
Abstract
Aim
This study aims to systematically integrate the evidence based on meta-analysis of the efficacy of virtual reality on depressive symptoms in various populations.
Methods
We systematically searched PubMed, Web of Science, Embase, Cochrane Library, PsycINFO, and Chinese databases (CNKI, Wanfang Data, VIP) from inception to December 31, 2024. This study used an evidence map approach to integrate the included meta-analyses, to assess the effectiveness of virtual reality in treating depression, and to explore the impact of different groups and intervention characteristics on efficacy.
Results
A total of 27 meta-analyses were included, from which 33 outcomes were extracted for analysis. The quality assessment revealed that a significant majority of these outcomes (69.70%, 23/33) stemmed from MAs classified as low or critically low quality. The bubble chart indicated that the majority (75.8%, 25/33) supported the beneficial impact of virtual reality in improving depressive symptoms. These meta-analyses encompassed 129 independent original studies involving 6639 participants across multiple diverse populations. Positive effects were observed for populations with chronic non-neoplastic diseases, cancer, degenerative diseases, cognitive impairment, and those in special care scenarios. However, the effect on patients with mental and psychological disorders remains unclear.
Conclusion
Virtual reality interventions represent a promising approach in improving depressive symptoms, particularly in settings where conventional therapies are difficult to implement. Future research should focus on accumulating high-quality evidence and encompass a broader range of individuals at high risk of depression to enhance the generalizability of virtual reality applications in managing depression.
Introduction
Depression, one of the most common psychiatric disorders, has affected more than 300 million people globally, imposing substantial suffering on patients and families along with a heavy economic burden. 1 Notably, the incidence of depressive symptoms is particularly pronounced among patients with chronic systemic diseases that include cardiovascular disease, stroke, cancer, diabetes, and chronic pain. 2 Research indicates that 20–40% of patients with cardiovascular disease experience significant depressive symptoms, 3 while the prevalence among diabetic patients is approximately 31%. 4 Furthermore, depressive symptoms are highly prevalent among cancer patients, especially those with lung cancer, affecting approximately 44% of individuals. 5 The primary characteristics of depressive symptoms include persistent low mood, reduced interest in activities, fatigue, and feelings of worthlessness. 6 These symptoms not only reduce patients’ quality of life and adherence to treatment,7,8 but may also exacerbate the underlying medical conditions through mechanisms such as neuroendocrine dysregulation and chronic inflammatory responses, 9 in addition to being linked to increased all-cause mortality. 10
Both antidepressant medications and psychological therapies have demonstrated efficacy in the treatment of depression. 11 However, psychotherapy has become the preferred choice among patients, primarily due to apprehensions regarding the side effects associated with pharmacological treatments and individual patient preferences.12,13 Among the various psychological approaches, cognitive behavioral therapy (CBT) is recognized as one of the most widely used and empirically supported approaches.14,15 Nevertheless, the complexity of the therapeutic process, the dependence of its therapeutic effect on the therapist's expertise and the patient's compliance,16,17 as well as the financial implications, have hindered its widespread implementation. 18 Therefore, it is crucial to explore more accessible and cost-effective alternatives.
In this context, virtual reality (VR) is emerging as an innovative digital technology tool garnering increasing attention. 19 By generating computer-simulated immersive environments, VR provides multisensory stimulation and interactive experiences that aid in diverting attention from negative stimuli. 20 This capability also evokes positive emotional experiences, 21 thereby directly addressing the pleasure deficiency often associated with depression. 22 As technological advancements continue and costs decrease, VR is becoming more popular among diverse populations. 23 Multiple meta-analyses (MAs) have demonstrated significant effects of VR interventions in reducing depressive symptoms among individuals with cardiovascular disease, 24 Parkinson's disease, 25 anxiety disorders, 26 and cancer. 27 Nonetheless, some studies have failed to confirm its efficacy in patients with cancer and anxiety disorders.28,29 This inconsistency may stem from variations in participant characteristics, types of VR employed, and study designs,28,30,31 leading to substantial heterogeneity within MAs and undermining the reliability of efficacy evaluations.
