
Abstract
Background
Health-related social media is widely used for health information but has mixed effects on patient-provider relationships. The cognitive pathways through which health-related social media engagement shapes patients' perceptions of patient-centered communication (PCC) remain unclear.
Objective
Drawing on self-efficacy theory and theories of information behavior and adoption, this study examined two parallel mediators, the application of health information from social media (AHI) and online health information seeking self-efficacy (OHIS), in the association between the frequency of health-related social media engagement (HSME) and PCC among U.S. adults with chronic conditions.
Methods
This study was based on cross-sectional data from the 2022 Health Information National Trends Survey 6. The final sample included 3663 respondents who reported having at least one chronic condition and at least one hospital visit in the past year. Parallel mediation analyses were performed using Hayes' PROCESS macro (Model 4) in SPSS.
Results
HSME was negatively associated with PCC (β = -0.075, p < 0.001). HSME positively predicted AHI (β = 0.432, p < 0.001) and OHIS (β = 0.207, p < 0.001). AHI was negatively linked to PCC (β = -0.043, p < 0.05), whereas OHIS was positively linked to PCC (β = 0.141, p < 0.001). Significant indirect effects of HSME on PCC were found via AHI (effect = -0.019, 95% CI [-0.036, -0.002]) and via OHIS (effect = 0.029, 95% CI [0.020, 0.039]).
Conclusion
Findings highlight that while online information-seeking confidence is positively associated with PCC, direct reliance on health information obtained from social media is negatively associated with PCC. Understanding these pathways can help improve patient-doctor relationship.
Keywords
Introduction
In the United States, chronic diseases such as heart disease, diabetes, hypertension, and depression are highly prevalent. 1 In 2023, approximately 76.4% of U.S. adults, nearly 194 million individuals, reported having at least one chronic condition. 2 For individuals living with chronic illnesses, regular interaction with a healthcare system is critical. Effective communication with healthcare providers is essential for promoting self-management and better health outcomes for individuals with chronic conditions.3,4
In this context, perceived patient-centered communication (PCC) facilitates effective care. PCC is defined as a communication approach in which healthcare providers engage with patients to ensure that proposed care meets patients’ expectations, interests, and needs. 5 PCC emphasizes acknowledging the whole person, including their personality, life history, and social context, to develop a shared understanding of the problem, treatment goals, and potential barriers.5,6 By facilitating effective communication, PCC enhances patient trust in healthcare providers 7 and promotes self-care management, 4 thereby improving health outcomes.8,9 Previous studies have demonstrated that patients with multiple long-term conditions perceive more barriers and reported poorer hospital care experience than other patient groups.10,11 These findings highlight the urgent need to enhance PCC, particularly for individuals managing chronic diseases.
With the advancement of information and communication technologies, the rapid expansion of social media platforms has transformed how individuals access, share, and engage with health-related information, providing new opportunities for wider participation in health-related discussions.12–14 For patients with chronic conditions, activities such as sharing personal health information, connecting with others facing similar conditions, and participating in health-related discussions on social media serve as important avenues for acquiring both informational and emotional support. 15
However, prior research has produced mixed evidence regarding the relationship between health-related social media engagement (HSME) and patient–provider relationships as well as perceived PCC.16–18 When users encounter reliable health information sources, they tend to attend medical appointments better informed about their symptoms and treatment options. This preparation often leads them to ask more focused questions and feel more confident in seeking information, thereby enhancing communication with their healthcare providers.19,20 This pattern aligns with the self-efficacy theory, which posits that greater self-efficacy in acquiring information enhances patients’ ability to communicate effectively with providers, thereby improving their perceived PCC.
In contrast, exposure to misleading or contradictory online information may create uncertainty and undermine trust in clinicians and healthcare systems.21–23 As a result, physicians often spend additional time correcting misconceptions that patients have acquire from social media, which can disrupt the flow of clinical encounters. 24 Moreover, because social media can provide informational and emotional support for individuals with chronic conditions, highly educated patients may rely on online sources rather than their doctors, which may influence the quality of their clinical interactions. 25 Nevertheless, theories of information behavior and adoption 26 emphasize that mere exposure to online health information does not automatically lead to improved outcomes. Rather, engagement with social media can meaningfully shapes patient–provider communication when patients actively apply social media-based health information during decision-making 27 and clinical discussions. 28 Accordingly, the application of online health information can serve as a key mechanism linking health-related social media use to perceived PCC.
