
Abstract
Background
Digital testing services for sexually transmitted and blood-borne infections (STBBIs), such as GetCheckedOnline, experience significant user drop-offs. For example, 32% of GetCheckedOnline users needing testing at account creation do not test, constituting missed opportunities. We explored the influence of users’ expectations and experiences of GetCheckedOnline's web design and implementation on missed opportunities.
Methods
This interpretive description purposively sampled 14 GetCheckedOnline users who created accounts between April 2022 and February 2023, indicated needed testing at account creation but did not test. We conducted semi-structured interviews and cognitive walkthroughs of GetCheckedOnline on Zoom, exploring participants’ expectations and experiences, including problems using the service. Interviews were audio recorded, transcribed verbatim, and analyzed using reflexive thematic analyses.
Results
Three themes were identified: (a) transitioning between GetCheckedOnline and laboratory services is a major testing barrier; (b) users’ appraisal of their health and social contexts is a determinant of testing through GetCheckedOnline; and (c) tailoring GetCheckedOnline's design and implementation to accommodate varying user needs can promote equitable testing. Health equity issues occurred along sociodemographic gradients as the GetCheckedOnline-laboratory transition was more onerous for older users. Users’ appraisal of their testing needs which varied by age and gender, and their assessment of time, and travel requirements for testing in remote communities influenced testing. Learning about GetCheckedOnline from healthcare providers improved testing compared with learning about the service through Google search which raised trust concerns regarding GetCheckedOnline's authenticity. Suggested improvements to promote health equity include personalized education, mail-in testing options, and simpler seamless web experiences.
Conclusions
To promote equitable access to digital STBBI testing services such as GetCheckedOnline, we can adapt web-design and implementation to suit user needs and contexts, ensuring simplicity and options for testing that reduce user burdens.
Keywords
Introduction
Digital testing services for sexually transmitted and blood-borne infection (STBBI) have become more prominent over the past decade.1–3 These services can help to address rising incidence rates of STBBIs, including syphilis and chlamydia which have increased by 1.70% and 0.29% per year globally between 2010 and 2019.4,5 Various models of digital STBBI testing have been implemented to circumvent the traditional required consultation with healthcare providers (HCPs) before testing.1,6 These services are believed to be more accessible, convenient, cost-effective, and potentially empowering testing alternatives2,6–9; and may surmount barriers to in-clinic testing including long appointment waitlists, clinic wait times, travel requirements, and experiences of stigma and discrimination.7,9 This is especially important for marginalized populations who bear disparate STBBI burdens and barriers to clinic and provider-based testing.6,10 However, these benefits have mostly been demonstrated within pilots and small-scale services, with limited health equity impacts at scale. 11
At scale, digital STBBI testing interventions have not achieved their potential for equitable access.12,13 In a scoping review, our team found uptake of digital STBBI testing occurred largely along sociodemographic gradients. 12 White people, women, and urban residents with higher socioeconomic status were more likely to use these services.12,13 Irrespective of digital STBBI testing models (including those using online requisition and laboratory sample collection, online postal self-sample collection services (OPSS) or self-sample collection and interpretation (i.e. self-testing)), there are significant drop-offs along the service cascade (i.e. rate of abandonment of testing before completing all testing steps).3,8,11 For example, for models that use online requisition and laboratory sample collection, only 30–37% of users who create laboratory requisition forms submitted specimens.3,14 For models with OPSS services, only 58–65% of people who order kits return them for laboratory testing.15,16 While higher completion rates (up to 82%) are reported in pilot studies incentivizing testing, this approach is not sustainable in real-world settings due to cost implications.8,17
Despite researchers’ recommendations to investigate reasons for drop-offs, limited evidence has been generated to support possible solutions. 14 Where available, the limited evidence primarily focuses on OPSS models and reasons for unreturned test kits. A 2016 study of an OPSS program with options for home sampling test kits delivered at nearby pharmacies found that clients in areas with a higher index of multiple deprivation were less likely return test kits due to difficulties accessing these locations and concerns about non-discrete physical spaces for specimen collection. 16 Another study suggests that while OPSS increases users’ sense of control, apprehensions about delayed test results, loss of postal samples, and users’ lack of self-efficacy for self-sample collection limits testing. 18 An important yet underexplored aspect of these drop-offs is missed opportunities for testing, which we describe as inability or unwillingness of an individual to test despite needing testing when accessing the service. We need to understand how often missed opportunities occur and if they occur differentially within populations. This is an important public health issue considering missed opportunities may be the only opportunity for many people to access STBBI testing whether online or through provider-based testing, and could have implications for design and implementation.6,19
GetCheckedOnline is a provincial digital STBBI testing service launched in 2014 in British Columbia (BC), Canada to provide low barrier testing especially among marginalized populations. It follows an online requisition and laboratory sample collection model, experiencing similar drop-offs and potential missed opportunities. 3 A 2022 client survey of GetCheckedOnline users who had created an account found a third (32%) of people who reported needing testing at account creation did not complete testing process (i.e. experienced a missed opportunity to be provided STBBI testing). 20 Missed opportunities to provide testing were more likely to be experienced among people who did not find GetCheckedOnline's website easy to use, were concerned about privacy when using GetCheckedOnline, could not easily get to a laboratory, did not agree that GetCheckedOnline offered all needed tests and who preferred OPSS. These associations varied along sociodemographic gradients. Missed opportunities were more likely among people with annual income less than $20,000CAD, who reported the website was difficult to navigate, and among women and immigrants who could not easily get to a laboratory [unpublished report]. Current evidence on missed opportunities for digital STBBI testing interventions primarily explores individual-level characteristics of users completing testing. 21 This approach inadvertently places responsibility for testing barriers on people experiencing disparities. 21 The current study is designed to understand users’ experiences of the design, implementation, and socio-techno-political contexts of digital patient portals to provide evidence, for GetCheckedOnline and other similar interventions, to enhance health access by reducing missed opportunities,21,22 while potentially improving equity. 12 These findings emphasize need to further adapt current models to improve equitable access on GetCheckedOnline.