Given the variability in contemporary research findings and the fragmentation of existing evidence, there is a pressing need to systematically consolidate the evidence regarding the efficacy of VR interventions systematically. This study therefore employs an evidence map to systematically synthesize findings from relevant meta-analyses, evaluate the efficacy of VR interventions in improving depressive symptoms across diverse populations, and identify key evidence gaps to inform future research directions and clinical practice.
Materials and methods
The evidence synthesis adheres to the methodological standards of a comprehensive overview, mirroring the structure of an umbrella review. 32 This investigation was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines and the Cochrane Handbook for Systematic Reviews of Interventions. The study protocol has been registered with PROSPERO (CRD420251014626).
Search strategy
A systematic search of PubMed, Web of Science, Embase, Cochrane Library, PsycINFO, and three major Chinese databases (CNKI, VIP, and Wanfang Data) was performed from inception to December 31, 2024. A comprehensive search strategy, incorporating both subject headings and free words, was implemented across these databases. Search terms encompassed “virtual reality,” “virtual reality therapy,” “virtual reality interventions,” “virtual reality scene,” “VR,” “depression,” “depress*,” “depressive disorder*,” “melanchol*,” “dysthymic disorder,” “affective symptoms”. Furthermore, a manual search of reference lists from potentially relevant articles was conducted to identify additional eligible studies. The detailed search strategy is available in Supplemental File 1a.
Eligibility criteria
Study selection was governed by the following criteria. Inclusion required that studies: (1) involve any population; (2) utilize a VR intervention; (3) employ a non-VR control group for comparison; (4) report outcomes on depressive symptoms; and (5) be a systematic review with quantitative meta-analysis.
Conversely, studies were excluded if they were: (1) non-peer-reviewed publications (e.g., clinical opinions, protocols, or conference abstracts); (2) duplicate publications or those with data insufficient for extraction; (3) unavailable as a full text; or (4) published in languages other than Chinese or English.
Study selection and data extraction
After importing all records into EndNote21 and removing duplicates, two investigators independently screened the literature according to the pre-specified inclusion and exclusion criteria. Any discrepancies encountered were resolved through consultation with a third researcher. The following data points were extracted: first author, publication year, country of origin (first author), type of study included, population condition, type of VR, number of studies included, sample size, effect size and 95% confidence intervals (95% CIs).
Furthermore, the original study data from the MAs were integrated. Specifically, all original studies were initially compiled into a comprehensive list, and duplicates were eliminated by manual cross-validation of titles, authors, publication years, population characteristics, and sample sizes to ensure each participant was only counted once. After data extraction was completed, another researcher checked to ensure data accuracy.
Quality assessment
Two independent evaluators assessed the methodological quality of all included MAs. The assessment utilized the Assessment of Multiple Systematic Reviews (AMSTAR-2) tool, which comprises 16 items. Among these, items 2, 4, 7, 9, 11, 13, and 15 are designated as critical, while the remaining items are classified as non-critical. The overall methodological quality was subsequently categorized as high, moderate, low, or critically low, based on the presence of critical and non-critical deficiencies. 33 Any disagreements were resolved by consensus or by consulting a third researcher.
Statistical analysis and visualization
Publication trends of original research
The annual distribution of the number of independent original studies was visualized using a line graph in Microsoft Office Excel, with the year on the X-axis and the number of studies on the Y-axis.
Population classification
The study population was classified into five primary groups, determined by the predominant pathophysiological or clinical features of health conditions, as well as the specific requirements of VR interventions. The identified groups comprised chronic non-neoplastic organic diseases, degenerative diseases and cognitive disorders, mental and psychological disorders, cancer, and special care scenarios. Data on population characteristics and sample sizes were extracted from the independent original studies within the included meta-analyses. These data were then organized into the above categories and visualized using a Sankey diagram, generated with Origin 2024 software.
