
Abstract
Objective
The Thrive by Five app promotes positive interactions between children and parents, extended family, and trusted community members that support optimal socio-emotional and cognitive development in the early years. This article aims to describe the protocol for a prospective mixed-methods multi-site study evaluating Thrive by Five using surveys, interviews, workshops, audio diaries from citizen ethnographers and app usage data.
Methods
The study activities and timelines differ by site, with an extensive longitudinal evaluation being conducted at two sites and a basic evaluation being conducted at five sites. The learnings from the more comprehensive evaluations inform the iterative research and development processes while also ensuring ongoing evaluation of usability, acceptability and effectiveness of the app and its content across varying contexts. The study evaluates: (1) the impact of the Thrive by Five content on caregiver knowledge, behaviours, attitudes and confidence; (2) how the content changes relationships at the familial, community and system level; (3) how cultural and contextual factors influence content engagement and effectiveness and (4) the processes that facilitate or disrupt the success of the implementation and dissemination.
Results
All in-country partners have been identified and data collection has been completed in Indonesia, Malaysia, Afghanistan, Kyrgyzstan, Uzbekistan, Namibia and Cameroon.
Conclusions
Very few digital health solutions have been trialled for usability and effectiveness in diverse cultural contexts. By combining quantitative, qualitative, process and ethnographic methodologies, this innovative study informs the iterative and ongoing optimisation of the cultural and contextual sensitivity of the Thrive by Five content and the processes supporting implementation and dissemination.
Keywords
Introduction
The importance of sociocultural context in early childhood development
The first 5 years of a child's life represent a critical period of development. The genesis of new synapses during the first year of life occurs at an estimated 150% that of adult levels. 1 Critically, these developmental processes are strongly sculpted by experiences with the environment. 2 To that end, through positive and responsive interpersonal relationships with parents, families, community members and peers, young children develop social skills and learn to identify and manage emotions, either independently or with the assistance of others.3,4 Further, cognitive stimulation (e.g. reading books, playing games and drawing) is critical for the development of foundational cognitive skills, including maintaining attention, following directions, communicating with others and problem-solving. 3 Highlighting the importance of a maximally enriched environment, research in developed countries has identified three aspects of parenting that are critical to healthy socio-emotional and cognitive development among young children, namely cognitive stimulation, caregiver sensitivity, and emotional warmth and responsiveness.5,6
One-quarter of the global population is comprised of children aged 14 years and younger, 7 with many growing up in low- and middle-income countries (LMICs). It has been estimated that more than 200 million children under the age of 5 years from LMICs were not reaching their developmental potential due to poverty, nutritional deficiencies and social factors (e.g. deficient care and lack of learning opportunities).5,8 Recently, using pooled data from the Multiple Indicator Cluster Surveys and Demographic and Health Surveys conducted in 35 LMICs, it was highlighted that 35.8% of 3- to 4-year-old children were failing to attain basic socio-emotional and cognitive milestones, with poverty and stunting being primary contributing factors. 3 Importantly, research has shown that responsive and stimulating caregiving can help mitigate the risks associated with social determinants of health and, in turn, promote healthy socio-emotional and cognitive development.9,10
It is important to recognise that the above referenced global knowledge base about early childhood development is based largely on research from Western, educated, industrialised, rich and democratic (WEIRD) contexts. 11 Definitions of healthy childhood development and optimal childcare are based on research that typically excludes findings from child development studies conducted with communities in the LMICs. Importantly, such studies often highlight the diversity of potential models of childrearing, socialisation practices and development pathways associated with varying sociocultural and environmental contexts. As an example, attachment theory has been postulated to be applicable universally; however, there are several factors underpinning attachment theory that are not compatible with cultural variability. 12 Specifically, attachment theory emphasises the importance of fostering secure attachment between the parent–child dyad; however, children raised in farming and village communities often have a broader network of multigenerational caregivers that play significant roles in their development. This example highlights the need to acknowledge in the global early childhood development literature that there is no single best way to support a child's healthy development. 11
Programmes targeting childrearing behaviours, attitudes, beliefs and knowledge are one way to intervene early in a child's development. However, parenting programmes cannot be generic or simply developed primarily in high income countries, but rather must be developed for the cultural context in which they will be implemented. Perhaps unsurprisingly, a meta-analysis showed that culturally adapted interventions were more effective than unadapted versions of the same intervention. 13 Indeed, effective multicultural parenting programmes include culturally relevant content and provide information and skills training to bolster the confidence of parents. 14 Demand for parenting programmes globally has been low due to stigma and a lack of awareness as to potential benefits to parents and families 15 ; however, such challenges can be overcome through mass media campaigns, 16 public health initiatives, 17 and flexible delivery methods, including via television, 18 radio 19 and web-based or app-based programmes. 15
Digital health solutions and their intersection with culture
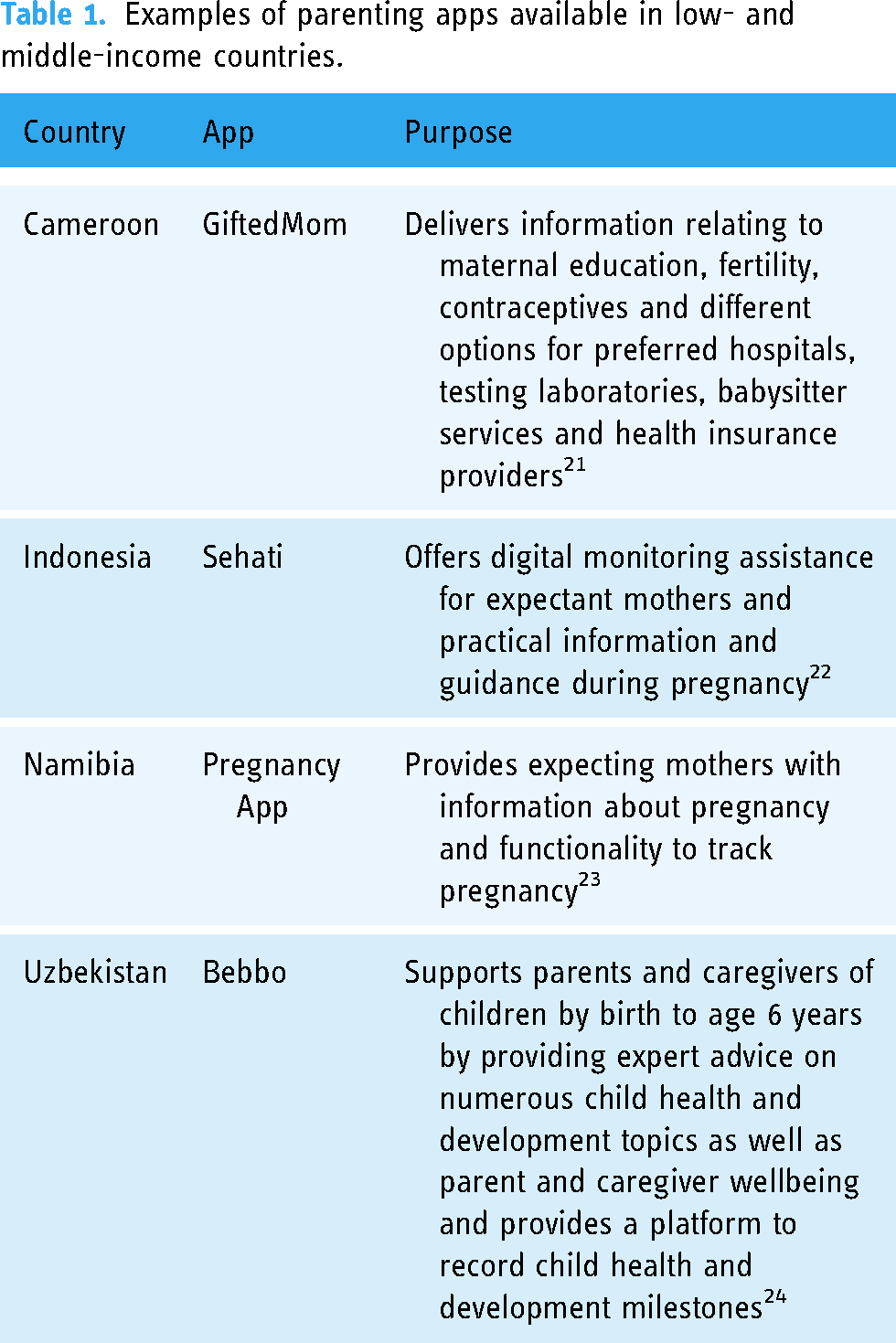
Mobile technologies are the primary point of access to the internet in LMICs, with 4G mobile broadband connections comprising 88% of total broadband connections. 20 As such, there is now a tremendous opportunity to implement mobile health (mHealth) initiatives globally and particularly in LMICs. Indeed, a multitude of parenting apps largely focusing on pregnancy and developmental milestones have been developed and launched in country-specific markets with examples provided in Table 1.