Building on the previous survey, this interpretive descriptive study aimed to explore users’ expectations and experiences of GetCheckedOnline's web design (i.e. user interface/experience (UI/UX)) and implementation (i.e. organization of systems required to get an STBBI test including getting a test requisition, accessing a partner laboratory, and submitting a specimen), and how these expectations and experiences influenced their experience of missed opportunities on the service. Secondarily, we explored these expectations and experiences to inform program adaptations to potentially promote equitable access. We asked the following research questions: how do clients who do not test despite reporting needing to test describe their expectations and experiences of the design and implementation of GetCheckedOnline? and, what might be learned from users’ experiences to reduce events of missed opportunities to provide testing on GetCheckedOnline?
Methods
Study design
We describe users’ experiences of GetCheckedOnline's design and implementation in the context of missed opportunities and interpret these experiences using the method of interpretive description developed by Thorne and colleagues. Interpretive description is a methodologically rigorous, yet flexible way to generate knowledge in an applied public health context.23,24 We applied a pragmatic yet critical lens, seeking to critique current systems while informing adaptations to promote health equity and social justice.23–25 Our inquiry was shaped by beliefs of users’ multiple realities, shaped through sociocultural contexts and we co-constructed knowledge outputs based on this belief and our interpretation of these realities.23,25 Our study methods sought to amplify voices of marginalized communities needing STBBI services the most. This study drew on Crawford and Serhal's Digital Health Equity Framework (DHEF) for theoretical underpinnings. The DHEF suggests digital determinants of health (e.g. digital access, digital health literacy, and beliefs about the helpfulness or harmfulness of digital technology) interact with intermediate health factors including health-related beliefs and behaviors along with health service resourcing and quality of care (e.g. timeliness, person-centeredness) to influence equity in access and outcomes of digital health services. 22 The DHEF suggests digital determinants of health are influenced by peoples’ intersecting social locations (access to resources based on social identity).22,26 This study further drew on the Unified Theory of Acceptance and Use of Technologies (UTAUT) to explore how users’ expectations of benefits of using technology (i.e. performance expectancy), expectations of efforts required to use technology (effort expectancy), social influences to use technology and the presence of facilitating conditions (e.g. presence of infrastructure to support the technology's use) determine their acceptance and use of technology. 27
Reflecting on positionality, the authors recognize their background, experiences, and perspectives shape the approach to this study. For instance, the first author (II) and senior author (MG) are physicians experienced with implementing digital interventions for testing, care, and treatment for HIV and other STBBIs across high and low-income contexts. Research team members are also community-based, and public health researchers (RK, AS, DG, and CW), while others (II, DH, HP, MB) have experience with human-centered design. This study is situated in a larger team grant promoting digital health equity using implementation science. This equity focus is built on shared experiences of intersecting minority identities and an understanding of the impact of social and structural oppression on health access. II is a recent immigrant of Black African descent. These experiences influenced our philosophical assumptions as described, the study design, data collection, and the reflexive thematic analyses.
Study setting and sampling
Described in detail elsewhere, GetCheckedOnline is currently run by the BC Centre for Disease Control (BCCDC) in eight urban, semi-urban, and rural communities in British Columbia, Canada in partnership with a privately-owned laboratory service provider through laboratory locations in all eight communities.3,28 These communities have populations ranging from over 8000 in rural setting to approximately 2.6 million in large urban settings, with varying incidence rates of STBBIs (Appendix 1). Within these communities, STBBI testing is freely available through provincial health insurance for most people, except for recent immigrants awaiting registration in the provincial insurance plan. These recent immigrants may freely access testing through various public health initiatives, depending on their awareness of these services. Testing can be accessed at multiple locations including specialized sexual health clinics, family practices, or hospital emergency rooms. 29 However, people's access to testing varies based on factors like having a primary care provider, wait times, and travel requirements.
To test on GetCheckedOnline, users create an account after getting an access code by requesting on the website or from a health provider or promotional materials. Users then complete an STBBI risk assessment questionnaire, consent to testing, download a laboratory requisition form with recommended tests, and visit any designated nearby laboratory to submit specimens (including blood, urine, and swabs). Results are received online (if negative) or by phone (if any of STBBI tests are positive) with linkage to treatment facilitated by public health nurses. Since December 2023, approximately 3000 STBBI monthly test episodes (an instance of a STBBI tests conducted, irrespective of the number and types of tests in each requisition) are conducted via GetCheckedOnline. Based on 2021 estimates, GetCheckedOnline represents more than 8% of all tests in BC jurisdictions where the service is available. 30
Participant recruitment
We recruited a stratified purposive sample of GetCheckedOnline users who participated in the 2022 GetCheckedOnline client survey, aged 16 years and older, who had created accounts between April and October 2022, consented to contact for research and evaluation during account creation, indicated they needed to test for STBBIs when creating their accounts, but reported not testing during the survey, were English speaking and consented to the current study. We recruited participants in two phases. First, we sent recruitment notices to email addresses provided by participants during the initial survey, using an official BCCDC account associated with GetCheckedOnline. Emails were sent to all 103 participants who met the inclusion criteria. In the second phase, we expanded the recruitment pool given limited responses in the first phase. We invited users meeting previously described eligibility criteria who created an account between October 2022 and February 2023 but had no record of testing and had not participated in the 2022 GetCheckedOnline client survey. We sent rolling invitations based on gender and sexual identity. For users responding to recruitment emails in the second phase, we confirmed if they needed testing at account creation but had not tested through GetCheckedOnline. For all eligible users who responded to recruitment emails, we sent pre-screening questionnaires to assess their sociodemographic characteristics, serially inviting them for interviews, ensuring diversity based on participants’ sociodemographic, ethnic, and sexual identities.
