trust in their functional accuracy and reliability. This trust can be easily undermined if they encounter problems with inaccurate data or poor operation during use. They may become frustrated by these negative experiences, lose confidence in the tool, and consequently reduce or stop using it, which is consistent with the findings of Portz et al. 34
As emphasized by the TAM model, perceived usefulness is the core driving factor for users to adopt new technologies. Our findings not only validate this theoretical premise but also extend its application to the domain of digital health tools for older adults. Therefore, in the process of designing and developing digital health tools, it is very important for developers to have a deep understanding and try to meet the actual needs of users. This means that the functional design of this tool should be closely centered on the health goals of users, effectively address the health issues of older adults, and provide effective health support. 20 Equally important is to embed mechanisms that address the psychosocial needs of older adults, such as promoting intergenerational connections through family-mediated interfaces. 35 These strategies go beyond the superficial usability features and address the systemic health barriers faced by older adults in an effort to win their trust and continue to use them. In addition to guiding the development of tools, this approach can also inform decision-makers and healthcare institutions to create scalable solutions, enhance health equity, and ultimately narrow the gap between technological innovation and its social realization. 36
Perceived ease of use analysis
Technology self-efficacy is both a driving force for older adults to experiment with digital health technologies and an important psychological basis for them to evaluate how easy these tools are to use, which is consistent with the findings of Golant et al. 25 When older adults believe they can effectively use digital health tools, they are more inclined to perceive them as easy to use and thus are more motivated to explore and utilize their features.
This study demonstrated that technical support and experience sharing among older adults significantly contributed to enhancing the perceived ease of use of digital health tools, a finding that fits with previous findings by Jokisch et al. 37 Additionally, experience sharing within the older adult community, such as exchanging usage tips and discussing common problems and coping strategies, builds informal knowledge-sharing platforms. Such platforms not only facilitate the rapid dissemination of technical knowledge, but also significantly increase older people's confidence in the ease of tool use. This interactive mechanism enables older adults to quickly adapt to new technology and reduces frustration due to unskilled operation, leading to more active participation in the practice of digital health management.38,39
Another study reported that older adults often face the dual challenges of operational difficulty and privacy protection when using digital health tools, which is in line with the views expressed by some of the respondents in the current study. 40 Older adults often feel apprehension that complex operational interfaces may lead to mis-touching, which will in turn trigger the disclosure of personal information, a concern that inadvertently reduces their perceived ease of tool use.
Although simplifying the user interface and optimizing the intuitiveness of operation remain the basis for improving the usability of digital health tools for old people, this study highlights the key interaction between usability and trust architecture. By combining the TAM, our research suggested that perceived usability goes beyond superficial interaction design—it requires embedding security mechanisms, such as end-to-end encryption and default privacy frameworks, as core usability features. In addition to technical specifications, this study is also conducive to promoting interdisciplinary collaboration among interaction designers, cyber-security experts, and gerontologists. By integrating expertise from multiple fields, we develop innovative solutions to jointly drive the optimization, upgrading, and wide application of digital health tools.41,42
Comparison of the use of digital health tools for older adults in megacities to small- and medium-sized cities
First, in terms of access to technology, megacities typically have more developed information infrastructures and richer digital resources, which provide older individuals with greater access to and use of digital health tools. However, this advantage does not mean that older individuals in megacities are necessarily better than their peers in small- and medium-sized cities in terms of technology acceptance. In fact, due to the faster pace of life and greater competitive pressures found in megacities, older adults may not have enough time and/or energy to learn and adapt to new technologies. 43
Second, differences in social support networks are also an important factor influencing older adults’ use of digital health tools. In small- and medium-sized cities, older adults tend to have stronger community ties and family support, which may compensate, to some extent, for their lack of technological resources. Whereas in megacities, although community services and older adult care may be more specialized, the detachment of social ties may lead to difficulties for older people in seeking help, which may hinder their exploration and use of digital health tools.38,43
Finally, differences in economic status may also have a significant impact on the adoption of digital health tools among older adults. Older adults in megacities may have higher socioeconomic status, and thus, may be able to afford more advanced digital health tools and services. 4 However, economic pressures may also drive them to pay more attention to the cost-effectiveness of tools, which may influence their choice of certain high-cost tools. In small- and medium-sized cities, although economic resources may be relatively limited, governments and communities may provide more subsidies and support, making it easier for older adults to access and use digital health tools. 5
Study limitations
This study has several limitations. First, the sample of this study may not have comprehensively covered all groups of older adults living in megacities, especially those living in the community, rather than older adult care institutions. This limitation may have affected the generalizability of the findings. Future studies should consider expanding the sample to include a more diverse group of older adults to gain a more comprehensive perspective. Second, due to the use of targeted content analysis in this study, the data collected were relatively limited; in addition, the sample size is relatively small, which may have led to limitations in the breadth of the findings. To address this limitation, a long-term follow-up and large sample size study should be conducted in the future, which would help to reveal the behavioral patterns of older people's continued use of digital health tools and the long-term impact of these tools on older people's health and quality of life. Third, while the semi-structured interview guide was refined through expert reviews and pilot-testing, it was not formally validated using standardized validation protocols. This limitation may affect the reproducibility of our findings in contexts beyond the current study. Future research should prioritize tool validation to ensure robustness across diverse populations.
Conclusion
The development and use of digital health tools has established an innovative connection between information technology and medical field, which has led to major changes in the health management of older adults. However, the widespread use of digital health tools among older adults in megacities still faces many challenges. In the future, the development of digital health tools and the research on the use experience of older adults should be promoted simultaneously to ensure the universality and applicability of the tools.
Footnotes
Acknowledgements
We appreciate the older adults who participated in this study.
Ethical considerations
Ethics approval was obtained from the Medical Ethics Committee of Zhejiang Chinese Medical University (code: 20231117-11). The authors confirmed that written informed consent was obtained from all the study participants before the interview. All methods were performed in accordance with the relevant guidelines and regulations.
Consent for publication
All the authors approved the final manuscript and the submission to this journal.
Authors’ contributions
JD participates in conception and experimental design, data collection and analysis, and writing the draft; YR, JX and QH participate in data collection and analysis; TC participates in conception and experimental design, data collection and analysis, revising the draft, and providing financial support. All authors approve the final version of this manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the Research Project of School of Nursing, Zhejiang Chinese Medical University.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data provided in this study are available upon request from the corresponding author. These data are not publicly available due to privacy restrictions.