Examples of parenting apps available in low- and middle-income countries.
It is important to recognise that the capabilities of mobile technologies extend well beyond information delivery or data tracking. Indeed, mobile media practices have transformed the way in which people communicate, seek out and share information, and care for others even from a distance, referred to as ‘digital kinship’. 25 Mobile devices have come to be a ubiquitous influence in interpersonal relationships, enabling and sustaining intergenerational connections, intimacy and monitoring, particularly with the rise of nuclear and/or non-traditional family structures. In this way, mobile media practices serve to create or reinforce networks, including preserving the more traditional multigenerational family structure. Even in settings where access to smartphones may be more difficult due to cost or availability, mobile devices are frequently shared among a family or community. 26 In this context, mobile technologies, including smartphone apps, have the potential to be a valuable tool to support a collective approach to childrearing, facilitating communication and coordination of responsibility among caregivers (e.g. mother, father, grandparents and nanny). 25
Importantly, digital technologies can also directly influence some of the cultural and societal barriers to care access and quality. For example, an evaluation of a digital perinatal mental health screening programme for women of refugee and migrant backgrounds delivered via iPad in common languages (e.g. Arabic, Dari, Farsi, and Tamil) at an Australian antenatal clinic highlighted that participants felt more comfortable answering questions truthfully in this manner and that they would not otherwise have brought up their feelings to a health professional. 27 The option to complete the screening in their native language ensured that participants easily understood the questions and facilitated engagement with the programme.
Despite their potential to reduce health disparities, however, digital heath solutions are less frequently used by racial and ethnic minority groups, 28 immigrant groups, 29 and Indigenous and First Nations people. 30 As evidenced in the study referenced above, language has consistently been identified as a critical factor impacting engagement with digital health solutions by diverse groups, including low literacy in English and/or an individual's first language. 31 There is a strong preference for content that is accessible in the first language of users, including the use of local vernacular. 31 The cultural appropriateness of the digital solution is also vital, including recognition of community-level concerns, inclusion of culturally appropriate information, avoidance of cultural stereotypes or inaccurate representations of diverse groups, appreciation for cultural preferences for text-based or face-to-face communication, and exclusion of any content that might be triggering of past traumas. 31 Co-design, or the direct participation of the target end users in the design and development of digital health solutions, is an effective way by which to overcome these challenges prior to implementation.32,33 However, iterative testing and evaluation of the user experience and effectiveness in the real-world is also a critical way to ongoingly refine and optimise the solution to facilitate scalability and sustainability.
The critical importance of evaluation
Whilst there has been a proliferation of parenting apps globally, studies evaluating the impact of such mHealth solutions for children and their families, the broader community or at the system-level remain scarce. Notably, a systematic review found that apps that have been evaluated scientifically were typically not available commercially and vice versa, highlighting the marked disconnect between these two contributors to the mHealth landscape. 34 A recent assessment of 53 acute childhood illness apps available to North American parents and caregivers found that only 5 (9%) had been trialled for usability or efficacy. 35 Further, reviews of mHealth programmes in LMICs targeting child and maternal health have also highlighted a dearth of evidence with regards to usability, acceptability and effectiveness.36,37
The pace at which apps are being developed precludes a mandate for evaluation prior to commercialisation. However, to ensure the credibility and validity of apps, it has been recommended that academics and subject matter experts take the lead in developing app content. 38 This approach is thought to best enable the development of high-quality apps to distribute up to date, evidenced based information to target end users. Nevertheless, even amongst apps developed by researchers or subject matter experts, the research and development process typically stops at the point of implementation, rarely extending into a post-implementation evaluation phase.38,39 In instances where evaluations are conducted, they frequently emphasise the importance of the individual app user experience, ratings of app quality (e.g. Mobile App Rating Scale), 40 or qualitative user feedback collected via interviews to inform quality improvement or create case studies for marketing and communications purposes. 39 Randomised prospective clinical trials remain the gold standard for generating evidence of effectiveness. However, such studies are rarely practical for digital solutions due to the lengthy time required to conduct and publish the research, the dynamic nature of apps with ongoing updates and improvements, as well as the emphasis on outcomes for an individual end user. 39 Indeed, it is important that the definition of evidence extends beyond data collected in highly standardised, randomised controlled trials that are unlikely to reflect the real-world circumstances (i.e. the context) in which many digital solutions are implemented. 41 In this regard, the effectiveness of both the app and the implementation processes needs to be evaluated to inform iterative quality improvement processes to facilitate the sustainability of interventions. 42
Culture is a critical contextual facet when planning and conducting evaluation research. Evaluation tools and approaches need to account for local knowledge, practice and culture. When evaluating parenting programmes in diverse cultural contexts, this means assessing the validity and applicability of parenting measures that have been developed in Western cultures. 43 Drawing on anthropological and cultural psychological research on child development within targeted communities, 11 as well as working with an advisory group with contextual expertise to enhance sociocultural understanding at the community level, can enable better alignment of cultural context and evaluation study design. Further, the research team needs to ensure that collectively they have the requisite experience and knowledge to undertake the study in a culturally competent, appropriate and safe manner.