Effectiveness of virtual reality to improve depression
The efficacy of VR in alleviating depression was illustrated using bubble plots generated with Origin 2024. Each bubble represents a single, independent effect size estimate. To explore heterogeneity, subgroup estimates were preferentially included over overall pooled estimates when available.
The bubble plots integrate multiple data dimensions:
X-axis: Interventions were categorized as “Effective,” “Potentially effective,” or “Unclear” based on statistical significance and effect direction (detailed criteria are provided in Supplemental File 1b). Y-axis: Alternates between AMSTAR-2 rated methodological quality (“High,” “Moderate,” “Low,” or “Critically low”), or the type of VR categorized based on degree of immersion (“Fully immersive,” “Non-fully immersive,” or “Any type”), whose definitions are detailed in Supplemental File 1c. Bubble Attributes: Size represents the aggregate sample size; the internal number denotes the number of original studies included, with an asterisk (*) indicating the presence of an active control group (e.g., CBT, mental imagery relaxation therapy); color corresponds to the population classification.
Results
Literature screening process and results
A total of 4418 studies were initially identified during the literature search. After removing duplicates, 3043 studies remained for further review. Following a screening of titles and abstracts, 2803 studies were excluded. A detailed evaluation of the full texts for 240 studies was then conducted, and ultimately 27 MAs were included. (Figure 1)

Literature screening process.
Characteristics of the included MAs
A total of 27 MAs were incorporated into this investigation, encompassing 4 published in Chinese25,31,34,35 and 23 in English.24,26–29,36–53 The publications spanned from 2014 to 2025, with only 2 articles published before 2020.37,38 Of these, 26 MAs exclusively analyzed randomized controlled trials (RCTs),24–29,31,34–50,52,53 while 1 MA also included quasi-experimental studies. 51 The number of constituent studies within each MA ranged from 2 to 17, with corresponding sample sizes ranging from 49 to 1076 participants. Regarding the type of VR, 10 studies focused on fully immersive VR,24,27–29,37,38,43,47,51,52 6 on non-fully immersive,25,39–41,46,48 and 11 encompassed any type.26,31,34–36,42,44,45,49,50,53 (Table 1).
Characteristics of included MAs.

Abbreviations:RCT = Randomized Clinical Trial, Q-Exp = Quasi-Experimental Study, TAU = Treatment As Usual, WL = Waitlist, SSD = Schizophrenia Spectrum Disorder , PD = Parkinson's Disease, PTSD = Post-Traumatic Stress Disorder, MS = Multiple sclerosis, COPD = Chronic Obstructive Pulmonary Disease, AMI = Acute Myocardial Infarction, CVD = Cardiovascular Disease, CHF = Chronic Heart Failure, PICS = Post-Intensive Care Syndrome, CHD = Coronary Heart Disease, CAD = Coronary Artery Disease, FMS = Fibromyalgia Syndrome, GAD = Generalised Anxiety Disorder, SAD = Social Anxiety Disorder., Effects with * indicate reversal of sign.
Methodological quality assessment of included mas
The methodological quality of the included MAs was assessed using the AMSTAR2 tool. The assessment revealed that among 27 included MAs, 2 studies24,36 were classified as high quality, 440,41,49,52 as moderate, 1126,27,29,39,42,44,45,47,48,50,53 as low and 1025,28,31,34,35,37,38,43,46,51 as critically low. Specifically, of the 16 AMSTAR2 items, full compliance was less than 50% for item 4 (comprehensive literature search strategy), item 7 (complete list of excluded studies included), item 10 (funding sources of included studies), and item 13 (risk of bias in included studies), which indicates significant deficiencies in these areas. In addition, 13 MAs (48%) did not explain the reasons for the type of study included (item 3), and publication bias was not adequately investigated and discussed (item 15). (Figure 2; detailed study-specific evaluations are presented in Supplemental File 1d.)