Building on this literature, two major research gaps can be identified. First, most existing studies have focused on the general population, with limited attention to individuals living with chronic conditions—a group that relies heavily on continuous medical care and frequently encounters barriers to effective patient–provider communication.18,29 To address this gap, we propose the following research question:
Second, although prior studies have documented mixed effects of HSME on perceived PCC, few have examined the underlying mechanisms that might account for these inconsistencies. Guided by self-efficacy theory and theories of information behavior and adoption, this study investigates whether patients’ application of health information from social media (AHI) and their online health information-seeking self-efficacy (OHIS) explain the association between HSME and PCC. Addressing this gap is crucial for designing interventions that leverage the benefits of social media while mitigating the spread of misinformation and the erosion of clinical relationships. Accordingly, we pose the following research question:
Literature review
Theoretical framework
Wilson's models of information-seeking behavior provide a comprehensive framework that links information needs, behaviors, and outcomes. His original model emphasized that needs arising from individuals’ roles and contexts may not lead to action because of various barriers. 30 Later revisions incorporated activating mechanisms and highlighted the dynamic interplay among needs, motivations, behaviors, and environment.26,31 Importantly, these models recognize that information processing and application are the critical stages in an information-seeking cycle. 26 Applied to health communication, Wilson's framework underscores that exposure to health information—such as content encountered on social media—does not automatically lead to improved outcomes. 32 Rather, recent empirical work on patients living with chronic conditions has extended Wilson's information-behavior model to digital health contexts, demonstrating that health information-seeking alone is insufficient and that the AHI are critical for health-behavior change.33,34 In this study, we therefore conceptualize AHI as a key mediator between HSME and PCC. Building on Wilson's models, we argue that AHI captures the depth of information integration, distinguishing it from mere exposure and offering a theoretically grounded pathway through which social media engagement may be associated with patients’ clinical interactions.
Theory of Self-Efficacy is a core component of Bandura's Social Cognitive Theory. 35 Self-efficacy is defined as an individual's belief in their ability to succeed in specific situations or accomplish tasks, which plays a key role in how they approach goals, tasks, and challenges. 36 Recent research in digital health highlights the central role of patients’ self-efficacy in shaping their engagement with online health information.37,38 Prior research has demonstrated that individuals with higher self-efficacy are more likely to actively seek, process, and apply health information.39,40 In this study, self-efficacy is operationalized as patients’ confidence in obtaining health information online, which allows them to understand and use this information more effectively. This increased confidence enables patients to participate actively in clinical interactions, ultimately improving their perceptions of PCC.
Hypothesis formulation
HSME is consistently linked to various forms of health information application, such as making health decisions or seeking preliminary information prior to consulting a healthcare professional.17,41 For instance, a cross-sectional survey found that while only one-fifth of social media users reported relying on health messages for decisions about family healthcare, nearly half admitted initiating medications based on social media content without physician consultation. 42 However, the information shared on social media—particularly concerning cancer, dental care, and diabetes—is often ambiguous or unverified, which requires professional verification before taking action. 43 Moreover, greater difficulty discerning credible content has been associated with increased odds of using social media information for health decisions and discussing it with healthcare providers. 44 Among people with chronic conditions, healthcare providers are also relied upon to filter social media-sourced information. 45 A recent survey of diabetic patients revealed that 70.9% had discussed social media-sourced health information during medical consultations. 46
Patients’ AHI can influence patient–provider relationships, such as perceived PCC. 47 Actively discussing online health information during consultations can empower patients and enhance collaboration with their healthcare providers. 48 However, many doctors feel overwhelmed when patients bring unverified social media content into consultations. 22 From the patient perspective, a focus group study by Rupert et al. 49 revealed that while patients viewed online health content as a valuable supplement to the information provided by their healthcare providers, many felt disempowered when clinicians reacted negatively to their questions about online health content. A recent study also found that some of the health professionals show negative attitudes toward the use of digital media. 50 Such dynamics can lead to potential conflicts and dissonance if healthcare providers disapprove of patients’ online health information-seeking behaviors. 18
Together, these findings suggest that although health information from social media can enrich patient knowledge, uncritical reliance on such information during consultations may compromise the quality and patient-centeredness of clinical communication. Based on this literature, we propose the following hypotheses:
OHIS refers to individuals’ confidence in using the internet effectively to access health-related information and has been associated with a higher frequency of healthcare visits.
51
Although few studies have directly examined how this self-efficacy shapes the relationship between HSME and perceived PCC, prior research indicates notable downstream effects.
16
A review has shown that users often experience anxiety and uncertainty during the initial stage of online health information-seeking, but gain confidence and clarity as the search progresses—a pattern consistent with a three-stage model of information-search behavior.
52
Engaging with health-related content on social media can make patients feel more empowered and assertive in medical decision-making,19,53 and this increased confidence fosters more balanced and participatory interactions with healthcare professionals.
54
For example, a study found that patients who used Facebook to learn about gestational trophoblastic disease (GTD) reported greater confidence in the information obtained online, expressed fewer doubts about GTD, and were less likely to perceive their clinicians’ explanations at diagnosis as inadequate.