Language translation is also an essential consideration, with potential solutions including the use of bilingual/bicultural research assistants with training in in-language data collection, or professionally certified interpreter. 44 All text-based evaluation materials also require translation. Finally, providing feedback at the community level about the evaluation results, and how these might in turn be actioned to enhance outcomes, can also be an important way in which to build trust and foster an enduring relationship between researchers, organisations, and communities and ensure the sustainability of positive outcomes that are derived. 44
Despite the above noted challenges, robust scientific evaluation is critical to support the successful and sustainable implementation of digital tools. A recent scoping review and concept mapping study found 75 unique approaches to evaluating digital solutions. 45 From this review, the researchers developed the ‘eHealth methodological guide’ which matches potential evaluation methods with the research and developmental phase of the digital solution. Mixed-methods approaches that incorporate both qualitative and quantitative methods have been shown to be well suited to the evaluation of digital health solutions as the questions associated with such initiatives are frequently broad, complex and multifaceted. 46 By capitalising on the strength of both quantitative and qualitative evaluation strategies, researchers can develop a deep understanding of the complexities that underpin the development, implementation, scalability and sustainability of digital solutions. This includes recognising and evaluating how the digital solution interacts with and changes the context in which it is implemented. 47
Importantly, the relationship between the digital solution and the implementation context, including social, cultural, physical, infrastructural and public health dimensions, is dynamic and multidimensional. 47 Complexity approaches to evaluation have highlighted the limitations of relying on causal inference to understand the conditions that link the implementation of interventions and outcomes. 48 To account for such complexities, evaluations of digital health solutions can include multifaceted aims, including questions about usability, acceptability and effectiveness; changes in relationships at the individual, community or system levels; processes influencing implementation and outcomes; and the relevance of contextual factors throughout the research and development process. 47 This invites research on how digital solutions alter patterns of information giving and support seeking, developing an understanding of what existing activities are potentially displaced and tracking how resources (material, social and cultural) are redistributed or transformed through the implementation of the digital solution. 49 Finally, by establishing an iterative knowledge translation process, learnings from such an evaluation enable rapid adaptation of the digital solution and inform continuous communication with key stakeholders with regards to individual, community and system-level outcomes.41,42
Thrive by five
Minderoo Foundation's Thrive by Five International Program aims to empower parents with the knowledge they need to support the healthy development of their child from birth to age 5 and ensure universal access to this valuable parenting information regardless of sociodemographic background. 50 As described in detail in LaMonica et al., 32 the Thrive by Five app is the flagship product of this programme. The app and its content are freely available via local Apple and Android app stores, and are being iteratively designed and developed in collaboration with parents, caregivers and individuals with relevant subject matter expertise (e.g. early childhood education and curriculum development, psychology, medicine, education) in each of the countries where the Thrive by Five International Program will be implemented. Critically, prior to embarking on work in any country, an in-country partner(s) is identified to provide support, guidance and expertise throughout the duration of the project, including recruiting participants to engage in the evaluation study described in this protocol.
As described in detail in Crouse et al., 51 the Youth Mental Health and Technology Team from the University of Sydney's Brain and Mind Centre lead the development of the Thrive by Five content, referred to as Collective Actions. As shown in Figure 1, the key elements of the Collective Actions are the ‘The Why’ which reflect scientific information relating to early child development, presented in simple, user-friendly language. Each scientific fact is coupled with one or more childrearing activities for parents, extended family and trusted members of the community to engage in with the children to support their socio-emotional and cognitive development. Importantly, the co-design process outlined in LaMonica et al. 32 helps to inform the development, testing, and refinement of the content for the local context of each of the countries where the app is implemented. This process offers local stakeholders the opportunity to share their knowledge and expertise to inform, iterate, and tailor the features, functionality, and content to the local context.
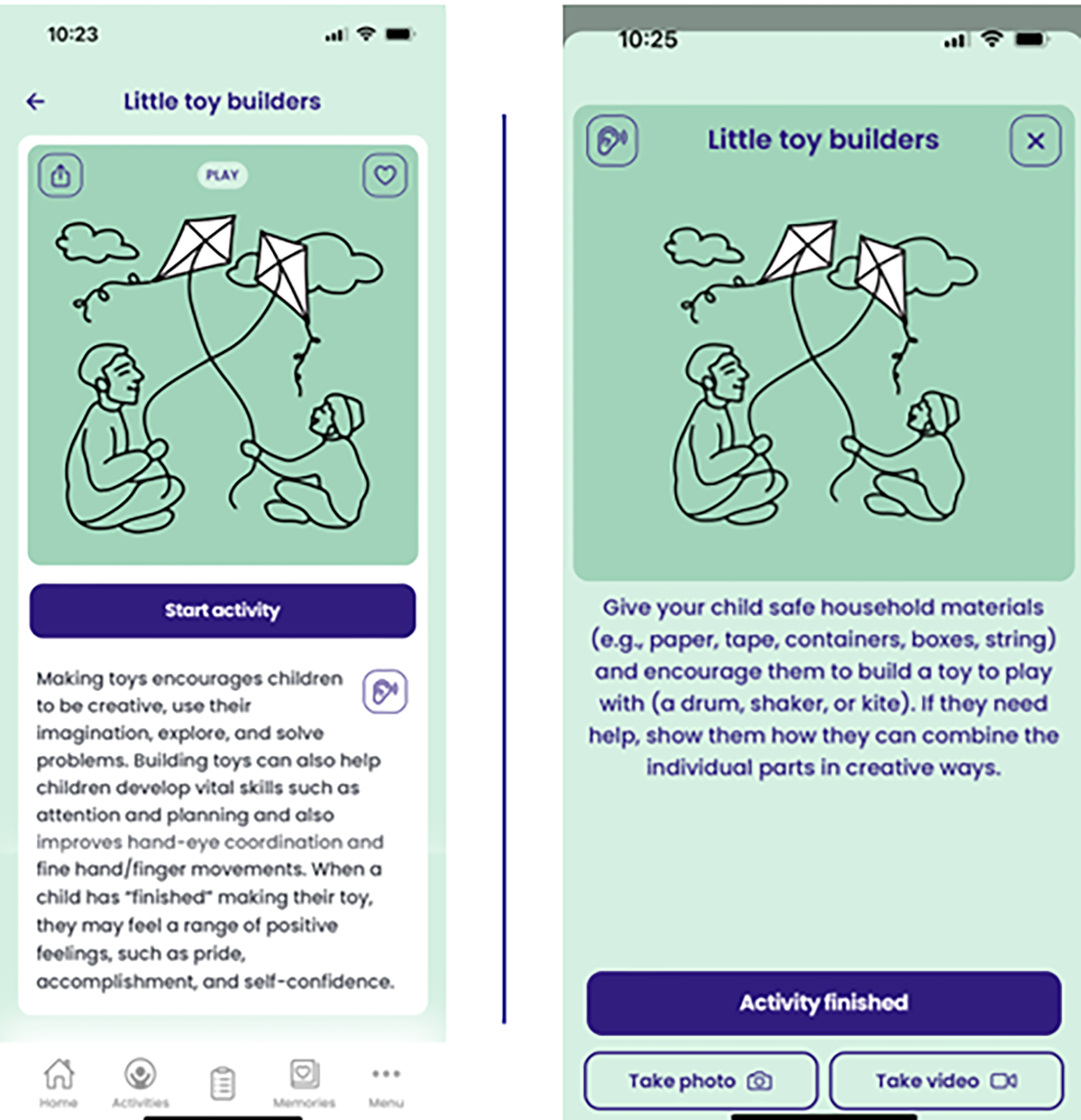
Example collective action.