We determined initial minimum sample size of 18 representing six participants per stratum for each of the three main strata for social variables including age, geographic location, race/ethnicity, and gender.23,31 We successfully recruited only 14 participants for interviews greater than six months after they created accounts (12 from recruitment phase one and 2 from phase two). Within the sample, 4/14 (29%) participants eventually tested via GetCheckedOnline despite initially indicating missed opportunities. These users were included to understand how deviant experiences influenced testing over time.
Data collection
Fourteen semi-structured interviews were conducted between March and November 2023, lasting approximately 30 min (range: 18–48 min). All interviews were on Zoom with only the participant and interviewer in attendance. Participants were in their homes or other selected private spaces and had no prior relationship with the interviewer. For one participant without a stable internet connection, the interview was conducted by phone. The interviewer followed a topic guide (Appendix 2) which was piloted using interviews with four participants and adjusted to improve its clarity. Data from the pilot interviews was included in the study given no discernable differences in responses and an overall small sample size. All interviews were conducted by II, a physician and PhD candidate, with 5 years of training and experience conducting interviews. During interviews, participants were asked about their expectations and experiences using GetCheckedOnline for STBBI testing, reasons they sought GetCheckedOnline compared with other STBBI testing options, and reasons for test noncompletion, including issues encountered with GetCheckedOnline.com, and before or during their laboratory visit for specimen submission. For seven participants who had difficulty recollecting their experiences regarding specific aspects of the website's interface, cognitive walkthroughs of GetCheckedOnline were conducted, exploring the website interface from account creation to getting a laboratory appointment using the Zoom screen share function. 32 Participants were encouraged to think aloud about their observations and recollections of their experiences—a common approach in human computer interaction research. 33 Audio recordings of each interview were created and stored on encrypted digital devices. Recordings were auto transcribed using Zoom's transcribe function. Verbatim transcripts were reviewed for accuracy and corrected where necessary. Detailed field notes were collected by the interviewer to document impressions of the interviews in real time.
Ethics
Ethics approval was obtained from the University of British Columbia's Behavioral Ethics Board (ethics #H22-03148). Written informed consent was obtained from participants at least 24 h before each interview using a Qualtrics survey instrument, emphasizing voluntary participation. Each participant received a $50 CAD gift card as honorarium. Upon commencement of each interview, participants were assigned a code for all documents collected from their interviews without personal identifiers.
Data analyses
Verbatim interview transcripts, field notes, and the pre-interview survey data were imported into QSR NVivo version R 1.3 for data management and analyses. 34 A reflexive thematic analysis was conducted by one researcher (II) following Braun and Clarke's recommendations.35,36 First, II comprehensively read interview transcripts identifying broad ideas within the data. This was followed by line-by-line coding focusing on participants’ processes for deciding on STBBI testing, learning about GetCheckedOnline, and testing or not testing through the service (i.e. process coding). This approach aimed to clarify users’ expectations and experiences, potential tension points between them, and to describe design and implementation characteristics potentially accounting for testing noncompletion on GetCheckedOnline. Beginning with an inductive process (four transcripts), an initial codebook was generated, with subsequent coding following a deductive-inductive approach (Appendix 3). Thereafter, codes were reviewed and grouped into categories and themes based on similarity of described processes both at a latent and semantic level.36,37 II routinely reviewed the evolving codebook and preliminary themes in collaboration with the research team and refined the themes through consultations with GetCheckedOnline's Sexual Health Advisory Group—a group of users and community STBBI advocates with lived experiences of marginalization and seeking STBBI testing within current systems.
Data collection and analyses followed an iterative approach with subsequent interviews being adapted to emergent findings. For example, trust became a recurring theme early in the interviews, so subsequent interviews were adapted to explore this concept in relation to experiences of missed opportunities. To explore equity, codes and identified themes were cross-tabulated by socio-demographic characteristics, examining similarities and differences between groups using constant comparative techniques. 38 Throughout the analyses, II kept a reflexive journal and routinely discussed perspectives with the research team to further explore how researchers’ positionality and perspectives were reflected in the data. Knowledge translation opportunities were sought throughout the research as GetCheckedOnline's operations team were embedded research team members and contributed to the entire study. 23 Research reporting adhered to the consolidated criteria for reporting qualitative studies (COREQ) (Appendix 4). 39
Results
A sample of 14 participants were interviewed, including seven (50.0%) users 30 years or older, nine (64.3%) women, and six residents of large urban cities (Vancouver and West Vancouver (Greater Vancouver Regional District (GVRD))) (Table 1). Six participants (42.9%) self-identified as white, four (28.6%) identified as South-East Asian, seven (50.0%) identified as heterosexual, and four (28.6%) identified as gay, bi-, or pansexual. All participants had a mobile phone and 10 (71.4%) had experience using other health apps and websites. Overall, three main themes were identified describing the expectations and experiences of GetCheckedOnline's design and implementation among these users with missed opportunities to be provided testing (Figure 1). The themes are described further, embedding learnings about ways to reduce missed opportunities. Participant quotes are used to illustrate aspects of the analyses.

Map of themes identified in the 2023 GetCheckedOnline client interviews. Circles represent themes; boxes represent sub-themes; dotted lines represent relationships between the main themes and dashed lines represent relationships between sub-themes.
Participants’ characteristics: 2023 GetCheckedOnline client interviews (N = 14).