55
Drowning on the reviewed literature, we propose the following hypotheses:
Method
Data source
This study drew upon data from the Health Information National Trends Survey 6 (HINTS 6), a cross-sectional, nationally representative survey conducted by the National Cancer Institute between March and November 2022. HINTS, which has been fielded regularly since 2004, is designed to assess health-related behaviors and attitudes among U.S. adults. 56 This study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement for cross-sectional studies to ensure methodological transparency and reporting rigor. The completed STROBE checklist is provided as Supplemental material. HINTS 6 employed a mail survey with a two-stage sampling process, consisting of (1) selecting addresses based on the U.S. sampling frame provided by the Marketing Systems Group and (2) randomly choosing one adult from each household. Of the 6252 completed surveys in HINTS 6, we included only those who reported at least one chronic condition (diabetes or high blood sugar/high blood pressure or hypertension/a heart condition/chronic lung disease/depression or an anxiety disorder), and who had at least one healthcare visit in the past 12 months. Applying these inclusion criteria resulted in a final analytic sample of 3663 participants. All analyses were weighted using the final person-level survey weights (PERSON_FINWT0) provided by HINTS to ensure nationally representative estimates. Variance estimation was conducted using the jackknife replication method with the 50 replicate weights provided by HINTS (PERSON_FINWT1–PERSON_FINWT50). Subpopulation analyses were implemented using a design-based approach by applying the inclusion criteria to the full replicate-weight survey design, rather than by restricting the dataset prior to estimation, to ensure that standard errors appropriately reflected the complex sampling design. Applying these inclusion criteria yielded a final analytic subpopulation of 3663 respondents. The resulting weighted analytic sample represented an estimated 134,042,743 U.S. adults with at least one chronic condition. The HINTS 6 survey was reviewed and approved by the Westat Institutional Review Board (IRB) as exempt research under 45 CFR 46.104 (Project no. 6632.03.51; approved on May 10, 2021; Amendment ID no. 3597, approved on November 24, 2021). The study also received a determination of Not Human Subjects Research from the NIH Office of IRB Operations on August 16, 2021 (iRIS reference number: 562715) (Figure 1).

Flow diagram of sample selection.
Measurement
For transparency and reproducibility, the original HINTS 6 variable names, coding schemes, and recoding procedures for all study variables are reported below and summarized in Supplemental Table S1.
The dependent variable, perceived patient-centered communication (PCC), 57 is defined as a communicative behavior that provides care in line with patients’ needs, values, and preferences, to improve active participant in their health decision-making. 58 In this study, PCC was measured as the mean of seven items, which are adapted from the NCI Monograph and recommended evaluation methods. 59 Participants were asked to reflect on their experiences with doctors, nurses, or other health professionals over the past 12 months and report how often each of the following occurred: (a) being given the chance to ask all the health-related questions they had; (b) receiving the attention they needed to their feelings and emotions; (c) being involved in decisions about their healthcare as much as they wanted; (d) being ensured that they understood the things they needed to do to take care of their health; (e) having things explained in a way they could understand; (f) having enough time spent with them; and (g) receiving help in deal with feelings of uncertainty about their health or healthcare. Responses for each item were rated on a 4-point Likert scale ranging from 1 (never) to 4 (always), with the scale demonstrating strong internal consistency (Cronbach's α = 0.93).
The independent variable, Frequency of health-related social media engagement (HSME), was defined as the actions individuals use social media to seek, share, and exchange health information. 41 It was computed as the mean score of four items. These items were drawn from previous research,60,61 measuring how often participants engaged in health-related activities on social media during the past 12 months: (a) sharing personal health information, (b) sharing general health-related information, (c) interacting with others who have similar health or medical issues, and (d) watching health-related videos. Responses were provided on a 5-point Likert scale ranging from 1 (never) to 5 (almost every day).12,13 The HSME composite scale showed good internal consistency (α = 0.87).
The first mediator, application of health information from social media (AHI), was operationalized as the mean of two items. 62 Participants rated their agreement with the statements “I use information from social media to make decisions about my health” and “I use information from social media in discussions with my healthcare provider” on a 4-point Likert scale (1 = strongly disagree to 4 = strongly agree). These two items were designed to capture two core dimensions of deep health information use: the internalization of information for personal health decision-making and its application in patient–provider communication. This operationalization aligns with the classic “Information Use” framework in health information behavior research. 62 The composite score reflects the extent to which participants integrate this information into their health decision-making and communication with providers. As the AHI construct was measured using two items, internal consistency was assessed using the Spearman–Brown coefficient, which indicated acceptable reliability (ρ = 0.57, p < 0.05).
The second mediator, online health information seeking self-efficacy (OHIS), an individual's confidence in their ability to locate and access helpful health information on the Internet when needed.63,64 It was assessed with a single item: “How confident are you that you can find helpful health resources on the Internet?” Responses were recorded on a 5-point Likert scale ranging from 1 (not confident at all) to 5 (completely confident). This item was adapted from validated measures of eHealth literacy and online health information-seeking confidence. 64 For example, the widely used eHealth Literacy Scale includes items such as “I know where to find helpful health resources on the Internet.” 64 Similarly, recent studies have employed single-item or brief measures of online health information-seeking confidence, demonstrating their predictive validity for digital health use and health behaviors.51,57 This item captures respondents’ belief in their ability to find and use online health information when needed.