The co-design research protocol 32 was adapted from the Medical Research Council's Framework for Complex Interventions 47 and emphasises the need for iterative research and development in collaboration with parents, caregivers, and early childhood subject matter experts to develop the content for each country in which Thrive by Five is implemented. After conducting a thorough literature review of the cultures, traditions and values of the people of the target country, the research team develops a preliminary content base comprised of 20 to 50 Collective Actions. After this content is reviewed and refined in collaboration with subject matter experts, the updated Collective Actions are populated into a test app for testing by at least 25 potential real-world users. Testers are invited to engage with the app and its content naturalistically (i.e. there is no minimum requirement for engagement) and participate in a co-design workshop to provide their feedback on the relevance and cultural appropriateness of the content to inform future refinement. Whenever feasible, testers are recruited from metropolitan, regional, and rural communities and included male and female caregivers from varied demographic backgrounds. The learnings from the co-design workshops directly inform the iterative refinement of the app and its content to enhance the usability, acceptability, relevance and cultural appropriateness for each country. Further details about the co-design process are available in the published protocol. 32
Objective
Childrearing apps generally and Thrive by Five specifically have the potential to empower parents and other caregivers with the knowledge and confidence needed to facilitate the healthy development of young children and to promote positive connections between children, parents, families and communities. However, as noted by Sanders et al., 19 it is now critical to evaluate the usability, acceptability, and effectiveness of the features, functions, and content of such apps as well as how these outcomes are influenced by implementation processes and contextual factors. The primary objective of this mixed-methods study is to evaluate the impact of the co-designed Thrive by Five app and its content on parent and caregiver knowledge, behaviours, attitudes, and confidence, and the impact of the app on the connection between the child and their parents, family, community and culture. We hypothesise that engagement with the Thrive by Five content will improve knowledge of early childhood development, reduce problematic childrearing practices, such as the use of physical punishment, increase the childrearing confidence, and strengthen connections between the child and their caregivers, community and culture. Secondary aims include the evaluation of the cultural and contextual factors influencing engagement with the content; how content engagement influences relationships at the parental, familial and community level; the cultural appropriateness and relevance of the content; the quality, usability, and acceptability of the app and content; and the processes that occurred prior to and during implementation of the Thrive by Five app that influenced awareness, uptake, adoption and engagement. The protocol presented in this article was developed at the outset of this large-scale international project, prior to any data collection.
Methods
Study design
This prospective mixed-methods, multi-site evaluation study uses surveys, semi-structured and conversational interviews, workshops, audio diaries, and app usage data to evaluate the impact of the Thrive by Five app and its content, as well as the processes and contextual factors that influence and shape its implementation, usage and effectiveness.
Sites
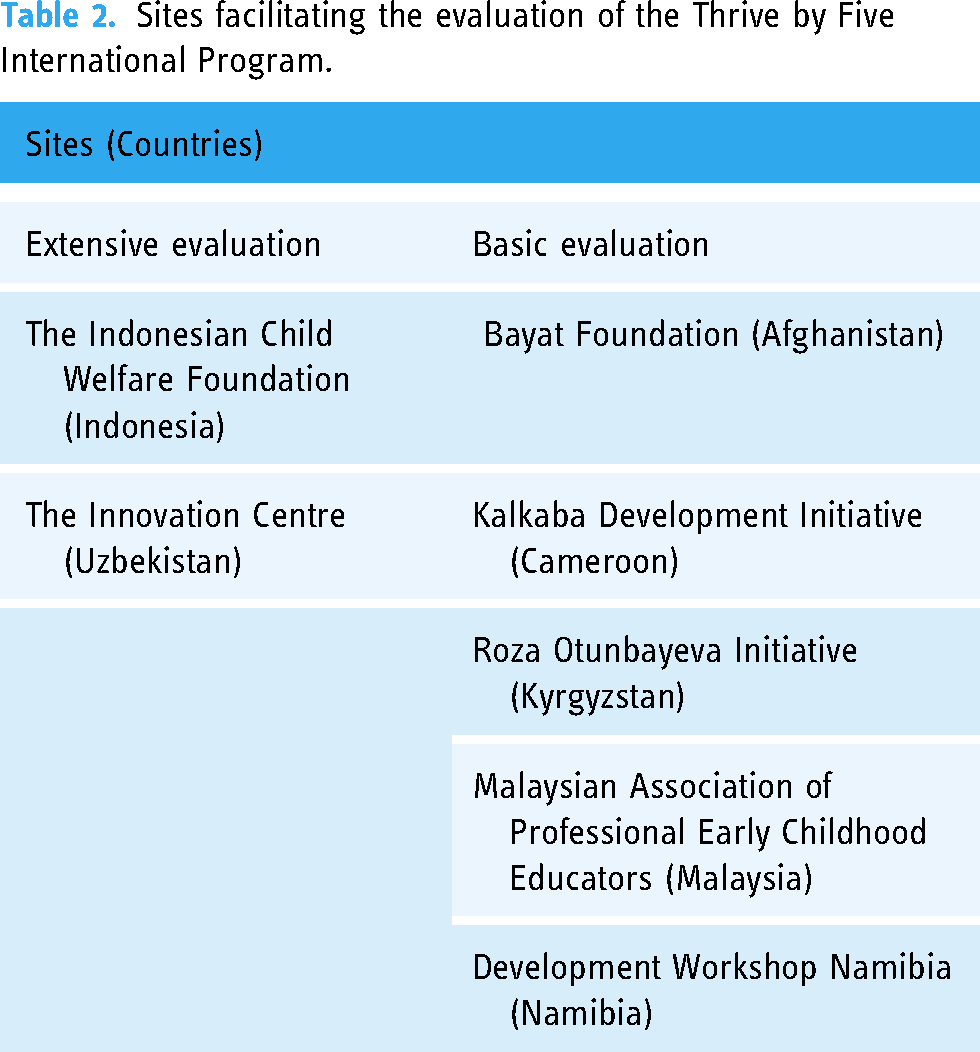
This study focuses on the evaluation of the Thrive by Five childrearing app and its content at seven sites located in LMICs. As shown in Table 2, for each country, there is one identified local site that facilitates the research activities. The data collection for this research took place over 2 years and is now complete. The study activities and timelines differ depending on site, with an extensive longitudinal evaluation being conducted at two sites (see Table 2) and a basic cross-sectional evaluation being conducted at the remaining five sites. Across the project, the countries in which the sites were located were grouped by geographic region, including Africa, Central Asia and Southeast Asia, with a leading extensive evaluation site selected in each region. The extensive evaluation sites were identified by Minderoo Foundation based on the country's population size (i.e. larger population sizes were expected to afford more opportunity for programme impact and learnings) and planned project timelines. In relation to the latter, sites with implementations planned earlier in the project were selected for extensive evaluation to enable learnings from these more in-depth longitudinal studies to be translated into the research and development processes for other sites in the same region. The basic evaluation is then designed to investigate the similarities and differences in outcomes across the remaining sites in the region.