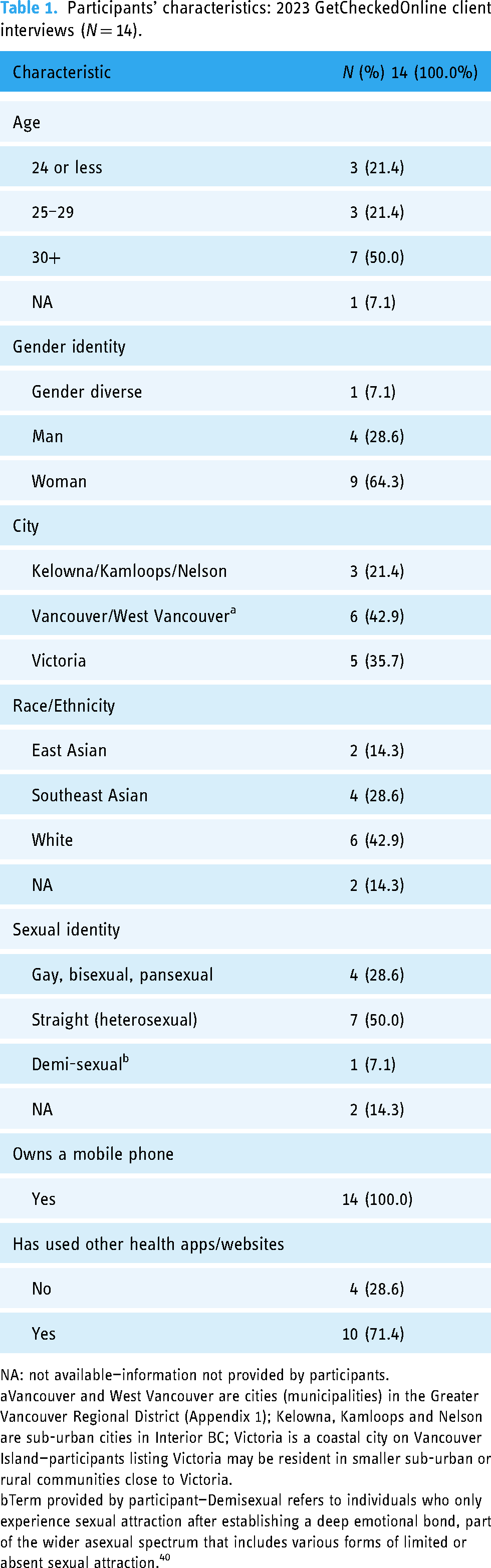
NA: not available—information not provided by participants.
Vancouver and West Vancouver are cities (municipalities) in the Greater Vancouver Regional District (Appendix 1); Kelowna, Kamloops and Nelson are sub-urban cities in Interior BC; Victoria is a coastal city on Vancouver Island—participants listing Victoria may be resident in smaller sub-urban or rural communities close to Victoria.
Term provided by participant—Demisexual refers to individuals who only experience sexual attraction after establishing a deep emotional bond, part of the wider asexual spectrum that includes various forms of limited or absent sexual attraction. 40
Transitioning between GetCheckedOnline and laboratory services is a major testing barrier
Most users described challenges transitioning between GetCheckedOnline's website and partner laboratory services for specimen submission. Most users with missed opportunities could create laboratory requisition forms but were unable to either get an appointment at a laboratory or go in-person to submit specimens. Some users suggested this transition was more onerous for older, less experienced users and emphasized needing more seamless experiences between GetCheckedOnline and partner laboratories, as one participant described: I think if you could have just one site, like if it could be all done through GetCheckedOnline, like you could book your appointments to [the laboratories] through GetCheckedOnline, it would be easier as opposed to getting your QR code [laboratory requisition] then having to go to a different website and then having to do it all over again. (#01, 25–29 years, Sexual Identity—NA, Man)
Participants described perceiving GetCheckedOnline and the laboratory as two separate organizations with different goals, struggling to work together. They suggested these perceptions were reinforced by requirements to use two different websites to access testing, differences in their previous experiences between GetCheckedOnline (often favorably perceived) and the laboratory, which was perceived as sometimes unsafe, inaccessible, or characterized by long wait-times. For example, a participant said: I think when we talk about this service GetCheckedOnline, it's also paired with the service provided by [the laboratories]. They are not connected; they are two different organizations. But because I am being sent to [the laboratories], I have to think “do I really want to go to a [laboratory]?” The customer service experience is as quick and efficient as possible. Sometimes the staff are fine but sometimes the customers and patrons are a bit unruly. (#03, 25–29 years, Gay, Man)
While most users acknowledged GetCheckedOnline's website was relatively easy to use, they described feelings of confusion and frustration with needing to create separate accounts on GetCheckedOnline and partner laboratory websites, seeing conflicting information across both websites, and not being fully aware about what to expect at the laboratory after getting a requisition on GetCheckedOnline. One participant explained: It [GetCheckedOnline] was pretty simple. As I remember, you can just fill the form. Then they just said like, here's the address of the clinic… close to you and you can just go there. We [participant and their partner] were like okay; we didn’t feel comfortable going there. Is there going to be a line? Is it going to be like you have to reserve a spot before? That was not clear. (#06, 30+ years, Straight, Man)
Users’ appraisal of their health and social contexts is a determinant of testing through GetCheckedOnline
Despite challenges experienced with transitioning between GetCheckedOnline and laboratory services, findings showed users’ appraisal of their health and social contexts was crucial in determining whether they persisted to test or not test via GetCheckedOnline. Intermediate factors shaped by users’ social contexts informed perceptions of GetCheckedOnline's relevance to them amongst alternatives. Users described assessing GetCheckedOnline's suitability to their testing needs which were on a spectrum ranging from precautionary (e.g. on entering a long-term sexual relationship or doing routine checks) to concerned testing needs (e.g. after having a perceived “high-risk” sexual encounter, partners with extra-relational sexual affairs, or being symptomatic). Assessments of GetCheckedOnline's suitability to their testing needs were also influenced by users’ self-perceived risks of STBBIs. A participant stated: I was having some different symptoms. Just some like irritation, some different discharge and stuff vaginally… I was like, this is a little different than my baseline. So, I had a few partners in the last couple of months and it was a little bit since I got checked. So, I figured it could be something along those lines, so I thought the safest thing to do would be to get checked. So, I kind of was like looking for a sexual health resource while I was in BC. (#08, 25–29 years, Straight, Woman)