In our analyses, we included five key sociodemographic covariates, including age, sex (0 = female, 1 = male), race/ethnicity (1 = non-Hispanic White, 2 = non-Hispanic Black, 3 = Hispanic, 4 = non-Hispanic Asian, and 5 = non-Hispanic Other), marital status (0 = single and 1 = non-single), education level (from 1 = less than 8 years to 7 = postgraduate); and household income (from 1 = less than $20,000 to 5 = $75,000 or more). These covariates were selected because, in the U.S. context, they are known to influence patients’ healthcare experiences, including perceived PCC. In addition, race/ethnicity was dummy coded before being included in the mediation models to ensure appropriate estimation.
Statistical methods
Data analysis was conducted in SPSS version 26. To ensure nationally representative estimates, all analyses were weighted using the final person-level survey weight (PERSON_FINWT0) provided by HINTS 6. These weights account for sampling probabilities and non-response, allowing population-level inference. First, bivariate Pearson correlations and a multicollinearity check were conducted to assess the relationships among perceived PCC, frequency of HSME, AHI, and OHIS. To test our hypothesized parallel mediation, we used Hayes’ PROCESS macro (Model 4) in SPSS, specifying AHI and OHIS as simultaneous mediators of the association between HSME and PCC. Indirect effects were evaluated using a bias-corrected bootstrap method with 5000 resamples, and effects were considered significant if their 95% confidence intervals (CIs) did not include zero. 65 The proportion of missing values varied across variables, ranging from 0.2% to 6.9%. For example, the variable marital status had 2.9% missing values, and the variable age had 1.0% missing values. This missing data arose from refused answer and non-ascertainment. We handled the missing values in this model using listwise deletion.
Result
Demographic and participants’ characteristics
As shown in Table 1, the analytic sample included 3663 adults with at least one chronic condition (unweighted N), representing 134,042,743 U.S. adults after applying the HINTS final survey weight (PERSON_FINWT0). The weighted mean age was 53 years. The proportion of females was 52.8%, compared with 45.7% for males. The sample was predominantly non-Hispanic White (63.1%). Regarding marital status, 54.2% of the respondents reported being non-single. Approximately 29.5% had completed college or higher, and 40.0% reported a household annual income greater than $75,000. All descriptive statistics were weighted to produce nationally representative estimates for U.S. adults with chronic conditions.
Descriptive statistics (unweighted N = 3663, weighted N = 134,042,743).

Relationships among key variables
Bivariate correlations among the continuous key variables are presented in Table 2. Significant associations were observed among frequency of HSME, AHI, OHIS, and perceived PCC, with correlation coefficients ranging from −0.094 to 0.125 (p < 0.01). Significant correlations between covariates including age (r = 0.126, p < 0.01), education (r = 0.026, p < 0.01), household income (r = 0.090, p < 0.01), marital status (r = 0.066, p < 0.01) and PCC were observed. Age, education, household income, and marital status were thus included as covariates in subsequent analyses.
Zero-order Pearson correlations (weighted N = 134,042,743).

PCC: patient-centered communication; HSME: health-related social media engagement; AHI: application of health information from social media; OHIS: online health information-seeking self-efficacy.
*p < 0.05; **p < 0.01; ***p < 0.001.
A multicollinearity check was conducted for the three key predictors (HSME, AHI, and OHIS) in the regression predicting PCC. Variance inflation factor values ranged from 1.054 to 1.193, well below the common cutoff of 10, tolerance values ranged from 0.083 to 0.949, the maximum condition index was 10.93 (OHIS), and no dimension showed multiple predictors with variance proportions exceeding 0.50, indicating that all three predictors can be considered independent without bias.
Mediation tests
As shown in Table 3 and Figure 2, a significant direct association was found between frequency of HSME and perceived PCC (β = −0.075, p < 0.001), addressing RQ1. In addition, HSME was positively associated with the AHI (β = 0.432, p < 0.001) and OHIS (β = 0.167, p < 0.001), supporting H1 and H4. Further, AHI was negatively associated with PCC (β = −0.044, p < 0.05), whereas OHIS was positively associated with PCC (β = 0.141, p < 0.001), supporting H2 and H5. The results also indicated significant indirect effects of HSME on PCC through both AHI (β = −0.019, 95% CI [−0.036, −0.002]) and OHIS (β = 0.023, 95% CI [0.015, 0.033]), supporting H3 and H6. In the parallel mediation model including HSME, AHI, and OHIS, the outcome model explained 8% of the variance in PCC (R2 = 0.08, p < 0.001). Although the variance explained by the model was modest, the use of a large, nationally representative sample from HINTS enhanced the generalizability and robustness of the findings. Together, these findings demonstrate that AHI and OHIS serve as opposing mediators in the relationship between HSME and PCC, thereby addressing RQ2.