Assessment of the methodological quality of the included MAs.
Publication trends of independent original research
This analysis ranked the original studies in the included MAs separately, and the findings revealed that the 27 MAs covered 129 independent original studies (125 RCTs, 4 Q-Exp) with a cumulative sample size of 6639 people. Of these, 22 original studies were duplicated across the included MAs, with 3 studies being re-included twice. (Processes are described in Supplementary File 2). Among 129 independent original studies, 57.4% (74/129) were published in 2020 or later, with a peak in 2020 (20.9%,27/129). However, there has been a decline in the number of studies published each subsequent year. (Figure 3)

Original studies including MAs publication trends.
Population classification and its distribution
Based on an analysis of 129 original studies, the population was divided into 5 distinct groups based on disease characteristics and VR intervention requirements. The largest group comprised individuals with chronic non-neoplastic organic diseases (hereinafter denoted as “chronic diseases”), which accounted for 37.31% of the population and included cerebrovascular diseases (17.89%) and cardiovascular diseases (15.94%), such as coronary heart disease, hypertension, myocardial infarction, and valvular disease. The second category comprised mental and psychological disorders (hereinafter denoted as “mental disorders”), representing 21.28% of the population. The third category is degenerative diseases and cognitive impairment (18.06%), the fourth category is special care scenarios (13.84%), and lastly, cancer patients (9.50%). (Figure 4)

Population classification and its distribution.
The effectiveness of VR interventions in the depression treatment
Bubble plots were used to visualize findings from 33 study outcomes derived from the 27 included MAs. These plots illustrate the associations between the methodological quality of the MAs, the type of VR, and control conditions with depression outcomes.
Effectiveness distribution based on AMSTAR-2