Sites facilitating the evaluation of the Thrive by Five International Program.
A Site Principal Investigator is responsible for the conduct of the research at each site and ensures that the study is conducted ethically and in full accordance with the research protocol. Importantly, a co-investigator from the University of Sydney research team trained in Good Clinical Practice provides training to the Site Principal Investigator and any other members of the site-specific research team with regards to the research protocol, recruitment and consenting processes. This ensures delegated site staff understand and can explain to participants the study aims, the eligibility criteria for participants, the research activities including expected duration of participation, and any potential risks or benefits to participants. The University research team also assists the Site Principal Investigator in ensuring that the appropriate country-specific ethics and governance approvals are obtained prior to commencing the research.
Participants
Eligibility criteria
Participants are parents and caregivers (e.g. grandparent, aunt, uncle and nanny) who have used the Thrive by Five app and its content. There are no minimum requirements with regards to contact with the child to be eligible to participate as a caregiver. For the purposes of inclusion in the study, participants must be 18 years of age or older, self-identify as a caregiver for at least one child under the age of 5 years, and have engaged with the content in a manner of their own choosing, either on their own smartphone or on a device shared with other family members or close friends. There were no specifications set as to the frequency of app use, time spent on the app, level of app engagement or the number of Collective Actions completed. For the purposes of evaluation, it is critical to capture the breadth and range of ways in which people have used the app. As identifying information is not collected during the evaluation or in the Thrive by Five app, it is not possible to link evaluation participants to their app usage data. However, self-reported app usage is collected in the survey as well as during the qualitative interviews and workshops. Participants must be literate to complete the surveys; however, participants who cannot read have the opportunity to participate in semi-structured interviews and workshops in countries where the extensive evaluation is being conducted. Individual participants from the same family or household can participate in the evaluation activities.
Staff from Minderoo Foundation, members of the site-specific research team, local subject matter experts and other key stakeholders actively involved in the development and implementation of Thrive by Five are also eligible to participate in semi-structured and conversational interviews about the processes that underpinned the implementation, to understand the contextual factors that impacted on study participation, app uptake, usage and adoption, and content dissemination.
Sample size
The minimum sample sizes for each research activity are presented in Table 3. For the extensive evaluations, assuming 80% power is sufficient to detect a medium effect size (Cohen's d > 0.50), a power analysis using G*power indicated that a minimum sample size of 150 participants across the three groups will be sufficient to support our planned quantitative analyses of the impact evaluation survey. 52 Therefore, a minimum of 50 surveys will be collected at each of the three time points (≥150 total surveys). Wherever possible, a minimum of five semi-structured interviews and two workshops will be conducted with parents and caregivers at each of the three time points of 2-, 10- and 24-week post-launch of the app. Additionally, conversational interviews will be conducted with collaborators and key stakeholders (e.g. site-specific research team and Minderoo staff). For the interviews with collaborators and stakeholders, the concept of “information power” will be applied, where the more information the sample holds relevant to the inquiry, the lower the number of participants needed. 53 Additionally, the number of participants interviewed will be limited, until adequate information is obtained and where there is no new information or themes. 54 The target number of interviews is therefore flexible.
Minimum sample sizes for research activities.

*This part of the evaluation is optional depending on the interest and engagement of participants. A maximum number of citizen ethnographers and audio diaries was used as a guide to ensure feasibility of data collection and analysis within project timelines and to minimise the potential for participation to become onerous or burdensome to participants.
In accordance with the Central Limit Theorem as well as our team's extensive experience conducting survey studies, a minimum of 100 participants will be recruited for basic evaluations, which is expected to enable basic group comparisons (e.g. male and female caregivers). 55 Participation in citizen ethnography (described in greater detail below) is an optional component of the extensive evaluations.
Recruitment
Parents and caregivers
Recruitment for research activities with parents and caregivers will be facilitated by the sites in each respective country using their established networks and advertising mechanisms led by the Site Principal Investigator. The research team meets online with the sites to discuss strategies to recruit a diverse sample of participants as well as to address cultural and contextual challenges as they arise. The respective sites use the recruitment methods best suited to their community and context (e.g. emails, poster displays, paper-based and online internal news articles, handouts, digital advertisements on social media). It is expected that some passive snowballing will occur as the study is shared with others to increase the participant pool. 56 Interested potential participants need to contact the identified Site Principal Investigator or their delegate (details provided on all study adverts) who will then forward the Participant Information Sheet (PIS) and Consent Form in either digital or paper format upon receiving the request.
Site-specific research team, local subject matter experts and other key stakeholders
Recruitment for interviews with staff from Minderoo Foundation, site-specific research team members, local subject matter experts and other key stakeholders commences from the development and co-design phase of the Thrive by Five. 32 In order to gain in-depth understanding of the local contextual issues in preparation for the extensive evaluations, senior researchers (VL and ME) attend app co-design workshops conducted in the countries designated for extensive evaluation. During these workshops, potential participants who appear to be enthusiastically engaged and demonstrate an in-depth knowledge of the local contextual considerations relevant to the implementation of the Thrive by Five International Program are identified.
Informed consent
PIS and Consent Forms are available for and specific to each site. There is a PIS specific to the completion of the surveys. Consent is indicated by submitting the survey; therefore, a formal consent form is not required. For parents and caregivers, there is also a PIS and Consent Form specific to the semi-structured interviews, workshops, and citizen ethnography activities. Finally, there is a PIS and Consent Form specific to the involvement of staff from Minderoo Foundation, site-specific research team, local subject matter experts, and other key stakeholders in semi-structured and conversational interviews.
Whenever possible, web-based PISs are distributed by the country-specific site via REDCap, a secure electronic data collection and management tool57,58 hosted at the University of Sydney, using a public link or QR code. Importantly, each PIS is translated from English into up to three local languages in accordance with guidance from the site. Potential participants are allowed to review the study requirements in their own time and then those who are participating in the semi-structured interviews, workshops and citizen ethnography are asked to provide written electronic informed consent via REDCap. Given limitations in access to the internet in some countries where the study is being conducted, paper-based versions of the PIS and Consent Forms are distributed via post or by hand based on guidance from the site. In this instance, participants are asked to either return the completed paper-based survey as indication of consent or the signed consent form for the interviews, workshops or citizen ethnography to the Site Principal Investigator.
As many of the countries in which the Thrive by Five app will be implemented have low literacy rates (e.g. 43% in Afghanistan), 59 it is important that there is an option for participants who do not read to participate in the research activities. This is particularly relevant as the Thrive by Five app was developed with audio recordings designed to enable parents and caregivers with limited or no text-based literacy to use the app. In instances where a potential participant cannot read, the Site Principal Investigator or their delegate is responsible for reading the PIS and Consent Form for the interviews and workshops to the participant and subsequently answering any questions they may have about the study. Potential participants are given ample time to consider their involvement in the study. Oral consent is required from participants who cannot read prior to engaging in an interview or workshop and is documented by the Site Principal Investigator on a paper-based consent form.