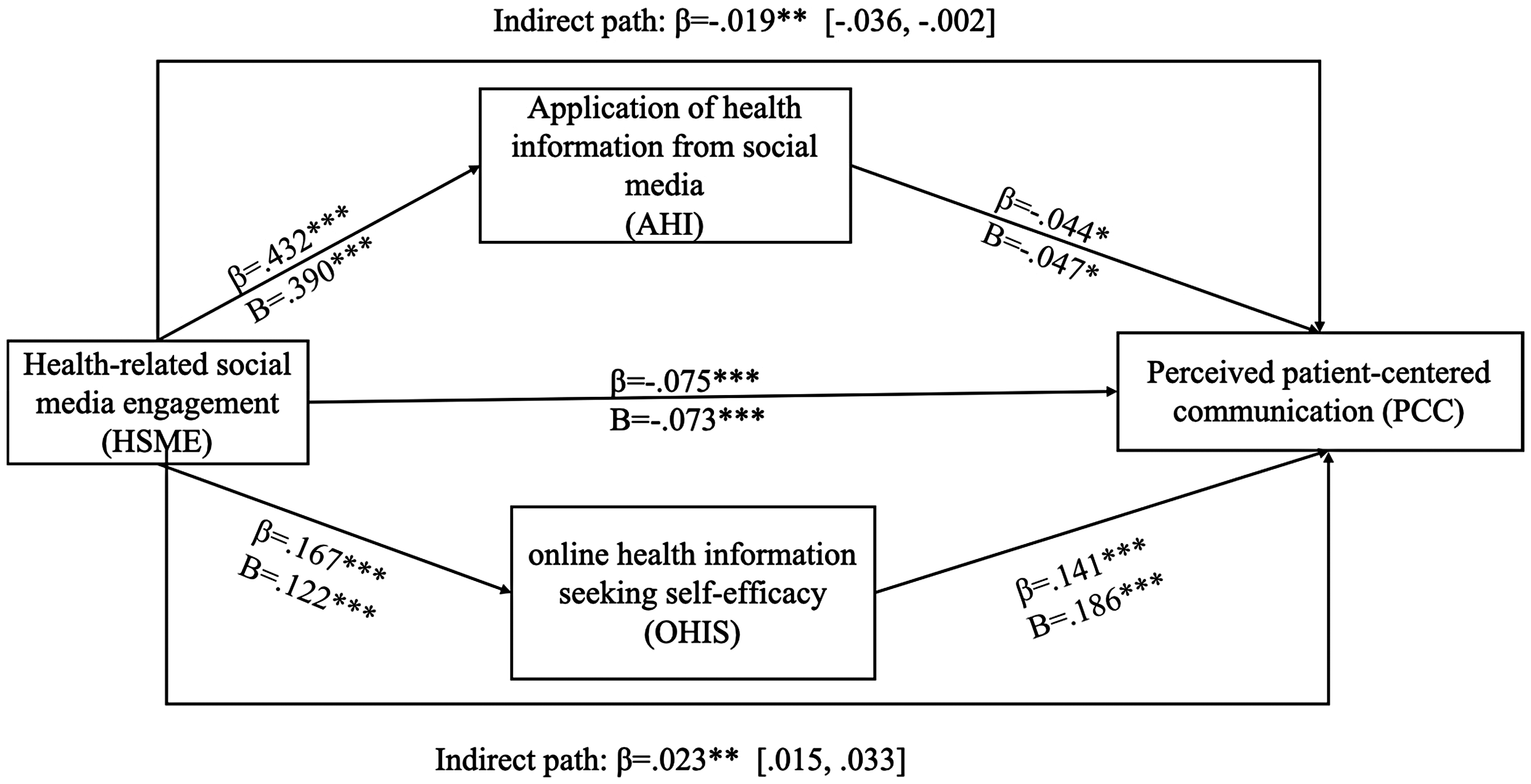
The results of mediation analysis. Note: *p < 0.05; **p < 0.01; ***p < 0.001.
Summary of mediation effects from regression models adjusted for sociodemographic covariates (weighted N = 134,042,743).

B: unstandardized coefficients; β: standardized beta; SE: standard error; CI: confidence interval; PCC: patient-centered communication; HSME: health-related social media engagement; AHI: application of health information from social media; OHIS: online health information-seeking self-efficacy; LLCI: lower limit confidence interval; ULCI: upper limit confidence interval.
All models controlling for age, gender, marital status, education, annual household income, and race/ethnicity.
*p < 0.05; **p < 0.01; ***p < 0.001.
Discussion
This study examined the patterns of association between HSME and perceived PCC among individuals with chronic conditions. These contrasting pathways highlight the complex and dual-edged role of social media in relation to patient–provider interactions and illustrate the relevance of self-efficacy theory and theories of information behavior and adoption in the context of health information acquisition and medical consultation.