Figure 5 presents a bubble chart visualization of 33 study outcomes, integrating quality assessment results, the effectiveness of VR intervention for depression, and population information. The quality assessment revealed that a significant majority of these outcomes (69.70%, 23/33) stemmed from MAs classified as low or critically low quality, while only 30.30% (10/33) were from moderate to high-quality MAs. Despite the variability in study quality, the majority of research concluded that VR intervention has a positive effect on alleviating symptoms of depression. 66.67% (22/33) of the studies considered VR intervention for depression as effective, 9.09% (3/33) as potentially effective, and 24.24% (8/33) were unclear.
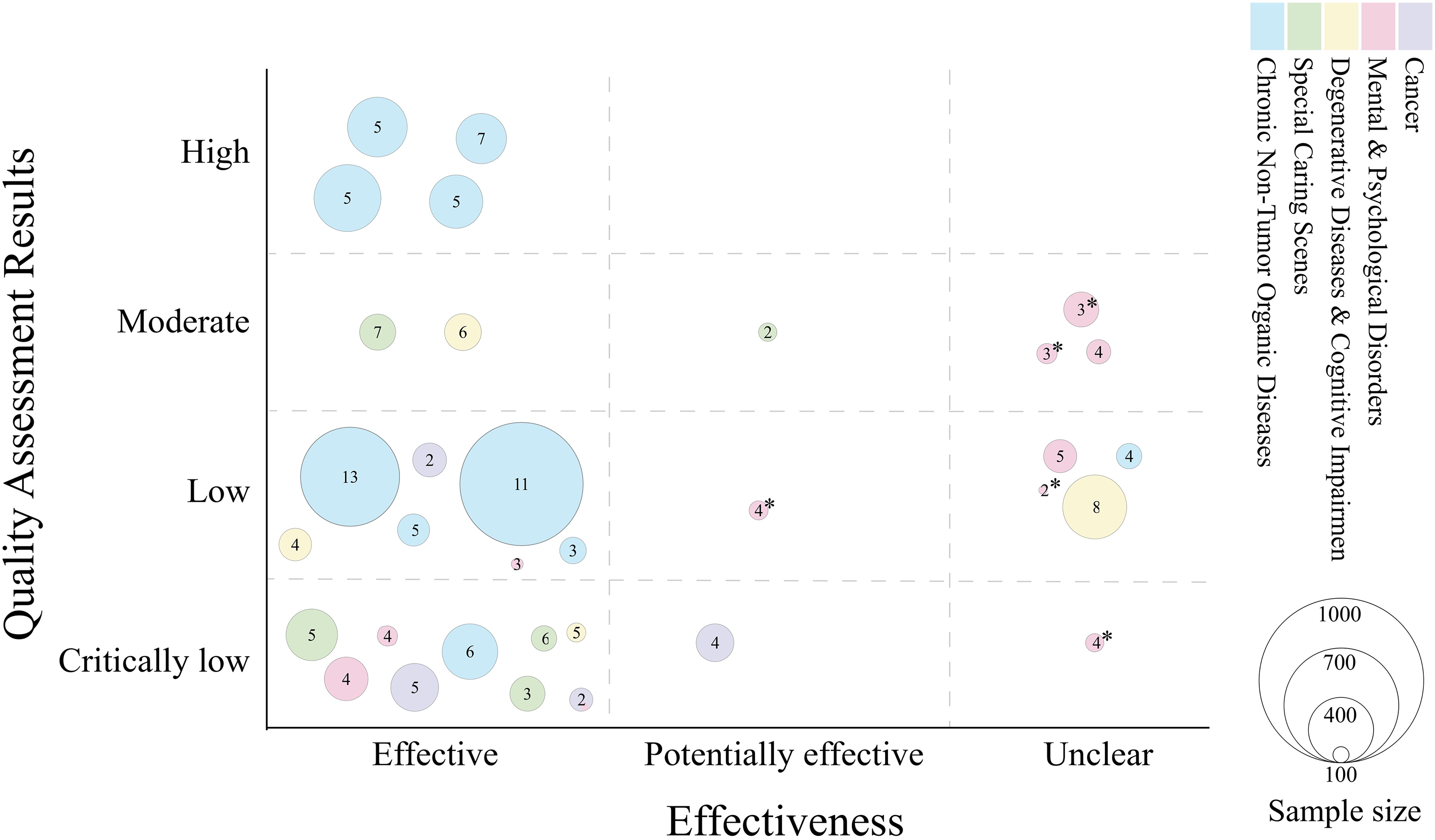
Effectiveness distribution based on AMSTAR-2.
VR interventions have demonstrated generally favorable therapeutic outcomes across diverse populations, including those with chronic medical conditions, cancer patients, and those within special care scenarios. Additionally, positive feedback has also been documented among individuals with degenerative diseases or cognitive impairments. However, the effectiveness of VR interventions for individuals with mental disorders is inconsistent, and it remains unclear how these interventions compare to other active control, such as CBT.
Distribution of effectiveness based on type of VR
Figure 6 presents an analysis of the efficacy of various types of VR in alleviating depressive symptoms across different demographic groups. Of the 33 study outcomes, 11(33.33%) utilized any type of VR, with 10 of these indicating effective or potentially effective results. Non-fully immersive VR was employed in 8 (24.24%) outcomes, 7 of which showed effective or potentially effective results. Fully immersive VR was the most common, used in 14 (42.42%) outcomes, with 8 demonstrating effective or potentially effective outcomes.

Distribution of effectiveness based on type of VR.
In terms of population applications, the use of different types of VR intervention shows some variations. Specifically, any types of VR were more widely used in applications for patients with chronic diseases and special care scenarios. Notably, fully immersive VR was uniformly adopted in research involving cancer patients and also showed a preference in studies focusing on individuals with mental disorders. Whereas studies on patients with degenerative diseases or cognitive impairments more frequently used non-fully immersive VR.