Participant procedures
Basic evaluation
Four weeks after the Thrive by Five app and its content are implemented, the site provides participants with a web link or QR code providing them access to the impact evaluation survey via REDCap (see Supplemental Appendix 1). Paper-based surveys are also available and distributed by the Site Principal Investigator via post or by hand on as needed basis for those participants who do not have reliable access to the internet or a smartphone. The surveys are anonymous; however, basic demographic information (e.g. relationship to the child under age 5, sex, country of birth, language spoken at home, age, marital status) is collected for descriptive purposes. Participants are asked to complete the survey within 1 week of receiving it, with those completing it on paper returning the survey directly to the site. Importantly, the survey is translated from English into up to three local languages to enable participants to provide their responses in their preferred language. The survey is first translated by a professional translator. The translation is then reviewed and edited by a second translator, with any discrepancies or concerns discussed with the original translator. For all languages that have NAATI accreditation, the translations are NAATI accredited. NAATI is the national standards and certifying authority for translators and interpreters in Australia (https://www.naati.com.au/).
Specific scales, all of which have been used in cross-cultural contexts, included in the survey are: (1) the Parenting and Family Adjustment Scales, a 30-item validated measure of changes in parenting practices in response to parenting interventions,43,60,61 that has been adapted to (a) inquire about self-reported changes in childrearing behaviours and (b) include a ‘neutral’ response within the Likert-scale; (2) the Parenting Confidence Scale, a 15-item measure assessing how confident parents are in relation to their parenting skills62,63; and (3) the System Usability Scale,64,65 a 10-item 5-point Likert-scale evaluating the usability and acceptability of the app. The Parenting and Family Adjustment Scale is comprised of two primary scales: Parenting and Family Adjustment. The Parenting scale is then further broken down into four subscales, including Parental Consistency, Coercive Parenting, Positive Encouragement, and Parent-Child Relationship. Family Adjustment is comprised of three subscales: Parental Adjustment, Family Relationships, and Parental Teamwork. 60 The possible range of scores varies between 0 and 15 across all subscales. There is no predetermined cut-score for this scale, however a lower score is better as a rule of thumb. The score for the Parenting Confidence Scale has a possible range from 0 to 45, with higher scores indicating greater confidence. 62 Participants scoring 39 or lower on this scale may be experiencing low levels of parenting confidence. The System Usability Scale is comprised of 10 statements on a 5-point Likert scale with 5 negative-worded items (even-numbered) and 5 positive-worded items (odd-numbered). The overall score is calculated by subtracting 1 from the raw score for odd-numbered items and subtracting the raw score from 5 for even-numbered items. The adjusted score is summed and multiplied by 2.5 to get the standard score. The final System Usability Scale score ranges from 0 to 100, with scores above 68 indicating acceptable usability.66,67 The remaining survey questions were designed by the research team specifically for the purposes of this evaluation and examine app use and satisfaction, impact on a child's connection with their parent(s), family, community and culture and knowledge of early childhood development using categorical, Likert scale and True/False questions.
Extensive evaluation
The extensive evaluation with parents and caregivers is comprised of surveys, semi-structured interviews, and workshops at 2, 10 and 24 weeks after the Thrive by Five app is implemented. As only aggregate data from each time point is reported, participants have the option to complete a survey, interview and/or workshop at one or multiple time points. Change at the level of an individual participant is not being assessed. All participants are asked to provide basic demographic information for descriptive purposes. The impact evaluation survey (see Supplemental Appendix 1) administered at each of the time points is the same as that described previously for the basic evaluation. The qualitative component of the extensive evaluation is designed to explore the breadth and diversity of practices and change processes accompanying the use of the Thrive by Five app. One-on-one semi-structured interviews are conducted with parents and caregivers by a senior researcher (VL and ME) as guided by the interview schedule available in Supplemental Appendix 2. Similarly, group-based workshops are facilitated by two senior researchers (VL and ME) in accordance with the agenda provided in Supplemental Appendix 3. These interview schedules are used in a flexible manner to allow for contextual variation in understanding of particular concepts. For example, when exploring the cultural impact of the app, the notion of ‘culture’ may hold different meaning and value based on particular socio-historical circumstances and therefore may need to be approached differently in order to obtain an understanding of participant perspectives on the issue.
All interviews and workshops with parents and caregivers are conducted via ‘Zoom’, a secure cloud video-conferencing service with end-to-end chat encryption. Depending on the language used to conduct the interviews and workshops, an interpreter is available as needed to allow participants to communicate in their preferred language. Efforts are made to use the same interpreter throughout the research activities. Debriefs with the research team and translator are held at the conclusion of each interview and workshop to encourage reflexive discussions about translation 68 and impressions of the research event. These discussions are informed by an acknowledgement that ‘cultural knowledge is woven into vocabulary’ and that common English words relating to emotions, behaviour management and other evaluation topics of interest, may not exist in certain languages and vice versa. 69 With participant consent, the interviews and workshops are audio recorded to ensure that feedback and responses are collected accurately. Further, one to two scribes (AN and IUMZ) are also present to take written notes throughout the research activities.
While the above activities focus specifically on capturing responses from parents and caregivers, opportunistic semi-structured and conversational interviews are also conducted via Zoom with participants who have been actively involved in the country-specific development and iterative refinement of the Thrive by Five app and its content, such as staff from Minderoo Foundation, in-country partners from the site, subject matter experts and other key stakeholders (e.g. translators). These interviews strengthen the understanding of how the app and its content are embedded within broader public health contexts as well as system change processes. Interviews explore participants’ first-hand knowledge about the issues faced by users while engaging with the content and gain insights about behaviour changes or impediments that occurred as a result. 70 Interviews also include discussions about how participants use the content as part of their professional practice (if applicable), and their views on its role and value in relation to other public health or child development initiatives in the country. Additionally, in-country partners and key stakeholders involved with the implementation of the app are asked if they have insights as to why potential end-users may have chosen not to use Thrive by Five to identify potential targets for improvements in the app, content or broader programme of work.71–73 An interview guide is available in Supplemental Appendix 4.
Depending on the interest of participants identified by the sites, the extensive evaluation has the potential to involve ‘citizen ethnography’ to add additional perspectives and experiences of end-users that may not have been identified through other evaluation methods. ‘Citizen ethnography’ is an approach that has been used in other evaluation studies to inform quality improvement. 74 Highly engaged participants identified through semi-structured interviews or workshops will have the option to be enrolled in the study as ‘citizen ethnographers’, documenting their experiences using the Thrive by Five app and its content through recording rich in-the-moment insights using audio-diaries on their personal smartphone (i.e. Voice Memos for Apple devices and Voice Recorder for Android devices). Audio diaries have been shown to be an effective way to add greater depth to the data 75 and help to demographically broaden the study sample as they do not require written responses. 76 ‘Citizen ethnographers’ undergo a short training session via Zoom with a researcher (VL), an experienced ethnographer 77 with expertise in ethnographic engagements with new technology.78–80 This training supports participants to understand topics of interest for the evaluation, answers their questions, and encourages them to reflect and document their experiences engaging with the Collective Actions. It is expected that participants engage in this part of the research for up to 5 hours over 4 weeks during the extensive evaluation period. Upon completion of the ethnographic research activities, the sites provide participants with a link or QR code to REDCap which directs them to complete a brief, anonymous survey regarding basic demographic data and then they are able to securely upload their non-identifiable audio files. Data from uploaded audio-diaries is translated (if required), transcribed and coded alongside data from semi-structured interviews and workshops.