Most users described how recommendation sources and social influences to use GetCheckedOnline influenced their expectations and ability to complete testing. Most users who reported learning about GetCheckedOnline from friends and family had expectations of its ease of use and convenience but were unprepared for the steps required to test. Users who learned about GetCheckedOnline through Google reported being similarly unprepared and confused, while users who learned about GetCheckedOnline from HCPs reported better preparedness for the steps required to test. One participant said: I think because the lady [HCP] that suggested I do this to begin with, mentioned that was through [the laboratory], I feel like I had it in the back of my mind. But I can see how it would be a little confusing to some people if you weren’t aware of the picture in regards to how to make an account with you [GetCheckedOnline] and then you have to make an account with [the laboratory]. (#01, 25–29 years, Sexual Identity—NA, Man)
Closely related to intermediate factors, users’ digital determinants of testing via GetCheckedOnline were described as factors influencing testing. Many users described their prior access, capability, and trust of digital health services like GetCheckedOnline as a key factor in completing testing. Participants who learned about GetCheckedOnline through Google search reported concerns with trusting its genuineness. Notably, partner logos available on GetCheckedOnline's website embedded links to other websites lacking security certificates. Some users suggested the security warnings reinforced trust concerns especially among recent immigrants with little knowledge of BC's health system. Contrastingly, users learning about GetCheckedOnline from HCPs, friends, and families (i.e. users with social and health systems connections) did not report trust issues as they confirmed GetCheckedOnline's genuineness through these social connections. One participant stated: Maybe I should be a bit hesitant just like giving out my info [on GetCheckedOnline] but I like felt pretty secure with it. Just people at work were saying like, oh yeah, you can do like a check online. So, like at least I talked to like a couple of coworkers about it [GetCheckedOnline]. Which did make me feel better. (#08, 25–29 years, Straight, Woman)
Users’ beliefs about the comparative advantages and features of digital STBBI testing were described as important factors especially in relation to their testing needs. Within our sample, younger men (<25 years) reported more concerned testing needs and wanted immediate access to treatment and HCPs to answer their questions. Some users considered these needs incompatible GetCheckedOnline's current model. Women reported more precautionary testing needs and indicated wanting convenience and a comprehensive battery of STBBI tests. Given GetCheckedOnline offers testing for five STBBIs as indicated on the website, some users with precautionary testing needs perceived testing through GetCheckedOnline as inadequate. They described having to navigate long wait times for clinic appointments to access all needed tests as an alternative. A participant stated: So yeah, when you go onto the site [website], it actually tells you what can you test for, or what can’t you? So, I was like, okay, well, that means that I have to do [the] test twice. I can do these ones right now and then, the other couple of them that I wanted to do, I will have to go and see a doctor and get the form whatever…. I went to the clinic that is like specially for doing all these things [STBBI tests], and I think it's like I had to wait for like 3 weeks, almost a month, and I was like, Oh, Gosh!. (#05, 30+ years, Bisexual, Woman)
Moreover, users described appraising their health and social context and the resource capacity and quality of health services to meet their testing needs. Most users described having access to an HCP and the resources required to access testing (e.g. travel requirements and time) as determinants of testing via GetCheckedOnline. Many described difficulties with accessing HCPs and testing locations especially with COVID-19 related clinic closures. They described resource requirements for testing on GetCheckedOnline as antithetical to its description as an easier alternative to in-person testing but also appeared resigned to this trend which reflects broader shifts in the responsibility of care to users with digital health interventions. Resource challenges were reported more among users outside the large urban GVRD where laboratory sites are sparsely distributed. For instance, a participant described struggling to plan their trip to a laboratory around work schedules: So, I made the account… I got the requisition. Then, yeah, I just kind of looked into the steps and I, yeah, found that I would have had to go to, Duncan, which is like in a half an hour drive from where I lived… So, it was just really hard to find a day with my work schedule that I could like drive myself over there and get that done. And so, I just kind of put it off for a while. (#10, 30+ years, Straight, Woman)
Users also described their assessment of their prior experiences with partner laboratories and STBBI testing services as a determinant of testing. Some suggested the laboratory was somewhat unsafe, impersonal, and characterized by long wait times which deterred test completion. For other users who eventually tested through GetCheckedOnline, prior understanding of laboratory processes either as health workers or in testing for other conditions was described as a facilitator of testing. Users’ English and health literacy also informed their ability to navigate testing steps. While users with English as a second language did not describe the language on GetCheckedOnline as a major determinant of testing, they described difficulty reading long text passages on the website.