Discussion
Main findings
We analyzed 27 systematic reviews to evaluate the effectiveness of VR interventions in improving depressive symptoms. Our investigation also explored factors influencing efficacy, including population characteristics, the type of VR, and control conditions. Overall, the findings indicate that VR intervention has yielded positive outcomes in improving depressive symptoms among people with chronic diseases, cancer, degenerative diseases, and cognitive disorders and in special care scenarios. However, the effects of interventions on individuals with mental disorders remain ambiguous. Furthermore, the generally low methodological quality of most included MAs raises concerns about potential efficacy biases and may obscure the influence of moderating variables. These results highlight preliminary support for the potential of VR interventions and the critical need for more methodologically rigorous studies to clarify its efficacy across diverse populations.
Population distribution of VR interventions for depression
VR has been employed as a therapeutic intervention to alleviate depression across various populations. However, research in this area has been unevenly distributed, with inadequate attention given to high-risk groups for depression. For instance, while numerous studies are focusing on patients with chronic diseases like stroke and cardiovascular disease, there is a relative scarcity of studies focusing on other high-risk groups, such as individuals with diabetes mellitus. Research on VR interventions for patients with mental disorders have primarily targeted anxiety disorders and post-traumatic stress disorder (PTSD), as confirmed by recent systematic reviews, 54 with comparatively few studies exploring other types of mental disorders. Research in oncology has primarily focused on breast cancer patients, and there is a paucity of studies related to populations at high risk of depression, such as lung cancer. 5 Overall, despite the growing clinical implementation of VR interventions for depression, the research about high-risk populations remains inadequate, necessitating further efforts to enhance the evidence base in this area.
Influences on the effectiveness of VR interventions
The effectiveness of VR interventions in the treatment of depression is influenced by a range of factors, with VR immersion being a key consideration. We discovered that the impact of immersion on treatment effectiveness may be closely associated with the characteristics of the population, instead of the previous simplistic assumption that “the higher the degree of immersion, the more effective it is”. 55 Specifically, non-fully immersive VR has exhibited superior efficacy among patients with chronic and degenerative diseases, as well as cognitive impairments, who are predominantly older adults. This demographic often presents with reduced physiological capabilities and lower adaptability to technology, rendering them more susceptible to the adverse effects associated with fully immersive VR. 56 Additionally, non-fully immersive VR can more easily incorporate physically interactive elements (somatic gaming), which can yield synesthetic advantages by enhancing motor function and improving mood. 57 Conversely, fully immersive VR has consistently demonstrated beneficial outcomes in cancer patients, possibly suggesting that this group may benefit from a higher level of immersion for distraction purposes. Fully immersive VR engages participants in a virtual environment through devices such as HMDs, offering a highly realistic 360-degree audiovisual experience and a strong sense of presence. This immersive environment effectively obstructs external stimuli, enabling participants to temporarily detach themselves from the pain and anxiety of reality, thus alleviating depressive symptoms. 20 Consequently, the characteristics of the patient population should be a critical consideration in the selection of VR types to maximize their effectiveness in the treatment of depression.
Meanwhile, this study found that the effect of improvement in depressive symptoms exhibits a nonlinear relationship with the length of the VR intervention. Notably, interventions lasting 6 weeks or longer are correlated with significant improvements in depressive symptoms. 14 However, the effectiveness of these interventions appears to diminish when the duration exceeds 8–12 weeks. 36 This decline may be attributed to stimulus habituation, a phenomenon in which repeated exposure to the same stimuli leads to diminished neural responses. 58 As a result, participants may become desensitized to the virtual environment, which can reduce the overall efficacy of the intervention. Therefore, effective VR intervention designs should incorporate updates to content or progressive difficulty adjustments to maintain their therapeutic benefits.