Incentives
Incentives to compensate participants for their time were offered based on each site's national paid participation rates and methods of reimbursement as recommended by the local ethics practices and committee's advice.
Data analysis
Data from the quantitative survey will be analysed through a mix of descriptive analyses, inferential statistical tests (e.g. two sample t-test), tests for variability (e.g. standard deviation (sd-test)), correlations and multivariate regression analyses. Descriptive statistics will be reported as mean (standard deviation) for continuous and normally distributed variables, median and interquartile range for skewed continuous variables, and number (percentages) for categorical variables. Scatterplots will be used to investigate the pattern of relationships (strength and direction) between variables.
The primary variables used in the analyses are summed scores of the Parenting and Family Adjustment Scale, the Parenting Confidence Scale, and the System Usability Scale, as well as a mix of categorical and continuous variables, such as age, gender, education, employment status, frequency of using the app and total number of children. For basic evaluations, two sample t-tests will be used to test for statistical differences in demographic groups (e.g. survey language and gender). In addition, sd-test will be used to check for the variability in responses to the same scale across different demographic groups. For extensive evaluations, two sample t-tests will be used to test for statistical differences in demographic characteristics and scores on the three primary scales across the points of collection. Multivariate regression will also be used to explore predictors of the dependent variables (i.e. the summed scores of the Parenting and Family Adjustment Scale, the Parenting Confidence Scale, and the System Usability Scale).
Interpretation of the qualitative data from the interviews, workshops and audio diaries, including transcriptions, will primarily follow established thematic techniques. 81 All raw data are reviewed and checked across all participants by a senior researcher to develop a coding framework outlining all key concepts. Subsequently, data is coded in NVivo 12 software 82 using this framework by two researchers (VL and ME) following an established iterative process of reading, coding, and exploring the pattern and content of coded data, followed by reflection and discussion to reach consensus. Importantly, as outlined by Braun and Clarke, the form and outcomes of the thematic analyses are expected to vary. 82 Given the comprehensive nature of the qualitative data that will be collected in this study, the specific approach to thematic analysis will be determined by individual research questions and aims. Additionally, alternate means of analysing qualitative data (e.g. grounded theory) may be explored.
As noted previously, participants from the same family or household can complete the survey. No identifying data are collected during the evaluation; therefore, statistically controlling for family or household is not possible. However, as each participant has an independent relationship with the 0–5-year-old child/children, statistical control for overlaps in family or household is not deemed necessary. Indeed, all data on the impact of the content on each participant's personal childrearing attitudes, behaviours, practices, and confidence as well as their relationship with the child will be included in the analyses.
Results
All data has now been collected for this study in accordance with the protocol presented in this article. Specifically, the extensive evaluation has been completed in Indonesia, with 158 participants completing the survey, 49 parents and caregivers participating in interviews and workshops, 10 in-country experts and collaborators participating in interviews, and 2 participants completing audio diaries as citizen ethnographers. The extensive evaluation has also been completed in Uzbekistan, with 152 participants completing the survey, 37 parents and caregivers participating in interviews and workshops, and 7 in-country experts and collaborators participating in interviews. The basic cross-sectional survey study has been completed in Afghanistan (n = 111), Namibia (n = 65), Kyrgyzstan (n = 116), Cameroon (n = 103) and Malaysia (n = 102). Reports summarising the evaluation findings, including recommendations with regards to how these learnings can be fed back into the research and development, implementation, and promotion and dissemination processes, are provided to Minderoo Foundation to inform the iterative refinement and optimisation of the Thrive by Five International Program. The results are also shared with in-country partners and collaborators to inform collaborative discussions about how best to action the findings to maximise impact.
Minderoo Foundation, in collaboration with the research team and the technology developers, is currently undertaking a period of innovation to plan the next iteration of the Thrive by Five International Program, including clarifying how to identify, reach and engage target end users who are most likely to be positively impacted by this initiative. This includes a review of the app and its features, functions, and content as well as the processes that support its development, implementation and dissemination, promotion, and sustainment. Given the extent of data collected during this multi-site mixed-methods study, the results will be published separately. This will include the results of the country-specific evaluation studies as well as findings derived from analyses of the comprehensive database. The first publications of the outcomes of this evaluation study are expected in mid-late 2023. As the data is analysed, the research team is synthesising the learnings to inform the study design for the next iteration of the evaluation to be conducted in association with the revised Thrive by Five International Program resulting from the above referenced innovation period.
Discussion
Global recognition of the importance of healthy early childhood development
Increased recognition of the importance of the early years with regards to long-term health and wellbeing outcomes has resulted in significant investment in early childhood development globally. Indeed, by July 2014, 45% of LMICs had established early childhood policies 83 and international organisations, such as the World Bank, have invested billions in projects focused on health, nutrition and population-based programmes for early child development. 84 Further, with the adoption of the United Nations Sustainable Development Goals in 2015, early childhood development has been recognised as a priority area by 193 world leaders. 85 Importantly, the rate of return for such investments in human capital decline in association with increased age. 86 In other words, the highest rates of return are associated with interventions implemented early in a child's life. 86
Childrearing programmes
Despite the recent attention paid to the importance of the early years, childrearing programmes remain relatively uncommon in global initiatives as a means to promote early childhood development. 19 In accordance with the Nurturing Care Framework, nurturing care is characterised by an emphasis on a child's health and nutritional needs, emotionally supportive and responsive interactions with caregivers, and stimulation, including age-appropriate opportunities for learning and play, all in the context of protection from adversities.87,88 Care is provided by the family but extends to the community, 89 forming a system supporting early child development including factors at the level of the caregiver (e.g. maternal health and education), family (e.g. economic resources) and society (e.g. safety and absence of stigma). 8 The Framework calls for programmes that inform and empower families and communities to support child development, with appreciation for the local context and the positive social norms and practices already in use. 88 To that end, the Thrive by Five content aims to provide parents and caregivers with information about the scientific principles that underpin the healthy socio-emotional and cognitive development of young children coupled with simple childrearing activities promoting these aspects of development. The content is informed by anthropology and is co-designed and iteratively refined in collaboration with local parents, caregivers and subject matter experts to be culturally informed and inclusive of place-based traditions, beliefs, values, stories, songs, dances and festivals. Further, the content champions the power of a collective group of quality caregivers to support early childhood development. To support the iterative redesign and refinement of the Thrive by Five app and its content, and to promote programme scalability and sustainability in diverse contexts, a robust scientific evaluation is now critical.