The negatively direct impact from HSME and PCC
The findings showed a significant negative direct association between HSME and PCC, suggesting that although social media is increasingly used as a tool for health engagement, it may sometimes hinder effective communication with healthcare providers. This result aligns with previous studies reporting that patients’ acquisition of online health information can complicate patient–provider communication.16,17,66 On the one hand, social media use for health purposes has been associated with different dynamics of clinical encounters. 67 On the other hand, healthcare providers often express skepticism or resistance toward patient-sourced online information, which may lead to relational tension during consultations. 47 For instance, Broom 24 in an in-depth interview study with medical specialists reported that physicians felt patients were unable to assess the quality of information found online. Many physicians perceived the introduction of internet-based materials as a challenge to their professional authority and as an unnecessary burden during clinical interactions. Additionally, recent research indicates that exposure to perceived misinformation on social media has been linked to lower patient trust. 68 Evidence suggests that patients may encounter large amounts of misleading information on social media, which may be linked to challenges in establishing trust in their physicians. 69 In addition, social media may foster overconfidence in self-diagnosis, thereby associated with lower reliance on professional medical advice. 47 Other studies have highlighted information overload as another significant mediator. Information overload has been shown to associate with greater patients’ anxiety and confusion, often leading them to present fragmented or contradictory questions during consultations.70,71 This, in turn, is associated with lower communication efficiency, and may co-occur with defensive responses, which, in turn, is related to lower perceived experience of PCC.70,72,73 In addition, this negative association may differ across patient groups. Patients with higher health literacy may be better able to evaluate and discuss online information without undermining communication, 74 whereas those with more complex chronic conditions, such as multimorbidity, often face competing information demands that may complicate clinical interaction. 75 Sociodemographic factors, including age and education, have also been linked to differences in online health information use and communication expectations, suggesting potential moderating effects on the relationship between HSME and PCC.76–78 These variations warrant further investigation to identify patient groups most susceptible to negative communication experiences related to social media use.
Based on these references, prior studies have primarily examined how physicians respond to or incorporate online health information, with a focus on its impact on the patient–provider relationship. 47 This study provides a new perspective by assessing the associations between information use and OHIS in a mediation analysis. This dual-pathway framework emphasizes the patient's role, particularly highlighting the association between their confidence in using social media health content and perceived PCC. The association between social media use and PCC is not uniformly negative; rather, it appears to be linked to two distinct psychological and behavioral pathways. One pathway is characterized by patterns that coincide with challenges in communication (related to the application of health information), while the other is characterized by patterns associated with more favorable communication dynamics (linked to greater confidence in information-seeking). The following section examines these contrasting mediating pathways, which help explain the mixed findings in the literature and underscore the dual-edged nature of social media in clinical encounters.
Mediation effect of information application and information self-efficacy
As the use of social media for health purposes can produce mixed outcomes in the patient–provider relationship, it is essential to explore the mechanisms underlying this process. This study identified two distinct mediating pathways. First, the AHI was observed as a negative indirect pathway, reflecting a statistical association between the use of unverified or conflicting online content and lower perceived communication quality and trust. In contrast, OHIS appeared as a positive indirect pathway, showing a statistical association between patients’ confidence in accessing and evaluating online health information and perceived PCC. Although these mediation effects were statistically significant, the overall proportion of variance explained in perceived PCC was modest. This indicates that the mechanisms identified here represent only a limited part of the broader determinants of clinical communication. Nevertheless, situated within the wider context of contemporary digital health practices, these findings offer meaningful insight into how social media-related information behaviors may shape patients’ perceptions of communication in clinical encounters.
The significant mediation effect of AHI between HSME and PCC is consistent with theoretical perspectives in information behavior and adoption of Wilson's framework, suggesting a pattern in which information application is relevant to patients’ health information acquisition processes.26,32,34,79 Although information behavior and adoption theories help contextualize patients’ engagement with online content, they do not fully address how patients cope with conflicting information during medical encounters. The negative results observed in this indirect pathway can be explained through cognitive dissonance theory (CDT). 80 According to CDT, individuals strive to maintain internal consistency, and when their cognitions or beliefs conflict, they experience psychological discomfort.81,82 In the current study, when patients encounter inconsistencies between information obtained from social media and advice from healthcare professionals, they may experience cognitive dissonance and the associated psychological discomfort. This psychological discomfort manifests as questioning, 83 defensiveness, 84 anxiety, 85 embarrassment, 85 distrust toward the physician, 86 or withdrawal from the clinical interaction. For instance, research indicates that misinformation on social media can lead to confusion, 83 and patients may regard this conflict as evidence of intentional bias and professional incompetence, 83 which increases their mistrust in healthcare, further complicating the therapeutic alliance.83,87 Moreover, evidence suggests that information overload and uncertainty regarding online health information sources increase the likelihood that patients ask fragmented or contradictory questions during consultations, thereby reducing the efficiency of patient–provider communication. 88 Thus, CDT aligns with a broader theoretical framework by clarifying how the evaluation and application of online information may coincide with less positive perceptions of PCC.