Furthermore, VR-related adverse reactions represent a significant factor affecting the effectiveness of treatment. 56 Among the included meta-analyses, VR sickness was the most commonly reported physiological effect, primarily presenting symptoms such as nausea, dizziness and eye fatigue. 27 While non-fully immersive VR showed a reaction incidence of approximately 4.8%, 48 recent studies report low rates of adverse effects in fully immersive settings.59,60 Neuroimaging studies have suggested that these adverse reactions may arise from a mismatch between vestibular and visual information processing. 61 Current evidence indicates VR interventions are generally safe, with physiological effects typically mild and transient. 56 Beyond physical effects, psychological risks warrant careful consideration. During VR experiences, patients may report frustration, confusion, fear, or temporary increases in depressive feelings, 62 potentially related to content or technical limitations. Notably, a theoretical concern involves the contrast between these experiences returning to real life after idealized virtual environments might potentially exacerbate feelings of dissatisfaction or depressive symptoms in vulnerable populations, though empirical evidence remains limited. Beyond these, immediate dissociative symptoms (depersonalization or derealization) after exposure are also frequently reported. 63 These physiological and psychological adverse effects may hinder treatment engagement or exacerbate anxiety, thereby impacting symptom alleviation. Future research should not only evaluate physical symptoms using established measures like the Virtual Reality Sickness Questionnaire (VRSQ), 64 but also systematically assess psychological effects to enhance both safety and therapeutic efficacy.
Scenarios and positioning of VR in depression management
The application of VR interventions demonstrates varying efficacy across diverse clinical settings. The existing body of evidence indicates that VR interventions may surpass passive control conditions (e.g., treatment-as-usual or waitlist) in alleviating depressive symptoms. Nonetheless, a limited number of MAs involving individuals with mental disorders have revealed that VR interventions are comparable to active controls (e.g., CBT) in improving depressive symptoms, without demonstrating a statistically significant difference.26,38,52 This phenomenon may be attributed to the fact that contemporary VR interventions for mental disorders are largely based on exposure therapy, which is recognized as the first-line treatment for anxiety-related disorders, rather than being specifically designed to address depressive symptoms. 65 Moreover, depression encompasses profound psychological issues such as low mood, lack of motivation, and negative thinking. 22 The complexity and variability of depression suggest that VR exposure therapy alone may not adequately target this condition.
Despite a limited role in the treatment of mental disorders, VR interventions have demonstrated considerable advantages in special care scenarios. In settings such as nursing homes, 46 hemodialysis treatments 41 and during natural childbirth, 35 individuals often encounter limitations in mobility and experience monotonous surroundings. VR effectively overcomes these challenges by transcending the limitations imposed by the physical environment. It enables participants to engage with various virtual scenarios without leaving their actual location, freeing them from the physical limitations of their bodies and surroundings. Further, VR can adapt intervention content to individual needs, provide immersive audiovisual experiences, and reduce negative stimuli in the real environment by fostering positive emotions or redirecting attention. This adaptability contributes to reducing anxiety and depression. 20 The personalized design and immersion of VR also counteract the monotony of traditional therapies, which in turn enhances participant satisfaction and treatment adherence. 55
In addition, the included MAs demonstrate diverse applications of VR in interventions for depressive symptoms. VR can serve not only as an adjunct tool integrated with established psychological interventions like exposure therapy and CBT to enhance therapeutic effects through virtual environments,26,37,38,47 but also as a stand-alone intervention utilizing virtual experiences such as natural landscapes, games, and meditation practices to improve depressive symptoms.35,48,49 This flexibility, which is brought about by individualized adjustments and a variety of application formats, enables adaptation to a wide range of clinical settings. On the other hand, such diversity in intervention design also complicates the evaluation of efficacy. Given the varied implementations of VR across different scenarios, future research should prioritize investigating its potential as either a complementary or alternative approach to established effective interventions, particularly in contexts that are challenging to address with traditional treatments to determine the optimal role of VR in the management of depression. For VR to realize its full potential across these diverse scenarios, broader implementation must consider several key issues, including physiological and psychological adverse reactions, technological barriers, and ethical concerns (e.g., data privacy and informed consent for vulnerable populations).