Limitations
We acknowledge that this evaluation study would benefit significantly from in-country fieldwork; however, this is not feasible given research programme funding as well as travel restrictions and safety concerns in some countries (i.e. the Taliban had regained control of Afghanistan when we conducted our evaluation). As such, this research relies heavily on the use of technology for both quantitative and qualitative data collection. Therefore, site-specific samples may be skewed towards individuals that are from a higher socio-economic group with greater access to digital technologies and/or from urban areas where digital infrastructure tends to be more developed. Additionally, evaluation participants are recruited by the in-country sites using their established networks which vary in relation to national reach. Taken together, these factors are expected to limit the representativeness of the country-specific samples and, in turn, the generalisability of the findings. It is also important to note that unreliable internet connections have the potential to disrupt qualitative interviews and workshops. Additionally, data collection is highly dependent on the quality of the translators which may vary by language, particularly where NAATI certification is not available. Finally, while the psychometric measures included in the quantitative survey have been used in studies in cross-cultural contexts, we acknowledge that they had not been validated for use in many of the countries in which the evaluation is conducted. Study limitations will be explored and discussed in greater detail in forthcoming papers detailing the evaluation results.
Conclusions
This protocol describes a multifaceted, mixed-methods evaluation study. The evaluation investigates the impact of the Thrive by Five content on parenting attitudes, behaviours, knowledge and confidence; familial, community and system-level relationships; and the bidirectional and dynamic interactions between cultural and contextual factors and content usage, engagement and effect; as well as the processes supporting implementation, dissemination and promotion. The research is being conducted in and culturally tailored to seven LMICs, each of which is multicultural and multilingual. Direct engagement with the community and in-country collaborators and experts forms the backbone of the research methodology, working to fill a marked gap in existing evidence in behavioural and social change efforts to improve early childhood health outcomes. Further, the inclusion of process evaluation and ethnographic methodologies are novel in child development research, including in the LMIC context. This innovative study is well-suited to the complexities of evaluating the impact of the unique, co-designed and evidence-based and place-based Thrive by Five content when implemented in diverse, dynamic and multifaceted sociocultural contexts. The learnings from this evaluation will inform the optimisation of the cultural and contextual sensitivity of the content and the processes supporting its implementation, dissemination and promotion to maximise impact for children, parents, families and communities. Furthermore, this study is an opportunity to gather evidence about the appropriateness and applicability of concepts from the global early childhood literature in diverse cultural contexts.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241242559 - Supplemental material for Promoting social, emotional, and cognitive development in early childhood: A protocol for early valuation of a culturally adapted digital tool for supporting optimal childrearing practices
Supplemental material, sj-docx-1-dhj-10.1177_20552076241242559 for Promoting social, emotional, and cognitive development in early childhood: A protocol for early valuation of a culturally adapted digital tool for supporting optimal childrearing practices by Haley M LaMonica, Yun J. C. Song, Victoria Loblay, Mahalakshmi Ekambareshwar, Aila Naderbagi, Iqthyer Uddin Md Zahed, Jakelin Troy and Ian B. Hickie in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241242559 - Supplemental material for Promoting social, emotional, and cognitive development in early childhood: A protocol for early valuation of a culturally adapted digital tool for supporting optimal childrearing practices
Supplemental material, sj-docx-2-dhj-10.1177_20552076241242559 for Promoting social, emotional, and cognitive development in early childhood: A protocol for early valuation of a culturally adapted digital tool for supporting optimal childrearing practices by Haley M LaMonica, Yun J. C. Song, Victoria Loblay, Mahalakshmi Ekambareshwar, Aila Naderbagi, Iqthyer Uddin Md Zahed, Jakelin Troy and Ian B. Hickie in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076241242559 - Supplemental material for Promoting social, emotional, and cognitive development in early childhood: A protocol for early valuation of a culturally adapted digital tool for supporting optimal childrearing practices
Supplemental material, sj-docx-3-dhj-10.1177_20552076241242559 for Promoting social, emotional, and cognitive development in early childhood: A protocol for early valuation of a culturally adapted digital tool for supporting optimal childrearing practices by Haley M LaMonica, Yun J. C. Song, Victoria Loblay, Mahalakshmi Ekambareshwar, Aila Naderbagi, Iqthyer Uddin Md Zahed, Jakelin Troy and Ian B. Hickie in DIGITAL HEALTH
Supplemental Material
sj-docx-4-dhj-10.1177_20552076241242559 - Supplemental material for Promoting social, emotional, and cognitive development in early childhood: A protocol for early valuation of a culturally adapted digital tool for supporting optimal childrearing practices
Supplemental material, sj-docx-4-dhj-10.1177_20552076241242559 for Promoting social, emotional, and cognitive development in early childhood: A protocol for early valuation of a culturally adapted digital tool for supporting optimal childrearing practices by Haley M LaMonica, Yun J. C. Song, Victoria Loblay, Mahalakshmi Ekambareshwar, Aila Naderbagi, Iqthyer Uddin Md Zahed, Jakelin Troy and Ian B. Hickie in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to thank all of the in-country partners, including the Indonesian Child Welfare Foundation (Indonesia), the Bayat Foundation (Afghanistan), Development Workshop Namibia (Namibia), Roza Otunbayeva Initiative (Kyrgyzstan), The Innovation Centre (Uzbekistan), Kalkaba Development Initiative (Cameroon) and the Malaysian Association of Professional Early Childhood Educators (Malaysia), for their assistance in facilitating local ethics and governance approvals and for recruiting parents, caregivers, and subject matter experts to participate in this research study. Additionally, we would like to thank all study participants who contributed their valuable, knowledge, and feedback. Finally, we are very appreciative of our partner, Minderoo Foundation, for their support of and contributions to this research.
Contributorship
Authors HML YJCS, JT and IBH were integral in securing funding to support the study. The impact evaluation study was designed by HML, YJCS, VL and ME, with additional insights and support from AN, IUMZ and JT. Scientific oversight and guidance were provided by YJCS, JT and IBH to ensure all activities were conducted responsibly and in a culturally appropriate manner. All authors contributed to and have approved the final manuscript.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: IBH is supported by a NHMRC L3 Investigator Grant (GNT2016346). He is the co-director, Health and Policy at the Brain and Mind Centre (BMC) University of Sydney. The BMC operates an early-intervention youth service at Camperdown under contract to headspace. He is the chief scientific advisor to, and a 3.2% equity shareholder in, InnoWell Pty Ltd which aims to lead transformation of mental health services internationally through the use of innovative technologies. VL is a board member for Matana Foundation, a philanthropic organisation that provides funding to programmes for disadvantaged young people in Australia. She does not receive any financial benefit for this role. No other authors have competing interests.
Ethics approval
This study has been approved by the University of Sydney Human Research Ethics Committee (HREC) (Project 2021/956). Where a country-specific HREC exists, a site-specific protocol and supporting documents will be submitted for local ethics approval, prior to initiating the research at the identified site. The Site Principal Investigator will assist in identifying the appropriate country-specific HREC as well as with the preparation and submission of ethics application as required. In instances where the country does not have a governing ethics body, the approval from the University of Sydney will apply as advised by the University of Sydney's HREC Office.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is being conducted by the University of Sydney's Brain and Mind Centre pursuant to an agreement between the University and Minderoo Foundation Limited (Minderoo). Minderoo's Thrive by Five International Program targets parents and caregivers of children 0–5 years to support the cognitive, socio-emotional development and wellbeing of young children across diverse cultures.
Guarantor
IBH.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.