Tailoring GetCheckedOnline's design and implementation to accommodate varying user needs can promote testing equity
Most users recognized their privileges in being able to use digital STBBI testing and emphasized the need to adapt GetCheckedOnline's design and implementation to make it more inclusive. They suggested accessibility improvements including simplified language or more language options for non-English speakers; and clarity in describing steps for testing on GetCheckedOnline, including dynamic “to-do” lists to inform users of their progress through the testing process. Users suggested needing more visual aids and pictures, integrated sexual and reproductive health services (especially for women needing pap smear tests and contraception), and more laboratory locations and mail-in testing options, especially for residents in remote locations. Some users suggested that mail-in options would be more aligned with their mental models of “testing online,” as this straight woman described: I have already mentioned that it would be nice if more [laboratories] offered the service. I wonder… it's not that it was a waste of time by any means because I did have the intention of going, but for me personally, I wonder if there was a little bit more information on like where one could go and like that it wasn't all online…. To be to be honest when I heard about tested online, I thought in my head maybe that I was like oh you get sent a kit in the mail or something and then you like send it back. (#09, Age—NA, Straight, Woman)
Many users described their use of GetCheckedOnline as a testing service and an STBBI education tool, highlighting the importance of personalized educational material depending on users’ testing states and whether users are accessing GetCheckedOnline for the first time. Users suggested education is important given the prevalence of unreliable information online. They emphasized needing clarity on what to expect through testing, and personalized connections especially for users in concerned testing states. Some users suggested options like phone calls or video chats as described by this participant: I think if you are on GetCheckedOnline… either you are trying to be precautious, or you suspect something's wrong with you. So, maybe for people that suspect there's something wrong with them that there is an option to talk to a doctor or a nurse [in real time]. Even if it is video chat or message to guide you as to what to do. (#01, 25–29 years, Sexual Identity—NA, Man)
Users concerned about testing may also move quickly through the website, missing its features and information. This was corroborated during cognitive walk-throughs with users who initially highlighted a lack of instructions about GetCheckedOnline's testing process and laboratory locations to support testing being surprised to these features when carefully exploring the website's interface. A participant who proposed clearer instructions about GetCheckedOnline's process expressed surprise when these features were highlighted on the existing website, suggesting that the user interface (Figure 2) may have distracted them: I wonder if before somebody makes an account, if there's information on locations where one would have to go, and just a little bit more information about how the process works… Oh my God! You have it, I’m sorry. Maybe It's because I did it on my phone and it was a little small, so all I saw was the login [create account button]. (#09, Age—NA, Straight, Woman).

GetCheckedOnline home page depicting design cues describing the testing process (highlighted in red) but often overlooked informed users’ perceptions of missing website features.
Discussion
This study explored how users’ experiences and expectations of GetCheckedOnline's design and implementation influenced missed opportunities to provide STBBI testing and assessed how these expectations and experiences may inform program updates that promote equitable testing access. The study identified three themes, each highlighting equity implications of users’ contexts during their interactions with GetCheckedOnline's web design and implementation, alongside the health systems’ role in these interactions. First, the transition between GetCheckedOnline and laboratory service is a major barrier to STBBI testing, with users suggesting this transition may be more onerous for older, less experienced testers. Second, users’ appraisal of their health and social contexts is a determinant of testing through GetCheckedOnline. Findings suggest users’ testing needs may vary by gender and age. Within our sample, young men reported more concerned testing which was potentially misaligned with GetCheckedOnline's implementation given timelines for results and connection to treatment on GetCheckedOnline. Older women reported precautionary testing but wanted comprehensive STBBI tests not currently available on GetCheckedOnline. Resource challenges accessing testing on GetCheckedOnline may also follow social gradients as time and travel requirements were more described by users living in rural communities in Vancouver Island, and Interior BC. Social connections including hearing about GetCheckedOnline from friends, families, and HCPs may improve trust compared with users who found GetCheckedOnline via Google search. Users who learned about GetCheckedOnline from HCPs may be more prepared for GetCheckedOnline's required steps. Third, users suggest tailoring GetCheckedOnline's design and implementation to accommodate varying user needs could promote testing equity. Users suggested personalized education, self-sampling, and mail in options and simpler integrated online experiences as web design and implementation changes to ensure equitable testing access for people with varied testing needs and for those in remote locations.
This study is the first to explicitly explore how web design and implementation of digital testing services may contribute to drop-offs within service cascades and missed opportunities to provide STBBI testing. 12 Where available, evidence from studies exploring OPSS services corroborate our findings that users’ perceived level of effort, self-efficacy for completing the testing process, and alignment of testing services with user needs significantly influenced test completion.16–18 Current study findings that travel requirements significantly affect test completion, especially for people with lower socioeconomic status have also been documented elsewhere. 16 This study extends the existing literature focused on OPSS models by qualitatively exploring design and implementation factors influencing missed opportunities on digital STBBI testing models based on online test requisition and laboratory specimen submission. Findings also explain our team's previous research from GetCheckedOnline's 2022 client survey that revealed ease of website use, difficulties accessing laboratories, and perceived inadequacy of available tests on the service were associated with missed opportunities to provide STBBI testing on GetCheckedOnline [unpublished report]. In the current study, ease of website use was found to be more complex than easily navigating GetCheckedOnline's website. Users’ challenges with ease of website use mainly imply challenges using all the different web services required for testing (i.e. inconsistent experiences across GetCheckedOnline.com and partner laboratory websites). Findings may also highlight the role of structural inequities which may be inadvertently reinforced for specific groups (e.g. women, low-income earners working jobs without access to paid medical leave and other similar populations) who seek alternatives to provider-based testing through GetCheckedOnline but lack the resources (including time and transportation) to do so, or are challenged by health system barriers in different parts of the process.6,26
The DHEF and UTAUT frameworks help further explain our findings, by demonstrating how users actively compare perceived benefits of digital STBBI testing (e.g. convenience and accessibility) with the effort (e.g. creating two online accounts, understanding GetCheckedOnline and associated laboratory systems) and resources required to use these services (e.g. travel and time requirements).22,27 Users who find the effort and resources required to access testing to be too high may not access testing despite positive perceptions of the comparative advantages of digital STBBI testing. 27 How information is received about GetCheckedOnline also plays a role in users’ capacity to complete testing. GetCheckedOnline has mainly relied on passive promotion through social circles (e.g. friends and family) over the past few years, and this inconsistent messaging may have increased expectations of ease of use and de-emphasized efforts required for testing. 27 Contrastingly, users who were recommended through HCPs were better prepared and more likely to test. Social influences therefore alter perceived efforts and expected benefits of using digital STBBI testing, and highlight reinforcement of structural inequities as current use of GetCheckedOnline may require social capital (either through friends and family or HCPs).27,29 From a systems perspective, this study suggests users’ assessments of the comparative benefits of digital STBBI testing services are often influenced by the resourcing and quality of in-person and digital STBBI testing services and its alignment with their needs in terms of access, timeliness, effectiveness, and safety. 22 Given prevalent challenges in accessing HCPs in BC, digital alternatives may appear effective, but only if they effectively remove access, resource, and other barriers experienced by users. This might not be true for some GetCheckedOnline users given its current model.