The positive mediation effect of OHIS further supports the application of self-efficacy theory in digital health use and patient–provider relationship. 36 Recent studies in digital health highlight that patients with higher OHIS are more likely to engage in meaningful discussions with clinicians and participate in shared decision-making, reinforcing PCC.37,89 Previous studies have shown that information-seeking self-efficacy can help improve patients’ health management,90,91 and this study points out its positive association with patients’ perceived PCC. After engaging with health-related social media, patients not only receive emotional and informational support from online communities but also experience increased mastery experiences and vicarious learning, which bolster their confidence in finding and evaluating health information.15,52 With this enhanced self-efficacy, patients are more inclined to articulate their health concerns and treatment preferences clearly, which lays a foundation for meaningful exchanges. 92 In addition, stronger self-efficacy encourages patients to participate more actively in shared decision-making. Evidence from patients with systemic lupus erythematosus showed that frequent online health information-seeking was positively associated with higher shared decision-making scores, indicating that such retrieval behaviors can foster more active participation in clinical encounters. 93 Furthermore, a quasi-experimental study involving older adults managing hypertension found that computer-assisted information retrieval significantly increased decision self-efficacy, suggesting that structured strategies, such as preparing question lists or reviewing online materials before consultations, may strengthen recall and follow-up. 94 These active engagements shift the clinical encounter from a one-way transfer of information to a two-way exchange, thereby reinforcing the core elements of PCC.
Taken together, these dual-mediation pathways offer a nuanced interpretive framework for understanding the inconsistent findings in the literature on social media and healthcare communication. One pathway, linking HSME, AHI, and PCC, is commonly situated within a risk-oriented narrative and is characterized by patterns of information application that coincide with cognitive tension and less favorable communication experiences, consistent with perspectives on cognitive dissonance. The other pathway, connecting HSME, OHIS, and PCC, aligns with an empowerment-oriented narrative, marked by greater confidence in information evaluation and information-seeking, resonating with self-efficacy-based perspectives on patient engagement and shared decision-making. Viewed together, these pathways reflect distinct but coexisting theoretical orientations through which social media-related experiences are associated with variation in patients’ perceptions of care. Beyond the identified pathways, it is important to recognize that PCC is inherently complex and shaped by multiple relational, organizational, and systemic factors. While this study focuses on social media-related informational and cognitive mechanisms, many determinants of clinical communication fall outside the scope of the present model. These findings should therefore be understood as illuminating one dimension of a multifaceted communicative process rather than providing a comprehensive explanation.
The practical implications
The diametrically opposed mediating roles of health information use and online information-seeking self-efficacy in our model provide several actionable insights. Although online communities have become vital sources of support for patients with chronic illnesses,15,18 they frequently host low-quality or misleading information. 95 Social media platforms should assume responsibility for the quality of health content by partnering with reputable medical organizations, implementing rigorous fact-checking processes, and clearly labeling evidence-based resources. In addition, healthcare professionals can play an active role in online health information fact-checking. For example, by establishing verified physician accounts on short-video platforms and providing evidence-based health education, clinicians can leverage their professional credibility to counteract the decline in trust toward medical professionals that often arises from information overload.69,96
Second, given the positive mediating role of information-seeking self-efficacy in enhancing PCC, healthcare systems and patient advocacy groups should prioritize eHealth literacy initiatives, such as interactive online tutorials, community workshops, and peer-guided forums, which can strengthen patients’ abilities to critically evaluate digital health information and bolster their confidence in finding and applying accurate resources. 97 Furthermore, in response to the informed questioning from patients resulting from increased information-seeking self-efficacy, physicians should first affirm this proactive behavior, then employ structured responses involving empathic validation, clarification of medical information, and summarization of the patients’ articulated concerns to ensure mutual understanding. 98 In addition, to leverage the enhanced patient engagement in health decision-making resulting from increased self-efficacy, clinicians should explicitly invite patients to express their preferences and utilize International Patient Decision Aid Standards (IPDAS) to present options neutrally. 99 Adopting a collaborative consultation style helps integrate medical evidence with patient values to reach mutually agreed-upon treatment plans. 99
Finally, clinicians must acknowledge the growing impact of social media on patient expectations and approach online-informed questions with openness and patience, transforming potential conflicts into collaborative opportunities. 18 Healthcare providers should actively ask patients about their information sources to understand how they access health content and, where necessary, correct misinformation with evidence-based explanations. 100 During consultations, providers can employ the teach-back method, inviting patients to restate information in their own words to verify comprehension and address potential misunderstandings. 101 Additionally, providers should pay attention to patients’ emotional responses, offering appropriate support to alleviate anxiety or embarrassment arising from conflicting information. 102 Furthermore, implementing feedback systems can enable providers to identify potential biases or gaps in their communication practices, promoting reflective learning and continuous improvement in PCC. 103 In this way, clinicians help initiate a virtuous cycle: high-quality online content increases patient self-efficacy, improves consultation preparedness, and ultimately strengthens the patient–provider partnership.