Limitations and strengths
This study acknowledges several limitations that warrant consideration. First, more than 80% of the included MAs exhibited low methodological quality. Furthermore, potential duplication of included studies across different MAs, may affect the overall reliability of our findings. Secondly, the declining trend in annual original research publications after 2020, as indicated by existing meta-analyses, may not fully reflect the true dynamics of this field due to potential confounding factors such as search time lag and inherent publication bias in the source data. Third, the limited depth of the evidence mapping analysis hindered the ability to refine the specific effects of various types of VR, application forms, and control conditions on treatment efficacy. Finally, the inclusion of only MAs published in Chinese and English imposes certain limitations on the generalizability and replicability of the findings.
Despite these limitations, the findings of this study are notably insightful and offer practical guidance. A major strength of the research is its extensive and up-to-date analysis, integrating data from 27 MAs and 129 independent original studies (totaling 6639 participants), with over half of the original studies published from 2020 onwards. Moreover, the study utilized various visualization tools to effectively present the results and enhance clarity. This comprehensive synthesis not only confirms VR's positive effects on depressive symptoms but also identifies key research gaps and influencing factors, providing a significant scientific foundation and practical recommendations for the implementation of VR in managing depressive symptoms.
Conclusion
In conclusion, this study affirms the therapeutic potential of VR for depression across diverse populations. Despite promising findings, existing research also highlights several key limitations and knowledge gaps, including a scarcity of intervention studies targeting high-risk populations, insufficiently delineated roles of VR in diverse clinical contexts, and an incomplete understanding of how various factors influence VR outcomes and their underlying mechanisms. Future research should address these gaps by exploring optimal VR implementation strategies for depression management, clarifying its potential as a complementary or alternative treatment, and ultimately enhancing its broader clinical application.
Supplemental Material
sj-pdf-1-dhj-10.1177_20552076251390555 - Supplemental material for The effectiveness of virtual reality to improve depression: A systematic evidence map
Supplemental material, sj-pdf-1-dhj-10.1177_20552076251390555 for The effectiveness of virtual reality to improve depression: A systematic evidence map by Xiao Lu, Jiaxin You, Tian Xia, Yan Huang and Rong Xu in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251390555 - Supplemental material for The effectiveness of virtual reality to improve depression: A systematic evidence map
Supplemental material, sj-docx-2-dhj-10.1177_20552076251390555 for The effectiveness of virtual reality to improve depression: A systematic evidence map by Xiao Lu, Jiaxin You, Tian Xia, Yan Huang and Rong Xu in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076251390555 - Supplemental material for The effectiveness of virtual reality to improve depression: A systematic evidence map
Supplemental material, sj-docx-3-dhj-10.1177_20552076251390555 for The effectiveness of virtual reality to improve depression: A systematic evidence map by Xiao Lu, Jiaxin You, Tian Xia, Yan Huang and Rong Xu in DIGITAL HEALTH
Footnotes
Ethical considerations
The study did not require ethical approval and complied with the journal's ethics policy as it was based on analysis of existing literature and did not involve new data collection or human participants.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contributions
Authors XL, JX, TX, YH, and corresponding author RX collectively contributed to this study. XL, with assistance from JX and TX, designed the methodology, conducted literature screening and data extraction, performed statistical analysis, created figures and tables, and drafted the manuscript. YH handled data curation and verification and participated in quality assessment. RX conceptualized the study, supervised the research process, and reviewed and edited the manuscript. All authors participated in the final review and approved the manuscript for publication.
Funding
This work was funded by the Nursing Special Fund (Major Project) of Tongji Hospital, Tongji Medical College of Huazhong University of Science and Technology (Grant No.2023C08).
Declaration of conflicting interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Declaration of AI use
During the preparation of this work, ChatGPT was utilized for language polishing and grammatical refinement. After using this tool, all content was reviewed and edited by the authors, who take full responsibility for the published work.
Data availability statement
The datasets used in this study are publicly available. All information was obtained from the articles cited in the manuscript and can be accessed from the publications.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.