Our study points to gender norms in STBBI testing described in previous studies. Our findings that men can consider GetCheckedOnline mostly in concerned states while women may consider GetCheckedOnline in precautionary testing states, suggest both groups may have different educational needs. 29 As previously described in our work, these patterns emphasize notions of hegemonic masculinity (perceived men's robustness associated with healthcare avoidance) and emphasized femininity (views of women as sexual health caretakers) especially in heterosexual relationships.29,41 Findings also affirm the importance of sexual health education as part of digital STBBI testing interventions, consistent with other studies.42,43 While concerned testers require estimation of risks and potential next steps, precautionary testers might require STBBI prevention education and conditions for testing for various STBBIs.
Implications for research, policy, and practice
Our findings suggest that while GetCheckedOnline, and by extension other similar digital STBBI testing models, reduce barriers to testing, they do not achieve this goal for all groups. The significant effort still required to navigate different web systems and to access a physical laboratory may be a barrier especially for older, less experienced testers and residents of rural and remote communities. Findings suggest that to reduce missed opportunities on GetCheckedOnline, three main improvements may be considered. First, simplify the web interfaces to ensure seamless transition across websites. We acknowledge the GetCheckedOnline team's efforts to ensure seamless experiences, including integration of information packages on the website and including GetCheckedOnline laboratory search filters on partner laboratory websites.28,44 However, these efforts increase text on the website and significantly amplify users’ cognitive load, potentially worsening inequities as demonstrated by missed website features. 45 Potential solutions include reducing the need for user input. For example, custom search locators on partner websites that already integrate a GetCheckedOnline filter may reduce user errors. Further, ensuring laboratory appointment bookings through GetCheckedOnline may improve users’ experiences.
Second, STBBI education should be more customized to user contexts. Findings suggest that users consider GetCheckedOnline not only for testing, but for STBBI education.42,43 Therefore, integrating education features that are personalized to users’ contexts (i.e. in concerned or precautionary testing states) may empower them to make informed decisions about testing. For example, STBBI risk estimation might be needed for concerned testers while precautionary testers may need information about tests required in routine testing. Messaging about tests available through the service should consider highlighting what STBBIs should be routinely tested for, and which may be needed only in unique contexts as GetCheckedOnline currently covers routinely tested STBBIs. 46 Findings suggest generically framed messages about what tests are available may reinforce the sense that available tests are not comprehensive. While a link to a separate BCCDC sexual health education website is provided, 47 better integration between both services may improve user experiences and clarify misconceptions. Personalized education could also support users with less experience and digital literacy to access testing. For example, AI chatbots using natural language processing algorithms have been used to provide personalized humanoid support to help users access digital health services in other contexts. 48 However, these solutions may not work for everyone, and helplines with HCPs may bolster trust among users (e.g. recent immigrants).
Finally, provide more options for testing, including more physical laboratory locations or OPSS opportunities. Such options may empower residents in rural and remote communities especially those with lower socioeconomic status to access testing. Including additional laboratories in the network might address some challenges for rural and remote residents but may simultaneously perpetuate transition challenges already described. Including options for OPSS may be better aligned with users’ mental models of digital or “online” STBBI testing services. Aligning services to this mental model may help to reduce the burdensome nature of accessing physical testing locations and may better meet public expectations of digital health services given widespread digital transformation in society. 49 However, this alignment will require attention to jurisdictional legal and policy constraints, especially regarding restrictions on transporting biohazardous materials through public postal services. 50 While private alternatives exist, their costs may be a limitation. 51 Similar OPSS services are being piloted by the BC Cancer Agency for cervical cancer screening in remote communities, but sample requirements and policies on postal services for such samples may be different from our context.50,52 More research is required to understand which of these solutions most resonate with users and can potentially increase test completion on GetCheckedOnline. Research is also required to understand which solutions work best for various marginalized populations.
Strengths and limitations
First, we have described the novelty of this study's objective in exploring the role of web-design and implementation in access to digital STBBI testing using an intervention implemented at scale. Our theory-informed equity-centered approach to exploring these factors, combined with findings from our prior survey of clients creating accounts gives us in-depth understanding of how web design and implementation of GetCheckedOnline may lead to missed opportunities to provide digital STBBI testing. Moreover, critically examining GetCheckedOnline, as opposed to exploring characteristics of users, gives us important leverage points to adapt systems to promote testing equity for digital STBBI services. While the sample size was sufficient to explore identified themes, challenges with recruiting a diverse group of participants limits our capacity to make conclusions about equity especially by gender diversity, immigration, and income status, and with no recruitment of Indigenous and Black participants. Further research will be required to explore similarities and differences in the experiences of GetCheckedOnline in these sub-populations. Sampling limitations may represent inherent inequities in awareness of and access to GetCheckedOnline, as we sampled existing users experiencing missed opportunities. Sampling limitations may also be explained by documented difficulties recruiting users with negative experiences of health services. 53 Therefore, we have not outrightly emphasized results from the equity analysis, rather highlighting potential differences in experiences between groups while recommending further equity-focused research to understand how differences in the experiences of GetCheckedOnline among different populations may affect missed opportunities.