Limitation
Several limitations should be acknowledged in this study. First, the cross-sectional design precludes any inference of causality among social media use, mediators, and PCC. Second, using a public database and conducting secondary analysis introduces limitations in variable measurement. For example, OHIS was measured using a single-item scale. While single-item measures are sometimes employed in large surveys, they inherently limit the ability to assess construct validity and internal consistency. This limitation should be considered when interpreting the mediation results. Future research could employ multi-item scales to provide more reliable and comprehensive assessments of psychological constructs. Third, the study did not assess the objective quality or veracity of the social media content accessed by patients, nor did it capture providers’ perspectives on specific information sources. While our measure of HSME captures both health-related content (e.g. lifestyle tips such as healthy eating or stress management) and health-related information (e.g. advice on disease prevention, diagnoses, or therapies), and the distribution of items suggests a stronger orientation toward health-related information. However, the questionnaire did not provide specific examples, so the responses may have encompassed a broad range of health information and content but lacked clarity. This overlap may limit our ability to disentangle the potentially different effects of exposure to general health content versus more specific medical information. Future studies should incorporate assessments of content quality and source credibility, as well as employ more fine-grained measures that differentiate between general content and specific information. Fourth, it is worth noting that this study focused on U.S. adults with chronic conditions who had at least one hospital visit in the past year. The sample was older (around 53 years), predominantly female (52.8%), and mostly non-Hispanic White (63.1%). As such, the findings may be most applicable to this specific subset of patients with chronic conditions and may not fully generalize to younger adults, more racially and ethnically groups, patients managing chronic conditions outside hospital settings, or those with acute conditions. Social media use, health literacy, and patient–provider interactions may vary across these populations. Future research should replicate and extend the dual-pathway model in more diverse cohorts to assess its broader applicability and inform interventions tailored to different demographic and healthcare contexts. Finally, although demographic variables (age, education, and ethnicity) were included as controls, this study did not examine whether the association between HSME and PCC varies across different chronic conditions or sociodemographic subgroups. Future research could explore these potential differences to better understand how patient characteristics relate to patterns of social media use and perceived communication quality.
Conclusion
In summary, this study highlights the dual-edged nature of health-related social media use in relation to patient–provider communication, suggesting two possible explanatory pathways. Reliance on unverified social media information was associated with lower perceived patient-centered communication, aligning with patterns described by cognitive dissonance processes. In contrast, greater OHIS was associated with more equitable, participatory dialogue. These findings contribute to theoretical development by extending self-efficacy theory and theories of information behavior and adoption to the digital health context, while also offering actionable guidance for platforms, patients, and clinicians. Future longitudinal and experimental research should further investigate these pathways across diverse patient populations and examine interventions aimed at strengthening patients’ digital skills and confidence in evaluating and applying online health information, with the broader goal of enhancing patient-centered communication in an increasingly connected world.
Supplemental Material
sj-xlsx-1-dhj-10.1177_20552076261425323 - Supplemental material for Exploring the associations between social media engagement and patient-centered communication among chronic disease patients: The mediating roles of information application and self-efficacy
Supplemental material, sj-xlsx-1-dhj-10.1177_20552076261425323 for Exploring the associations between social media engagement and patient-centered communication among chronic disease patients: The mediating roles of information application and self-efficacy by Zun Jiao and Xiaorong Yu in DIGITAL HEALTH
Supplemental Material
sj-doc-2-dhj-10.1177_20552076261425323 - Supplemental material for Exploring the associations between social media engagement and patient-centered communication among chronic disease patients: The mediating roles of information application and self-efficacy
Supplemental material, sj-doc-2-dhj-10.1177_20552076261425323 for Exploring the associations between social media engagement and patient-centered communication among chronic disease patients: The mediating roles of information application and self-efficacy by Zun Jiao and Xiaorong Yu in DIGITAL HEALTH
Footnotes
Ethical considerations and consent to participate
The HINTS 6 general population survey was designated “exempt research” under 45 CFR 46.104 and approved by the Westat IRB on May 10, 2021 (Project no. 6632.03.51), with a subsequent amendment approved on November 24, 2021 (Amendment ID no. 3597). HINTS 6 also received a “Not Human Subjects Research” determination from the NIH Office of IRB Operations on August 16, 2021 (iRIS reference number: 562715).
Author contributions
Zun Jiao conceptualized the study and wrote the original draft of the manuscript. Xiaorong Yu conceived the model idea and provided guidance throughout the manuscript writing process.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.