Conclusion
Our findings demonstrate significant challenges for users that lead to missed opportunities for digital STBBI testing interventions like GetCheckedOnline to provide testing and highlight the importance of adapting design and implementation features to suit users’ needs and contexts. Our study emphasizes issues related to web-design like interoperability challenges navigating between different websites and services for testing. It also highlights implementation issues that impose resource requirements to access a laboratory site that may still constitute a barrier especially for equity-seeking populations. Ensuring seamless transition between services through simplified web-design, ensuring education suited to users’ contexts, and integrating additional options for testing, including new laboratory locations and other digital STBBI testing models like OPSS, may ensure digital STBBI testing services are able to better provide access to testing, especially among equity-seeking populations.
Supplemental Material
sj-docx-2-dhj-10.1177_20552076241277653 - Supplemental material for Missed opportunities to provide sexually transmitted and blood-borne infections testing in British Columbia: An interpretive description of users’ experiences of Get Checked Online's design and implementation
Supplemental material, sj-docx-2-dhj-10.1177_20552076241277653 for Missed opportunities to provide sexually transmitted and blood-borne infections testing in British Columbia: An interpretive description of users’ experiences of Get Checked Online's design and implementation by Ihoghosa Iyamu, Rosemin Kassam, Catherine Worthington, Daniel Grace, Heather Pedersen, Devon Haag, Mark Bondyra, Amy Salmon, Mieke Koehoorn and Mark Gilbert in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076241277653 - Supplemental material for Missed opportunities to provide sexually transmitted and blood-borne infections testing in British Columbia: An interpretive description of users’ experiences of Get Checked Online's design and implementation
Supplemental material, sj-docx-3-dhj-10.1177_20552076241277653 for Missed opportunities to provide sexually transmitted and blood-borne infections testing in British Columbia: An interpretive description of users’ experiences of Get Checked Online's design and implementation by Ihoghosa Iyamu, Rosemin Kassam, Catherine Worthington, Daniel Grace, Heather Pedersen, Devon Haag, Mark Bondyra, Amy Salmon, Mieke Koehoorn and Mark Gilbert in DIGITAL HEALTH
Supplemental Material
sj-docx-4-dhj-10.1177_20552076241277653 - Supplemental material for Missed opportunities to provide sexually transmitted and blood-borne infections testing in British Columbia: An interpretive description of users’ experiences of Get Checked Online's design and implementation
Supplemental material, sj-docx-4-dhj-10.1177_20552076241277653 for Missed opportunities to provide sexually transmitted and blood-borne infections testing in British Columbia: An interpretive description of users’ experiences of Get Checked Online's design and implementation by Ihoghosa Iyamu, Rosemin Kassam, Catherine Worthington, Daniel Grace, Heather Pedersen, Devon Haag, Mark Bondyra, Amy Salmon, Mieke Koehoorn and Mark Gilbert in DIGITAL HEALTH
Supplemental Material
sj-pdf-5-dhj-10.1177_20552076241277653 - Supplemental material for Missed opportunities to provide sexually transmitted and blood-borne infections testing in British Columbia: An interpretive description of users’ experiences of Get Checked Online's design and implementation
Supplemental material, sj-pdf-5-dhj-10.1177_20552076241277653 for Missed opportunities to provide sexually transmitted and blood-borne infections testing in British Columbia: An interpretive description of users’ experiences of Get Checked Online's design and implementation by Ihoghosa Iyamu, Rosemin Kassam, Catherine Worthington, Daniel Grace, Heather Pedersen, Devon Haag, Mark Bondyra, Amy Salmon, Mieke Koehoorn and Mark Gilbert in DIGITAL HEALTH
Footnotes
Acknowledgements
We would like to thank GetCheckedOnline users who generously shared their time and experiences with us. We would also like to thank members of the BCCDC's Clinical Prevention Services—Sexual Health Advisory Board who reviewed study findings. Finally, we would like to acknowledge Hsiu-Ju Chang, the Digital and Sexual Health Initiative research manager who provided administrative support for ethics and participant recruitment.
Contributorship
II and MG conceived the study, II developed the study protocol with guidance from RK, AS, MK, and MG. II gained ethical approval, conducted participant recruitment, data collection, and analyses. II, HP, DH, CW, DG, and MG reviewed analyses and provided additional interpretation. II wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethics approval was obtained from the University of British Columbia's Behavioral Ethics Board (ethics #H22-03148).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This was supported by the Canadian Institute of Health Research (CIHR) [Implementation Science Team Grant: FR# CTW- 155387; PIs: MG, DG, CW] https://cihr-irsc.gc.ca/e/193.html. DG is supported by a Canada Research Chair in Sexual and Gender Minority Health https://www.chairs-chaires.gc.ca/home-accueil-eng.aspx. I.I is supported by the Canadian Institutes of Health Research (CIHR) Frederick Banting and Charles Best Doctoral Award (Grant number AWD-018949 CIHR 2021) (![]() ), the University of British Columbia Four Year Doctoral Fellowship (4YF) and the Bill Meekison Memorial Scholarship in Public Health.
), the University of British Columbia Four Year Doctoral Fellowship (4YF) and the Bill Meekison Memorial Scholarship in Public Health.
Guarantor
MG.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.